 Iris Cysts
Iris CystsIris Cysts
Iris cysts can assume any of several clinical variations (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16). Their classification, clinical features, pathology, and management are summarized briefly here. Our classification of iris cysts is as follows (1):
Primary cysts
Cysts of the iris pigment epithelium
Central (pupillary)
Midzonal (retroiridic)
Peripheral (iridociliary)
Dislodged
Anterior chamber
Vitreous chamber
Cysts of the iris stroma
Congenital
Acquired
Secondary cysts
Epithelial cysts
Epithelial downgrowth cysts
Postsurgical
Posttraumatic
Pearl cysts
Drug-induced cysts
Parasitic cysts
Cysts of the Iris Pigment Epithelium
General Considerations
Iris pigment epithelium (IPE) cysts can be divided anatomically into central, midzonal, peripheral, and dislodged types (1,2).
Central (Pupillary) Cysts. Pupillary cysts can be solitary or multiple. The solitary type is nonfamilial and appears as a round, dark-brown lesion at the pupillary border. The multiple variant is usually sporadic but can be autosomal dominant. It is usually bilateral and is characterized by variable-sized, dark-brown lesions that may encircle the pupil. They often spontaneously collapse and then re-form, producing irregular, wrinkled lesions known as iris flocculi. Even when extensive, they rarely cause visual impairment, and most remain relatively stable throughout the patient’s life (1, 2, 3, 4, 5, 6, 7). Although there are usually no systemic associations, one family had iris flocculi and dissecting aortic aneurysm (5).
Midzonal (Retroiridic) Cysts. The midzonal cyst is usually discovered on routine slit lamp biomicroscopy as a round or fusiform, smooth, dark-brown lesion at the pupillary margin. It can be unilateral or bilateral, solitary or multiple. With pupillary dilation, it becomes more elongated, and its central border sometimes rolls anteriorly over the papillary margin, findings that help to differentiate it from a ciliary body melanoma. Like a melanoma, it blocks the transmission of light.
Iridociliary (Peripheral) Cysts. The more common peripheral cyst is usually unilateral and more common in young women. It presents as an asymptomatic, localized, anterior bulge of the iris stroma, usually on the temporal side, that is noted coincidentally on slit lamp biomicroscopy. With the pupil widely dilated, the cyst can sometimes be visualized with slit lamp biomicroscopy and gonioscopy, and it tends to transmit light because it is partially covered by nonpigmented ciliary epithelium. More often, however, ultrasound biomicroscopy (UBM) is necessary to better demonstrate the lesion. In contrast, a tumor shows a solid pattern, and a cavitary melanoma would appear cystic but would have a thicker wall.
Dislodged Iris Pigment Epithelium Cysts. Any IPE cyst can become dislodged and float freely in the vitreous or anterior chamber (9,16). Free-floating cysts can eventually become fixed in the anterior chamber angle. Unlike melanoma in the angle, a fixed cyst has sharp abrupt borders rather than gradual sessile borders. UBM is an excellent method for the recognition of all types of iris cysts.
Pathology
Each of the IPE cysts is lined by a monolayer of IPE cells and usually has clear fluid in the lumen.
Management
None of the IPE cysts requires treatment, except for the rare occasion in which the lesion covers the entire pupil. Even then, pupillary dilation may allow vision and avoid surgery or laser disruption of the lesion, which are rarely necessary.
Selected References
1. Shields JA. Primary cysts of the iris. Theses, American Ophthalmological Society. Trans Am Ophthalmol Soc 1981;79:771-809.
2. Shields JA, Kline MW, Augsburger JJ. Primary iris cysts. Review of the literature and report of 62 cases. Br J Ophthalmol 1984;68:152-166.
3. Shields CL, Shields JA, Cook GR, et al. Differentiation of adenoma of the iris pigment epithelium from iris cyst and melanoma. Am J Ophthalmol 1985;100:678-681.
