 Intraocular Lymphoid Tumors and Leukemias
Intraocular Lymphoid Tumors and LeukemiasIntraocular Lymphoid Tumors
Introduction to Intraocular Lymphoid Lesions
Tumors derived from lymphoid cells can sometimes develop in the eye and affect the uveal tract, retina, vitreous, or optic disc (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16). The several classifications of lymphoid malignancies that have been used in recent years are beyond the scope of this book. The Revised European American Lymphoma Classification has been popular and applied to intraocular lymphomas (16). Intraocular lymphoid tumors range from benign, relatively stable lesions to highly aggressive malignancies that can produce blindness and even death from associated brain or visceral disease. Specific intraocular lymphoid and lymphoplasmacytic tumors to be discussed in this section include uveal benign reactive lymphoid hyperplasia (BRLH), malignant lymphoma, and plasmacytoma (1, 2, 3, 4, 5).
BRLH is an idiopathic infiltration of the uveal tract by benign lymphocytes and plasma cells. It has rather characteristic clinical and histopathologic features. Most have considered it to be a benign reactive immunologic process, and evolution into malignant lymphoma is very uncommon (14).
The great majority of intraocular lymphomas are non-Hodgkin large-cell lymphomas comprising malignant lymphocytes of B-cell lineage. There are two general types of intraocular lymphoma: the uveal type and the retinovitreal type. The uveal type is generally associated with visceral or nodal lymphoma and rarely with central nervous system (CNS) lymphoma. It is generally found in immunocompetent patients. The retinovitreal type is closely related to primary CNS lymphoma (PCNSL) and, when it appears initially in the eye, it has been called primary intraocular lymphoma (PIOL). This is not an ideal term because a primary lymphoma can also occur in the uveal tract, without any association with the CNS. It has a predilection to develop in immunocompromised patients, but it is also seen in patients who are presumably immunocompetent. Of all patients with intraocular lymphoma, approximately 60% have the PCNS lymphoma, 15% have the uveal form, about 5% have both types simultaneously, and 20% have no demonstrable extraocular lymphoma (3). We believe that almost all patients in the latter group will develop extraocular lymphoma on long-term follow-up.
Benign or malignant plasmacytomas can rarely occur in the uveal tract. Both types can appear as an isolated solitary lesion, with no demonstrable systemic associations, or as a component of multiple myeloma. Other lymphoid malignancies that can rarely involve the intraocular structures include Hodgkin disease, angiotropic large-cell lymphoma, T-cell lymphoma (mycosis fungoides), and adult T-cell leukemia/lymphoma. These rare forms are similar to the two more common forms with regard to ocular presentations, (7, 8, 9, 10, 11, 12, 13) and are not illustrated in this atlas.
Selected General References
1. Shields JA, Shields CL. Intraocular lymphoid tumors and leukemias. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:1489-1512.
2. Dhaliwal RS, Schachat AP. Leukemias and lymphomas. In: Ryan SJ, ed. Retina, 3rd ed. St. Louis: CV Mosby; 2001:842-858.
3. Harbour JW, Char DH. Intraocular lymphoid tumors. In: Guyer DR, Yannuzzi LA, Chang S, et al. Retina-Vitreous-Macula, Vol. 2. Philadelphia: WB Saunders; 1999:1204-1216.
4. Chan CC, Buggage RR, Nussenblatt RB. Intraocular lymphoma. Curr Opin Ophthalmol 2002;13:411-418.
5. Grossniklaus HE, Martin DF, Avery R, et al. Uveal lymphoid infiltration. Report of four cases and clinicopathologic review. Ophthalmology 1998;105:1265-1273.
6. Mori A, Deguchi HE, Mishima K, et al. A case of uveal, palpebral, and orbital invasions in adult T-cell leukemia. Jpn J Ophthalmol 2003;47:599-602.
7. Jensen OA, Johansen S, Kiss K. Intraocular T-cell lymphoma mimicking a ring melanoma. First manifestation of systemic disease. Report of a case and survey of the literature. Graefes Arch Clin Exp Ophthalmol 1994;232:148-152.
