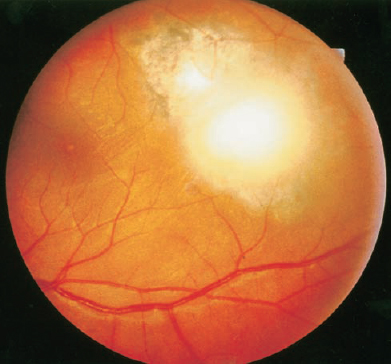
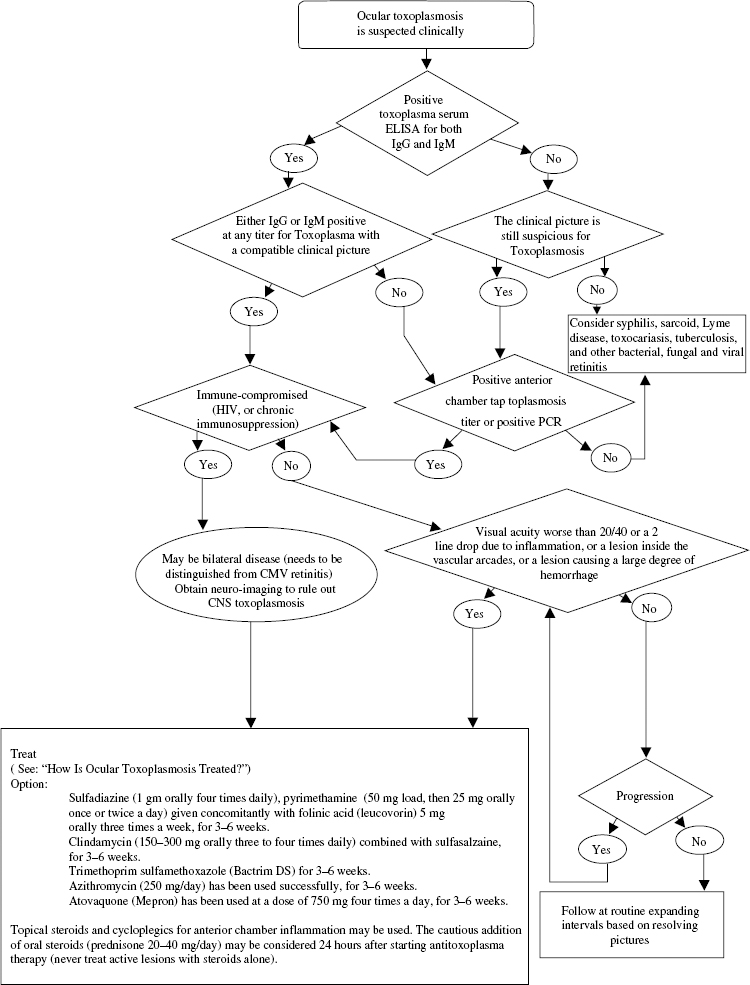
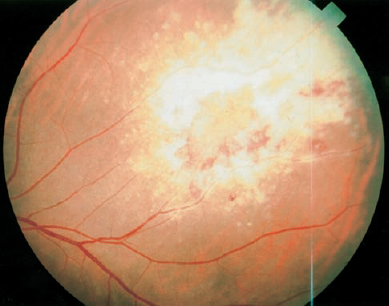
SECTION IV Toxoplasma gondii is an obligate intracellular protozoan. The parasite is found all over the world. Members of the cat family are the definite host. The oocysts are found uniquely in the intestinal mucosa of cats.1 The oocysts are excreted and released into the environment. Humans become infected directly by ingesting oocysts or indirectly by ingesting tissue cysts present in undercooked meat from infected animals (pork, lamb, or chicken and rarely beef). The cysts release tachyzoites, which are the active infectious form that can travel to the muscle and neural tissue, including the retina. The tachyzoites also may pass through the placenta to the fetus. The latent form of T. gondii is the tissue cyst (bradyzoite), which contains hundreds of thousands of organisms. The organism can remain dormant in the tissue cysts for many years, and its release is responsible for the recurrent nature of the ocular disease.1 Toxoplasmosis is very common. At least 50% of the adult population has been exposed to Toxoplasma as evident by a positive antibody titer.2 The incidence of a positive titer increases with age. In the United States, about 2 to 6 per 1000 women acquire the infection during pregnancy, with about 40% risk of transmitting the infection to the fetus. Previously, most cases of ocular toxoplasmosis were felt to be due to congenital infection; however, there is evidence, particularly in Brazil, that acquired toxoplasmosis accounts for most of the cases of ocular toxoplasmosis.3 Overall, ocular toxoplasmosis accounts for nearly one third of all cases of posterior uveitis. Acquired toxoplasmosis in the non-immune-compromised adult is frequently asymptomatic. The most common manifestation is lymphadenopathy (90%) followed by fever, malaise, and sore throat. More severe disease can occur, affecting muscle, skin, brain, heart, and kidney. In the immunocompromised host, in particular acquired immunodeficiency syndrome (AIDS) patients, the disease can be a fulminant central nervous system disease that rapidly leads to death. About 1 per 1000 newborns becomes infected.2 The earlier the disease is acquired in pregnancy, the greater the risk to the fetus. In neonates, the disease occurs in a clinical spectrum ranging from no signs or symptoms to bilateral retinochoroiditis, seizures, and intracranial calcifications. The presence of immunoglobulin M (IgM) antibodies against toxoplasmosis confirms the diagnosis. In many of the asymptomatic cases, ocular lesions are not present at birth and develop later. Ocular toxoplasmosis is a unilateral disease in most cases. Most symptomatic cases are due to reactivation of the disease due to release of tachyzoites from dormant tissue cysts in the retina. The characteristic finding is a cream-colored retinal lesion (satellite lesion) adjacent to an old atrophic chorioretinal scar (Fig. 18–1). Cells are found in the vitreous, particularly overlying the active lesion. Adjacent to the active retinitis one may see hemorrhage and sheathing of the retinal blood vessels. Anterior chamber cells can be seen and may appear as granulomatous or, less commonly, as nongranulomatous uveitis. The intraocular pressure may become elevated during active inflammation. FIGURE 18–1. An old pigmented scar with an adjacent more active lesion in a patient with ocular toxoplasmosis. In cases where the vitreous haze and cellular reaction are profound, patients become