Purpose
To assess the effects of intravitreal bevacizumab injections in the treatment of nonsubfoveal choroidal neovascularization (CNV) associated with angioid streaks (AS) in a 3-year follow-up study.
Design
Noncomparative, interventional, prospective case series.
Methods
Eighteen patients (18 eyes) with juxtafoveal/extrafoveal CNV secondary to AS were recruited. All patients underwent a complete ophthalmologic examination, including best-corrected visual acuity (BCVA) measurement on ETDRS chart, optical coherence tomography (OCT), and fluorescein angiography (FA). The protocol treatment included a first injection, followed by repeated injections on the basis of detection of new hemorrhage, any type of fluid on OCT, and/or presence of FA leakage. Primary outcome measures were final mean changes in BCVA and proportion of eyes with 10 ETDRS letters improvement. Secondary outcomes were mean changes of central macular thickness (CMT) and foveal involvement.
Results
After a mean BCVA stabilization over the first year, a statistically significant BCVA worsening was registered at the 24-month (72.8 ± 10.0 ETDRS letters, P = .03) and 36-month examinations (65.8 ± 15.0 ETDRS letters, P = .02) in comparison with the 1-year visual outcomes (80.1 ± 5.4 ETDRS letters); lastly, a substantial stabilization in the BCVA was observed at 36 months in comparison with the baseline value (77.9 ± 10.0 ETDRS letters, P = .22). Two eyes (25%) with juxtafoveal CNV and no eye with extrafoveal CNV experienced a 10-letter improvement at the 3-year examination. Mean CMT at baseline was 220 ± 15 μm and 235 ± 66 μm at 36 months ( P = 1.00). During the first and second years of follow-up, 5 juxtafoveal CNVs and 3 extrafoveal CNVs showed foveal involvement.
Conclusions
Intravitreal bevacizumab can be effective in the management of nonsubfoveal CNV secondary to AS, although monthly monitoring is required to control CNV recurrence or progression.
Angioid streaks (AS) can frequently be complicated by the development of choroidal neovascularization (CNV). In particular, it has been reported that CNV can be identified in up to 72%–86% of cases, with bilateral involvement in up to 71% of cases.2.
The management of AS–related CNV is still controversial, but the recent application of a therapy with intravitreal anti–vascular endothelial growth factor (anti-VEGF) molecules has shown positive visual outcomes for CNV subfoveal location.
Nevertheless, the follow-up of previous investigations was generally short, and limited data are available regarding nonsubfoveal CNV secondary to AS.
The aim of this study is to describe the effects of the treatment with intravitreal bevacizumab (IVB) for nonsubfoveal CNV associated with AS over a 3-year follow-up.
Methods
The study is designed as a prospective interventional cases series and is an extended investigation of previous research that was restricted to a 12-month follow-up.
All patients affected by juxtafoveal or extrafoveal CNV secondary to AS referred to the Department of Ophthalmology of the San Raffaele Scientific Institute in Milan from October 2010 to April 2012 were prospectively enrolled in the study. The research was approved by the local institutional review board and adhered to the tenets of the Declaration of Helsinki. Each patient was carefully informed about the purpose of the research, and provided signed consent to all procedures.
Inclusion criteria were diagnosis of AS; evidence of naïve CNV with juxtafoveal location (1–199 μm from the fovea center) or extrafoveal location (>199 μm from the fovea); and best-corrected visual acuity (BCVA) of at least 25 ETDRS letters (approximately corresponding to 20/320 Snellen equivalent). Exclusion criteria were any other ocular disease that could compromise vision in the study eye; pregnancy; previous corticosteroid therapy (either local or oral administration); uncontrolled systemic hypertension; peripheral vascular disease; and history of thromboembolism or stroke.
Each patient underwent an ophthalmologic examination, including measurement of BCVA using Early Treatment Diabetic Retinopathy Study (ETDRS) charts, slit-lamp biomicroscopy, fundus color photography, fluorescein angiography (FA), and spectral-domain optical coherence tomography (SDOCT). After a first IVB injection (1.25 mg), all patients were reevaluated at monthly intervals during the first year of follow-up. For the remainder of the follow-up each patient underwent a bimonthly assessment, including BCVA measurement, biomicroscopy, and SDOCT examination. FA was scheduled every 4 months. Additional FA or more frequent examinations were performed at the discretion of the retinal specialist, or when the patients complained of new disturbances. Further IVB treatments were performed following the detection of fresh hemorrhage on biomicroscopic examination, recurrence or persistence of fluid (any type) on OCT, and/or presence of leakage on FA.
Primary outcome measures were the change in the BCVA and the proportion of eyes gaining at least 10 ETDRS letters at the end of the follow-up. Secondary outcomes included central macular thickness (CMT) variations and extension to the fovea over the 3-year follow-up.
The normal distribution of continuous variables was verified with the Kolmogorov-Smirnov test. Repeated measures analysis of variance (ANOVA) was performed to analyze the changes in the BCVA and the CMT. Bonferroni correction for multiple comparisons was applied. Categorical variables were compared using the χ 2 test and a P value < .05 was taken as statistically significant. All calculations were performed with MedCalc Statistical Software version 15.8 (MedCalc Software bvba, Ostend, Belgium; 2015).
Results
Eighteen patients (18 eyes) fulfilled the inclusion and exclusion criteria. Three patients were lost during the second year of follow-up and were excluded from the final analysis owing to incomplete data collection. Thus, 15 patients (15 eyes) completed the 3-year follow-up study and were considered for the purpose of the investigation.