8. Yahalom C, Cohen Y, Averbukh E, et al. Bilateral iridociliary T-cell lymphoma. Arch Ophthalmol 2002;120:204-207.
9. Towler H, de la Fuente M, Lightman S. Posterior uveitis in Hodgkin’s disease. Aust N Z J Ophthalmol 1999;27:326-330.
10. Elner VM, Hidayat AA, Charles NC, et al. Neoplastic angioendotheliomatosis. A variant of malignant lymphoma immunohistochemical and ultrastructural observations of three cases. Ophthalmology 1986;93:1237-1245.
11. Keltner JL, Fritsch E, Cykiert RC, et al. Mycosis fungoides. Intraocular and central nervous system involvement. Arch Ophthalmol 1977;95:645-650.
12. Levy-Clarke GA, Buggage RR, Shen D, et al. Human T-cell lymphotropic virus type-1 associated T-cell leukemia/lymphoma masquerading as necrotizing retinal vasculitis. Ophthalmology 2002;109:1717-1722.
13. Kohno T, Uchida H, Inomata H, et al. Ocular manifestations of adult T-cell leukemia/lymphoma. A clinicopathologic study. Ophthalmology 1993;100: 1794-1799.
14. Cockerham GC, Hidayat AA, Bijwaard KE, et al. Re-evaluation of “reactive lymphoid hyperplasia of the uvea”: an immunohistochemical and molecular analysis of 10 cases. Ophthalmology 2000;107:151-158.
15. Nussenblatt RB, Chan CC, Wilson WH, et al. CNS and Ocular Lymphoma Workshop Group. International Central Nervous System and Ocular Lymphoma Workshop: recommendations for the future. Ocul Immunol Inflamm 2006;14:139-144.
16. Coupland SE, Foss HD, Hidayat AA, et al. Extranodal marginal zone B cell lymphomas of the uvea: an analysis of 13 cases. J Pathol 2002;197:333-340.
Benign Reactive Lymphoid Hyperplasia of the Uvea
General Considerations
Benign reactive lymphoid hyperplasia is an idiopathic condition characterized by infiltration of the uveal tract by benign lymphocytes and plasma cells (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15). There is controversy regarding its benign nature, and some cases originally classified as BRLH have been reclassified as well-differentiated small-cell lymphoma (8). In our experience, transformation into lymphoma is extremely uncommon. It has rarely been associated with Waldenstrom macroglobulinemia (2). In some cases, BRLH or low-grade lymphoma can have multisystem manifestations, a condition called Castleman syndrome. Uveal involvement has been observed with this syndrome (13).
Clinical Features
Uveal BRLH affects mainly adults and is usually unilateral (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15). It can occur in the iris, ciliary body, or choroid and can simultaneously involve the conjunctiva and orbit. In the iris, it appears either as a circumscribed mass or as a diffuse amelanotic thickening of the iris stroma (11). In the ciliary body, it presents as an amelanotic mass that can push the iris forward, simulating a ring melanoma and causing angle closure glaucoma (12). Choroidal BRLH appears as one or more circumscribed yellow-orange lesions that range from minimally elevated to dome shaped. Choroidal BRLH also manifests as numerous small yellow lesions that may be similar to birdshot choroidopathy, multifocal choroiditis, or sarcoidosis. These focal lesions can eventually coalesce to produce a diffuse thickening of the choroid. We have also seen cases that appear as a diffuse red-orange lesion in the posterior pole, remarkably similar to the diffuse choroidal hemangioma seen with Sturge-Weber syndrome. The vitreous is usually clear, with no evident inflammatory or tumor cells (6). A secondary, nonrhegmatogenous retinal detachment with clear serous subretinal fluid is often present. Spontaneous tear of the RPE is a rare complication (5).