symptomatic. The most common symptoms are blurriness and floaters. Rarely, if the lesions involve the macula, optic nerve, or the vascular arcades, the patient can experience profound loss of vision. The diagnosis of ocular toxoplasmosis is primarily clinical and is based on the typical ocular features. Serologic evidence of Toxoplasma infection is important to document exposure to the organism. The presence of IgG antibody at any titer even in undiluted serum (1:1) is considered positive. IgM antibodies suggest recent infection. A negative titer is evidence against the diagnosis and should alert the physician to other diagnoses. The type of serologic testing that is most reliable is still debatable, although the enzyme-linked immunosorbent assay (ELISA) is recommended by many. The Sabin-Feldman dye test requires live organisms and is used less frequently. It is important to realize that a positive antibody titer, which may be seen in nearly half of all adults, only indicates previous exposure and should be interpreted based on other clinical findings. Serologic examination of the aqueous or detection of the Toxoplasm a DNA by polymerase chain reaction (PCR) also has been used to determine specifically ocular infection in patients with positive serum antibodies. The differential diagnosis includes other causes of infectious retinitis, such as tuberculosis, toxocara, syphilis, cytomegalovirus, Candida organisms, and herpes simplex. Other causes of uveitis, such as sarcoidosis, also may manifest in a similar fashion. All patients with suspected ocular toxoplasmosis should also have their human immunodeficiency virus (HIV) status determined. If the patient is HIV positive, an evaluation of the central nervous system is mandatory. In immune-competent patients, the disease is self-limited. The natural history of a reactivated ocular lesion is resolution by 6 weeks to 6 months. Peripheral lesions without significant inflammation are generally observed and not treated. Treatment is recommended in all the following situations (Fig. 18–2): (1) there is a lesion within the temporal arcade, (2) a lesion is abutting the optic nerve or threatening a large retinal vessel, (3) a lesion has induced a large degree of hemorrhage, or (4) a lesion has induced enough vitreal inflammation to reduce the vision to below 20/40 (or a two-line drop from baseline). Several regimens can be used to treat ocular toxoplasmosis. The most common drug combination is sulfadiazine (1 g orally four times daily), pyrimethamine (50-mg load, then 25 mg orally once or twice a day) given concomitantly with folinic acid (leucovorin) 5 mg orally three times a week. A baseline blood count and platelet count should be obtained and repeated on a weekly basis while the patient receives pyrimethamine. Prednisone is judiciously added at a dose of 20 to 40 mg per day, beginning 12 to 24 hours after initiating specific antimicrobial therapy. Corticosteroids never are prescribed alone and never are administered by periocular injection. Topical corticosteroids and cycloplegics are used adjunctively in patients with anterior chamber reaction. Alternative regimens include clindamycin (150 to 300 mg orally three to four times daily) combined with sulfasalazine. Psuedomembranous colitis is a concern with clindamycin use. Trimethoprim-sulfamethoxazole (one double-strength twice daily) also has been used with success. Likewise, azithromycin (250 mg daily) has been used successfully. Most recently, atovaquone (Mepron) has been used at a dose of 750 mg four times a