4. Shields JA, Shields CL. Melanocytic tumors of the iris stroma. Primary iris cyst. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:78.
5. Lewis RA, Merin LM. Iris flocculi and familial aortic dissection. Arch Ophthalmol 1995;113:130-131.
6. Lois N, Shields CL, Shields JA, et al. Primary cysts of the iris pigment epithelium: clinical features and natural course in 234 patients. Ophthalmology 1998;105:1879-1885.
7. Shields JA, Shields CL, Lois N, et al. Iris cysts in children: classification, incidence, and management. The 1998 Torrence A Makley Jr Lecture. Br J Ophthalmol 1999;83:334-338.
8. Sallo FB, Hatvani I. Recurring transitory blindness caused by primary marginal pigment epithelial iris cysts. Am J Ophthalmol 2002;133:407-409.
9. Shields JA, Shields CL, De Potter P, et al. Free-floating cyst in the anterior chamber of the eye. J Pediatr Ophthalmol Strabismus 1996;33: 330-331.
10. Obata R, Suzuki S, Numaga J, et al. Congenital iris bombe induced by large iris cysts. Arch Ophthalmol 2003;121:906-907.
11. Shields JA, Shields CL, Mercado G, et al. Adenoma of the iris pigment epithelium: a report of 20 cases: the 1998 Pan-American Lecture. Arch Ophthalmol 1999;117:736-741.
12. Verma L, Venkatesh P, Sen S, et al. Surgical removal of a free floating cyst of the iris pigment epithelium causing disturbing visual symptoms. Ophthalmic Surg Lasers 1999;30:223-225.
13. Kozart DM. Echographic evaluation of primary cysts of the iris pigment epithelium. Am J Ophthalmol 1996;121:100-101.
14. Alward WL, Ossoinig KC. Pigment dispersion secondary to cysts of the iris pigment epithelium. Arch Ophthalmol 1995;113:1574-1575.
15. Lai IC, Kuo MT, Teng LM. Iris pigment epithelial cyst induced by topical administration of latanoprost. Br J Ophthalmol 2003;87:366.
16. Lally DR, Shields JF, Shields CL, et al. Free floating vitreous cyst of pigment epithelial origin. J Pediatr Ophthalmol Strabismus. In press.
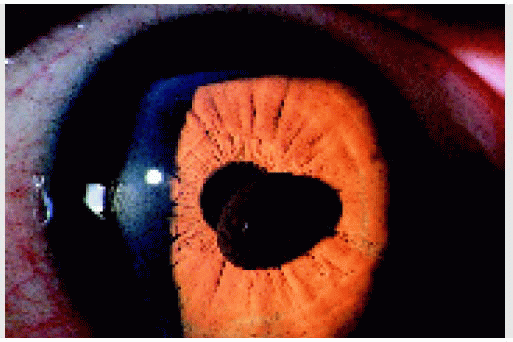
▪ Iris Pigment Epithelial Cyst: Pupillary (Central) Type