Uveal BRLH may be similar clinically to lymphoma, metastasis, localized or diffuse amelanotic choroidal melanoma, uveal effusion syndrome, posterior scleritis, birdshot choroidopathy, choroidal sarcoidosis, diffuse choroidal hemangioma, and other solitary, multifocal or diffuse yellow-orange fundus lesions. A clinical history and ocular examination, systemic evaluation, and selected laboratory studies can help in differentiating uveal BRLH from these entities.
Diagnostic Approaches
A simple, crucial diagnostic step in evaluating a patient with a fundus mass that could be BRLH or lymphoma is to carefully check the conjunctiva and look for the classic pink infiltration that characterizes either a benign or a malignant lymphoid tumor. Such a “salmon patch” infiltration is often subtle and located in the conjunctival fornix. This finding should prompt the clinician to perform biopsy of the conjunctival lesions rather than the intraocular lesion. The histopathology of the uveal and conjunctival components is generally similar or identical.
Fluorescein angiography of BRLH shows no specific features and may be similar to that for metastasis or lymphoma or choroidal inflammation. Like these other choroidal lesions, they are relatively hypofluorescent in the early vascular filling phases and show moderate late staining beginning in the venous or recirculation phase.
Ultrasonography shows a diffuse thickening of the choroid with medium to low internal reflectivity, similar to choroidal melanoma. However, a classic ultrasound finding that is seen in many cases is an ovoid echolucent epibulbar mass, usually posterior to the sclera (3). Even though it is strongly suggestive of a lymphoid tumor, extraocular extension of an amelanotic choroidal melanoma and other tumors can produce a similar pattern.
In cases in which the diagnosis is uncertain and there is no evidence of an episcleral mass to biopsy, a uveal biopsy can be performed (4,14,15). This can be done by fine needle aspiration biopsy, transvitreal biopsy with a vitrectomy instrument, or an eye wall biopsy. The first two of these yield scanty material for diagnosis and show only cells that do not reflect the true architecture of the lesion. Eye wall biopsy provides a better tissue diagnosis, but the surgery is more difficult. In general, FNAB is quicker and easier to perform and often yields a correct diagnosis (14).
Pathology
Gross examination of enucleated eyes shows a diffuse, amelanotic uveal mass. The epibulbar component, if present, is evident on gross evaluation (1,2,9). Histopathologically, uveal BRLH is characterized by a localized or diffuse replacement of the uveal stroma by an infiltration of benign lymphocytes and plasma cells. It can be confined to one portion of the uvea, or it can diffusely affect the entire uveal tract. It is most pronounced in the posterior choroid. In some cases, germinal centers are present in the lesion. Intranuclear inclusions, called Dutcher bodies, are often seen. Immunohistochemistry and polymerase chain reaction can be used to further categorize the condition as a low-grade proliferation of B-lymphocytes.
Management
The management of suspected uveal BRLH should be determined by the clinical findings. The patient should have a systemic evaluation to exclude lymphoma and myeloma. If the involvement is small and the patient is asymptomatic, periodic observation may be justified. Sometimes this condition can remain stationary for months or years. A larger, symptomatic lesion with secondary retinal detachment or other complications can be managed initially by a standard course of oral corticosteroids with tapering of the medication. In general, corticosteroids bring about some improvement. Whole-eye irradiation, usually 20 to 25 Gray of external beam in divided doses, is often necessary if corticosteroids fail to control the disease. The response of BRLH to irradiation appears to be favorable.
The visual prognosis depends on the extent of the disease, but most patients with less advanced disease have a fairly good visual outcome. The systemic prognosis for uveal BRLH is generally good, and evolution into systemic lymphoma appears to be very rare.
Selected References
1. Shields JA, Shields CL. Intraocular lymphoid tumors and leukemias. In: Shields JA, Shields CL, eds. Intraocular Tumors. A Text and Atlas. Philadelphia: WB Saunders; 1992:489-512.
2. Ryan SJ, Zimmerman LE, King FM. Reactive lymphoid hyperplasia. An unusual form of intraocular pseudotumor. Trans Am Acad Ophthalmol Otolaryngol 1972;76:652-671.