day. In all regimens, systemic treatment typically is given for 3 to 6 weeks. It is important to realize that all these regimens are targeting the tachyzoites (the active infectious form) and generally do not affect the tissue cyst. Although atovaquone has proven to be cysticidal in vitro, it remains to be seen clinically whether it can eradicate the organism. Therefore, toxoplasmosis can recur even after treatment because the tissue cysts generally survive. In patients with multiple recurrences, long-term prophylactic therapy with the preceding agents may reduce the likelihood of reactivation. Infectious endophthalmitis can be divided into exogenous and endogenous types. In exogenous infections, the organism enters the eye from the external environment. The subtypes of exogenous endophthalmitis include postoperative, traumatic, and bleb-associated. In endogenous endophthalmitis, the organism reaches the eye through the vascular system. Acute postoperative endophthalmitis is primarily a bacterial disease. The sources of bacteria are usually the eyelids and conjunctiva. The incidence is 0.1 to 0.4%.4,5 Wound problems appear to be an important contributing factor. Most cases occur within 3 to 7 days after surgery but may occur up to two weeks. Pain, decreased vision, conjunctival hyperemia, anterior uveitis with fibrin, hypopyon, and vitreitis are the characteristic features of acute bacterial endophthalmitis. The most common organisms isolated are Staphylococcus epidermidis, followed by S. aureus, Streptococcus species, and gram-negative organisms, such as Serratia marcescens, and Pseudomonas species. The treatment of acute postoperative endophthalmitis was the subject of the Endophthalmitis Vitrectomy Study (see Chapter 22‘s Fig. 22-2).6 This study found that cases in which the visual acuity at presentation is better than light perception could be managed with vitreous tap and injection of intravitreal antibiotics. On the other hand, in cases where the visual acuity is light perception only, the visual outcome was better if immediate pars plana vitrectomy and injection of antibiotics were performed. The combination of vancomycin and ceftazidime is the most common choice of antibiotics for intravitreal injection. Whereas systemic corticosteroids may be useful for reducing intraocular inflammation, systemic antibiotics were not shown to be beneficial. The role of intravitreal corticosteroid injection remains controversial. Chronic postoperative endophthalmitis begins more than 2 weeks after surgery. It typically presents as a chronic uveitis that can be partially suppressed with topical corticosteroids. The visual acuity is usually good. One of the most common organisms responsible for chronic postoperative endophthalmitis is Propionibacterium acnes.7 The typical patient with P. acnes presents with chronic low-grade anterior segment inflammation that starts from 2 months to 2 years after surgery. White plaques composed of bacteria are often seen between the intraocular lens and the posterior capsule. S. epidermidis, which typically presents 6 weeks after surgery, can also cause a chronic postoperative endophthalmitis. Likewise, fungal endophthalmitis, most commonly due to Candida species, may present at 3 months after surgery. Besides the clinical features, the diagnosis is primarily based on culture data. In case of P. acnes, it is important to inform the microbiology laboratory not to discard the cultures after the usual 3 to 4 days. Because the organism is slow growing, cultures should be maintained