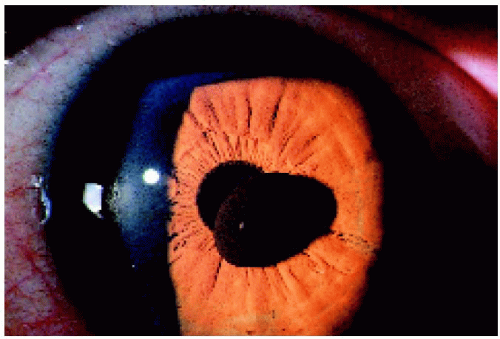 Figure 4.1. Large solitary pupillary margin iris pigment epithelial cyst in a 38-year-old man. The lesion had been present and relatively stable since early childhood. |
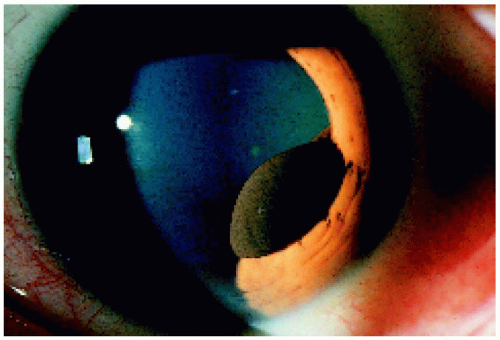 Figure 4.2. Lesion shown in Figure 4.1 after pupillary dilation. Note that the lesion has now been pulled more into the pupillary aperture, and its margin rolls anteriorly over the edge of the pupil. |
 Figure 4.3. Pupillary margin iris pigment epithelial cyst that has collapsed and has a flocculent appearance in a 25-year-old man. |
 Figure 4.4. Left eye of an 18-year-old man with bilateral multiple pupillary margin iris pigment epithelial cysts (iris flocculi). The lesions were noticed shortly after birth and remained relatively stable for 30 years of follow-up. |
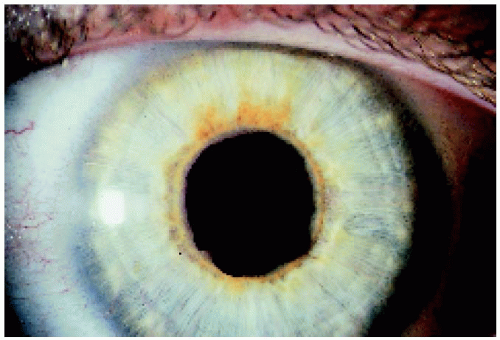 Figure 4.5. Right eye of the patient depicted in Figure 4.4, showing a similar appearance of the left eye. |
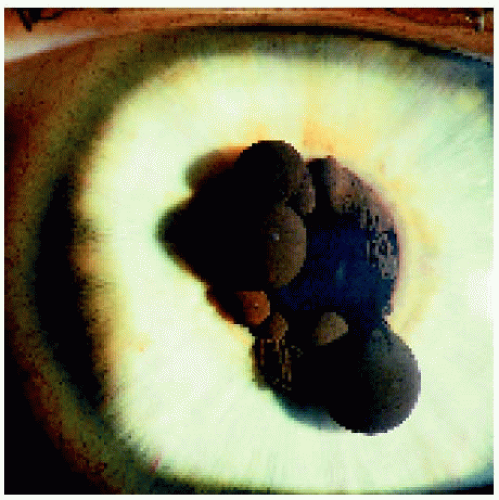 Figure 4.6. Right eye of the same patient 9 years later. Note that the configuration of the lesions changed, with some cysts collapsing and others becoming enlarged. The left eye underwent similar changes. The lesions were noticed shortly after birth, remained relatively stable for 30 years of follow-up, and required no treatment. |
▪ Iris Pigment Epithelial Cyst: Midzonal (Retroiridic) Type
A midzonal iris pigment epithelial cyst can resemble an iris or ciliary body melanoma. However, a melanoma would not ordinarily arise from the back surface of the iris and overhang the pupillary margin. In addition, the midzonal cyst becomes stretched with pupillary dilation, which would not occur with a melanoma. In contrast to a peripheral IPE cyst (discussed subsequently), a midzonal cyst tends to block transmission of light.
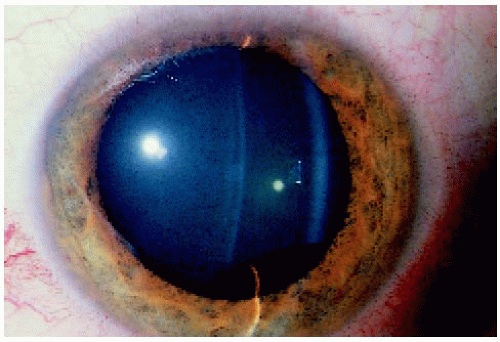 Figure 4.7. Slit lamp appearance, using a slit beam, of a midzonal iris pigment epithelial cyst inferiorly in a 40-year-old man.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|