3. Chang TS, Byrne SF, Gass JD, et al. Echographic findings in benign reactive lymphoid hyperplasia of the choroid. Arch Ophthalmol 1996;114:669-675.
4. Cheung MK, Martin DF, Chan CC, et al. Diagnosis of reactive lymphoid hyperplasia by chorioretinal biopsy. Am J Ophthalmol 1994;118:457-462.
5. Matsuo T, Matsuo N, Shiraga F, et al. Retinal pigment epithelial tear in reactive lymphoid hyperplasia of uvea. Ophthalmologica 1990;200:46-54.
6. Jakobiec FA, Sacks E, Kronish JW, et al. Multifocal static creamy choroidal infiltrates. An early sign of lymphoid neoplasia. Ophthalmology 1987;94: 397-406.
7. Desroches G, Abrams GW, Gass JD. Reactive lymphoid hyperplasia of the uvea. A case with ultrasonographic and computed tomographic studies. Arch Ophthalmol 1983;101:725-728.
8. Cockerham GC, Hidayat AA, Bijwaard KE, et al. Re-evaluation of “reactive lymphoid hyperplasia of the uvea”: an immunohistochemical and molecular analysis of 10 cases. Ophthalmology 2000;107:151-158.
9. Grossniklaus HE, Martin DF, Avery R, et al. Uveal lymphoid infiltration. Report of four cases and clinicopathologic review. Ophthalmology 1998;105:1265-1273.
10. Duker JS, Shields JA, Eagle RC. Ocular lymphoid hyperplasia. Arch Ophthalmol 1989;107: 446-447.
11. Shields JA, Augsburger JJ, Gonder JR, et al. Localized benign lymphoid tumor of the iris. Arch Ophthalmol 1981;99:2147-2148.
12. Gass JDM. Retinal detachment and narrow angle glaucoma secondary to inflammatory pseudotumor of the uveal tract. Am J Ophthalmol 167; 64:612-621.
13. Gittinger JW Jr. Ocular involvement in Castleman’s disease. Response to radiotherapy. Ophthalmology 1989;96:1646-1649.
14. Shields JA, Shields CL, Ehya H, et al. Fine-needle aspiration biopsy of suspected intraocular tumors. The 1992 Urwick Lecture. Ophthalmology 1993;100:1677-1684.
15. Scherfig E, Prause JU, Jensen OA. Transvitreal retinochoroidal biopsy. Graefes Arch Clin Exp Ophthalmol 1989;227:369-373.
▪ Uveal Benign Reactive Lymphoid Hyperplasia
Uveal benign reactive lymphoid hyperplasia (BRLH) is a benign lesion in which the uveal tract is infiltrated by a combination of lymphocytes and plasma cells. Because it can simultaneously involve the conjunctiva, careful external ocular examination may suggest the diagnosis of the intraocular lesion.
Shields JA, Augsburger JJ, Gonder JR, et al. Localized benign lymphoid tumor of the iris. Arch Ophthalmol 1981;99:2147-2148.