for 14 days. Chronic postoperative endophthalmitis caused by S. epidermidis can be treated successfully with intravitreal injection of vancomycin. Therapy for P. acnes endophthalmitis usually involves a combination of vitrectomy, posterior capsulectomy, and intravitreal vancomycin. Although the intraocular lens does not need to be removed at the time of initial therapy, recurrent cases are managed with repeat intravitreal antibiotics and removal of residual posterior capsule and intraocular lens. The treatment for fungal endophthalmitis is discussed later herein. Fungal infections can be exogenous (postsurgical or posttraumatic) or endogenous. Fungal endophthalmitis usually presents as a chronic pan-uveitis. Fluffy deep yellow–white retinal or choroidal lesions are frequently present, and the vitreous often contains “fluff balls.” The patient may not be symptomatic for days or even months until he or she develops blurred vision or floaters. Later in the course, redness, pain, hypopyon and dense vitreitis may occur. Candida species are the most common organisms responsible for endogenous (as well as exogenous) fungal endophthalmitis. Candida endophthalmitis usually occurs in chronically ill patients with an indwelling catheter. It is also a frequent complication of intravenous drug use. Aspergillus species are the second most common cause of endogenous fungal endophthalmitis. Table 18–1 summarizes the features of the more common organisms that can lead to fungal endophthalmitis.
The Inflamed Eye and Retinal Disease
18
Infectious Uveitis
Toxoplasmosis
What Is the Life Cycle of Toxoplasma gondii?
What Is the Epidemiology of Toxoplasmosis?
What Are the Manifestations of Acquired Toxoplasmosis?
What Are the Manifestations of Congenital Toxoplasmosis?
What Are the Typical Signs and Symptoms of Ocular Toxoplasmosis?
How Is Ocular Toxoplasmosis Diagnosed?
What Is the Differential Diagnosis of Ocular Toxoplasmosis?
When Should Ocular Toxoplasmosis Be Treated?
How Is Ocular Toxoplasmosis Treated?
Why Does Toxoplasmosis Recur?
Endophthalmitis
What Are the Various Types of Infectious Endophthalmitis?
What Are the Features of Acute Postoperative Endophthalmitis?
How Is Acute Postoperative Endophthalmitis Treated?
What Are the Features of Chronic Postoperative Endophthalmitis?
How Is Chronic Postoperative Endophthalmitis Diagnosed?
How Is Chronic Postoperative Endophthalmitis Treated?
What Are the Characteristics of Fungal Infections?
| Organism | Risk Factor | Ocular Features |
|---|---|---|
| Candida sp. | IV drug use, chronic IV therapy, surgery | Yellow–white chorioretinal lesions, vitreous fluff balls |
| Aspergillus sp. | IV drug use, immunosuppression, surgery | Yellow–white chorioretinal lesions, vitreous fluff balls |
| Cryptococcus neoformans | Immunocompromised, lymphoma | Yellow–white chorioretinal lesions, often with meningitis |
| Blastomyces dermatitidis | Systemic blastomycosis | Panuveitis |
| Coccidioides immitis | Southwest United States | Punched out choroidal lesions, yellow chorioretinal lesions |
IV, intravenous.
Modified from Nussenblatt RB, Whitcup SM, Palestine AG. Uveitis: Fundamentals and Clinical Practice, 2nd ed. St. Louis: Mosby–Year Book; 1996, with permission
How Is Fungal Endophthalmitis Treated?
For exogenous infections that are limited to the eye, vitrectomy combined with intravitreal amphotericin B is the mainstay of therapy. Oral fluconazole or ketoconazole also may be beneficial. Endogenous endophthalmitis requires systemic amphotericin B along with intravitreal amphotericin B.