Baseline demographic and clinical characteristics are summarized in Table 1 . The mean age of the patients, 6 of whom were female, was 59.2 ± 10 years. Biopsy confirmed a diagnosis of pseudoxanthoma elasticum in 1 patient (6.6%). Eight patients (53.3%) showed juxtafoveal CNV and 7 (46.7%) presented with extrafoveal CNV. Mean CNV duration on the basis of the referred symptoms was 2.1 ± 0.7 months.
| Extrafoveal CNV | Juxtafoveal CNV | Total | |
|---|---|---|---|
| Number of patients | 7 | 8 | 15 |
| Age (mean ± SD, y) | 54.4 ± 8.6 | 63.5 ± 11.3 | 59.2 ± 10 |
| Sex (M/F) | 5/7 | 4/8 | 9/6 |
| Baseline BCVA (mean ± SD) | 82.1 ± 5.6 | 74.2 ± 11.8 | 77.9 ± 10.0 |
| Baseline CMT, μm (mean ± SD) | 213 ± 12 | 227 ± 16 | 220 ± 15 |
The mean BCVA showed no change, from 77.9 ± 10.0 ETDRS letters (mean ± SD, approximately corresponding to 20/28 Snellen equivalent) at baseline to 80.1 ± 5.4 letters at the 1-year examination (ANOVA, P = 1.00). Subsequently, a statistically significant BCVA worsening was registered at the 24-month examination (72.8 ± 10.0 ETDRS letters, P = .03) and at the 36-month examination (65.8 ± 15.0 ETDRS letters, approximately corresponding to 20/50 Snellen equivalent, P = .02), in comparison with the 1-year visual outcomes, whereas BCVA turned out to be stable between the time points at 24 and 36 months ( P = .38) and between the time points at baseline and 36 months ( P = .12) ( Figure 1 ).
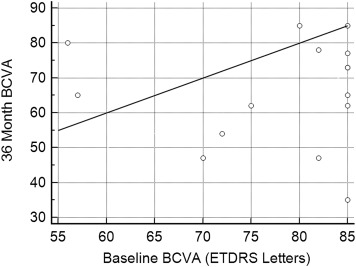
Table 2 lists the frequency distribution of the letter changes over the follow-up. One eye (12.5%) and 2 eyes (25%) with juxtafoveal CNV experienced a visual acuity improvement of 10 EDTRS letters at the 2- and 3-year examinations, respectively, whereas no eye in the extrafoveal subgroup showed a 10-ETDRS-letter improvement at the 3-year examination.
| ETDRS Letter Changes | 12 Months | 24 Months | 36 Months | |||
|---|---|---|---|---|---|---|
| Juxtaf CNV | Extraf CNV | Juxtaf CNV | Extraf CNV | Juxtaf CNV | Extraf CNV | |
| ≥10 letters | 2 | 1 | 1 | 0 | 2 | 0 |
| ≥5 letters | 4 | 1 | 2 | 0 | 2 | 1 |
| 0 | 2 | 4 | 2 | 3 | 0 | 1 |
| −5 letters ≤ | 2 | 2 | 4 | 4 | 6 | 5 |
| −10 letters ≤ | 2 | 0 | 3 | 3 | 5 | 4 |
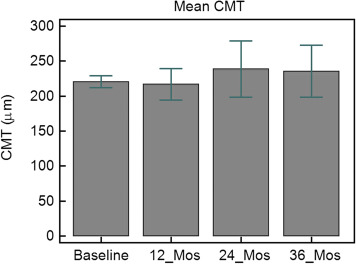
The mean CMT at baseline was 220 ± 15 μm, changing to 216 ± 40 μm at the 12-month examination (ANOVA, P = 1.00), 238 ± 72 μm at 24 months ( P = 1.00), and 235 ± 66 μm at 36 months ( P = 1.00) ( Figure 2 ). No statistically significant difference was found, either in the subgroup with extrafoveal CNV or in the subgroup with juxtafoveal CNV. Two eyes (13.3%) originally presenting with juxtafoveal CNV at baseline showed extension toward the fovea at the 12-month examination. During the second year of follow-up, 6 eyes (3 juxtafoveal CNV and 3 extrafoveal CNV) showed foveal involvement, whereas in no additional eye was a foveal invasion observed over the third year.
Subgroup analysis of the BCVA, from the moment CNV extended from a nonsubfoveal to a subfoveal location up to the final examination, disclosed a mean loss of 6 ETDRS letters in the juxtafoveal subgroups (actual letter change: +8, −19, +6, −30, +5) and 14 ETDRS letters in the extrafoveal subgroup (actual letter change: +5,−42, −5). It should be stressed that foveal involvement in the subgroup with initial extrafoveal location occurred without an intermediate juxtafoveal phase being precisely identified.
The mean number of IVB injections administered at the end of 3-year follow-up was 5.2 ± 2.7 (range, 1–10; 4.1 ± 2.9 injections in the subgroup with extrafoveal CNV, and 6.2 ± 2.2 injections in the subgroup with juxtafoveal CNV) ( Table 3 ). No systemic or ocular side effects were registered over the whole 36-month follow-up.
| Mean Bevacizumab Injections | All CNV | Extrafoveal CNV | Juxtafoveal CNV |
|---|---|---|---|
| 12 months | 2.53 | 1.85 | 3.12 |
| 24 months | 0.8 | 0.85 | 0.87 |
| 36 months | 1.8 | 1.42 | 2.25 |
| Total | 5.1 | 4.14 | 6.25 |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