What Are the Organisms Associated with Posttraumatic Endophthalmitis?
Posttraumatic endophthalmitis can develop after penetrating injuries. The most common organisms are S. epidermidis, Bacillus cereus, S. aureus, and fungi. Endophthalmitis due to B. cereus characteristically has a very fulminant course with rapid progression.
What Are the Characteristics of Bleb-Associated Endophthalmitis?
Infection after filtering surgery is one of the morbidities associated with this procedure. The use of antifibrotic agents, the presence of bleb leaks, and the inferior location of the bleb are among the main risk factors for developing endophthalmitis. Typically, these infections occur late and are preceded by conjunctival injection and discharge. The most common organisms are Streptococcus species (including pneumococcus) and Haemophilus influenza. Treatment includes vitreous cultures, intravitreal antibiotics, and vitrectomy for the more severe cases.
Cytomegalovirus Retinitis
What Is the Epidemiology of Cytomegalovirus Retinitis?
Cytomegalovirus (CMV) is a double-stranded DNA virus in the herpes class that causes an asymptomatic or mononucleosis-like syndrome in healthy adults. More than half of all adults have evidence of previous CMV infection. CMV infection of the retina occurs as an opportunistic infection only in immunosuppressed persons or in infants with congenital infection. In the past, chemotherapy and organ transplantation, particularly of the kidneys, were the most common causes of CMV retinitis. In the current era, however, AIDS has led to a significant rise in the number of cases of CMV retinitis. Most recently, the number of new cases of CMV retinitis has declined significantly with the introduction of highly active antiretroviral therapy (HAART).
How Common Is Cytomegalovirus Retinitis in the AIDS Population?
In AIDS patients, CMV retinitis is the most common ocular complication. It probably occurs clinically in 15 to 20% of these patients at some time.8 It typically occurs when the CD4 count reaches below 50 cells per microliter, and it is rarely seen if the CD4 is greater than 100 cells per microliter. The introduction of potent antiretrovirals has led to a dramatic decline in the incidence of CMV retinitis; nonetheless, new cases of CMV are still emerging in patients for whom HAART fails.
What Is HAART?
A combination of several antiretroviral agents, HAART has been highly effective in reducing the number of HIV particles in the bloodstream (as measured by the viral load) and more importantly in increasing the CD4-positive T-lymphocyte count. The typical regimen involves one protease inhibitor and two nucleoside reverse transcriptase inhibitors.
What Is the Typical Presentation of CMV Retinitis?
Cytomegalovirus retinitis begins as small white retinal infiltrates that if seen early may resemble a cotton-wool spot. Two types of clinical appearance may be seen.1 The typical presentation is a perivascular fluffy white lesion with many scattered hemorrhages. The other presentation is a granular-appearing lesion that has few associated hemorrhages and often has a central area of clearing with atrophic retina and stippled retinal pigment epithelium (Fig. 18–3). The latter presentation is seen more typically in the peripheral retina. Occasionally, it may present with periphlebitis (frosted-branch angiitis). There is usually a low-grade vitreitis associated with CMV retinitis, and there may be fine anterior-chamber keratic precipitates. Vision is normal unless the optic nerve or fovea is involved. CMV retinitis typically presents in one eye first, with the other eye becoming involved several months later.
How Does Cytomegalovirus Retinitis Progress?
Cytomegalovirus retinitis progresses in two ways. New lesions may form that are not physically near an old lesion, probably by hematogenous spread. Second, and most common, an old lesion spreads at its borders to involve a new, previously uninfected retina. The rate of progression is approximately 250 μ per week. In assessing the progression of CMV retinitis, it is important to pay attention to the border of the lesion and look for advancement or new lesions. Clearing at the center of the lesion should not be interpreted as improvement because the whiteness will gradually decrease as the retina becomes atrophic.
Visual loss from CMV retinitis may occur in several ways. Most commonly, the infected retina develops an absolute scotoma due to retinal necrosis. As the macula is involved, the central vision is lost. In some patients, paramacular CMV will produce macular edema, which is a reversible cause of visual loss if it can be treated before the active virus progresses through the fovea. The optic disc can also be involved with severe loss of vision. Last, the retina can develop a rhegmatogenous retinal detachment because there is vitreous traction on the thin, atrophic retina.
How Often Do Patients with Cytomegalovirus Retinitis Develop a Retinal Detachment, and How Is It Treated?
Retinal detachment develops in about 20% of patients with retinitis; 50% of these patients develop detachment in the second eye if there is retinitis. The greater the degree of peripheral retinal involvement, the greater the risk of retinal detachment. The mechanism of detachment in CMV retinitis is vitreous traction on the thinned, atrophic retina. Multiple retinal breaks are usually present, and large relatively posterior breaks can be seen.
The surgical treatment can be challenging. Scleral buckling is appropriate when the breaks are located near the vitreous base. In CMV retinitis, however, these breaks tend to be more posterior. A more effective approach is vitrectomy, endolaser, and the use of a long-lasting retinal tamponade, namely, silicone oil. Silicone oil significantly reduces the risk of redetachment. The silicone oil typically is left in place as long as the patient is at risk for CMV.
Laser also has been used to demarcate areas of retinitis and thereby prevent detachment. This approach is not uniformly successful, and the retinitis can progress through the laser burns.
What Are the Drug Treatments Available for Treating Cytomegalovirus Retinitis?
The most important and effective treatment for the long-term control of CMV retinitis is appropriate anti-retroviral therapy, which can increase the number of circulating CD4 cells and allow the patient’s own immune system to contain CMV. For the acute treatment of CMV retinitis, however, numerous of medications are available.
GANCICLOVIR
Oral ganciclovir, which has a low bioavailability, can be used for maintenance therapy as an alternative to intravenous ganciclovir. The typical dose is 3 to 6 g per day. The main advantage of oral administration is that it eliminates the need for long-term intravenous catheter and related complications.
Alternatively, ganciclovir may be injected directly into the vitreous at a dose of 2 mg in 0.1 mL. Therapeutic levels are maintained for 62 hours; thus, two injections per week must be given. This will result in long-term remission. This approach is useful when systemic therapy is not possible because of neutropenia. With repeated injections, the risk of vitreal hemorrhage, infection, and retinal detachment increases. In addition, intravitreal therapy does not treat possible systemic infections with CMV, such as CMV colitis. A novel approach to intravitreal therapy is the use of the ganciclovir implant (VITRASERT) (Fig. 18–4). This is a slow-release device that lasts about 8 months. It is surgically implanted through the pars plana. It provides the most effective therapy for the control of local disease; however, it does not prevent CMV retinitis in the fellow eye or prevent extraocular CMV infections. Martin and colleagues reported that patients treated with an implant alone are also at a significantly greater risk for developing Kaposi sarcoma compared with those who additionally received oral or systemic ganciclovir at maintenance doses.9 Therefore, patients not receiving potent antiretrovirals should simultaneously receive systemic ganciclovir (or valganciclovir) in addition to an implant.
VALGANCICLOVIR
An oral prodrug of ganciclovir, valganciclovir, was approved for use as both induction and maintenance therapy. Oral valganciclovir is rapidly absorbed and hydrolyzed to ganciclovir. The oral bioavailability of ganciclovir after oral valganciclovir administration is high. Oral valganciclovir 900 mg provides a daily exposure of ganciclovir comparable to that of intravenous ganciclovir 5 mg/kg. A single, randomized, nonblinded study indicated that oral valganciclovir (900 mg twice daily for 3 weeks, then 900 mg once daily) and intravenous ganciclovir (5 mg per kilogram of body weight twice daily for 3 weeks, then 5 mg/kg once daily) were equally effective in the treatment of newly diagnosed CMV retinitis in 160 patients with AIDS.10 Valganciclovir appears to have a similar tolerability profile to intravenous ganciclovir during induction duction therapy in patients with AIDS and newly diagnosed CMV retinitis.