 Figure 24.1. Peripheral iris involvement with a localized mass in a 33year-old woman. The lesion was successfully excised by iridocyclectomy, and it proved histopathologically to be BRLH. |
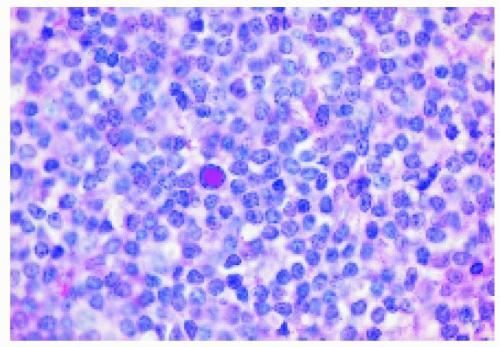 Figure 24.2. Histopathology of uveal benign reactive lymphoid hyperplasia, showing mature lymphocytes, one of which, near the center of the photomicrograph, has an intranuclear inclusion (Dutcher body). (Periodic acid-Schiff X200.) |
 Figure 24.3. Localized choroidal involvement with BRLH near the temporal equator of the right eye in a 49-year-old man. |
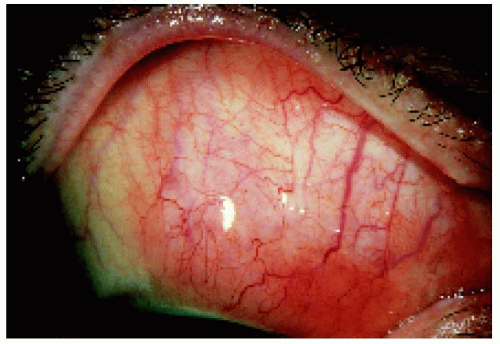 Figure 24.4. Characteristic lymphoid infiltration of the conjunctiva in the same eye shown in Figure 24.3. A conjunctival biopsy revealed benign lymphoid infiltration. |
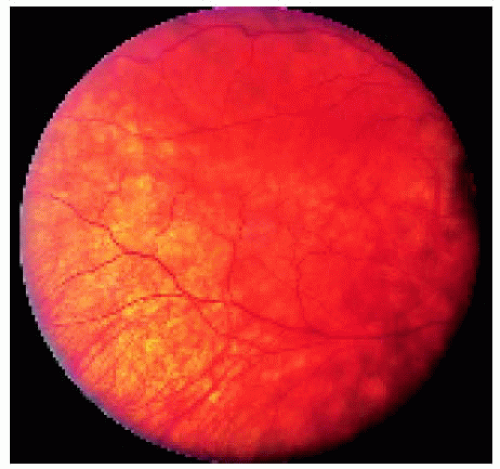 Figure 24.5. Appearance of the fundus lesion shown in Figure 24.3 after 2000 cGy of ocular irradiation, demonstrating excellent response. |
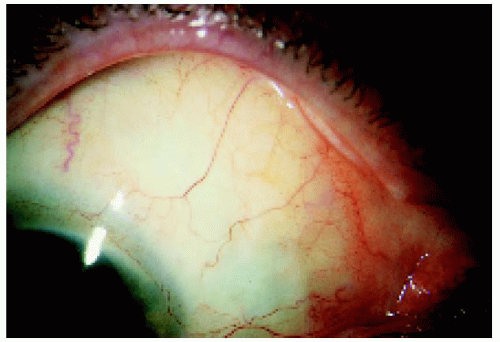 Figure 24.6. Appearance of the conjunctival lesion after the irradiation, showing excellent response. |
▪ Uveal Benign Reactive Lymphoid Hyperplasia (BRLH): Clinical and Pathologic Features
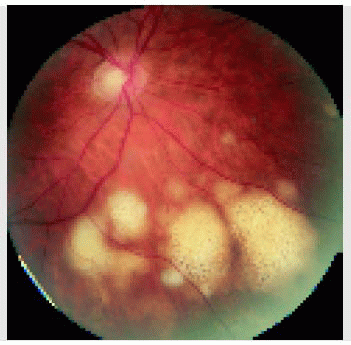
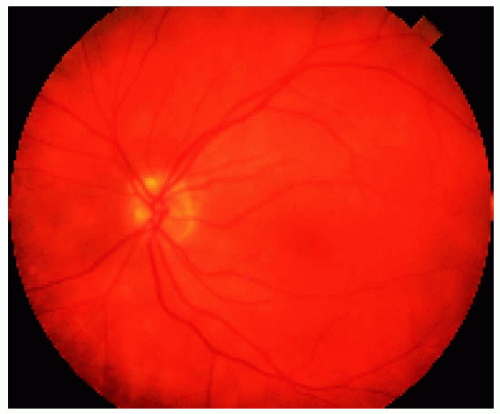 Figure 24.7. Multiple subtle yellow choroidal lesions in left eye of a 65year-old woman. The small lesions are difficult to visualize with photography. Note the red-orange color to the posterior choroid. |
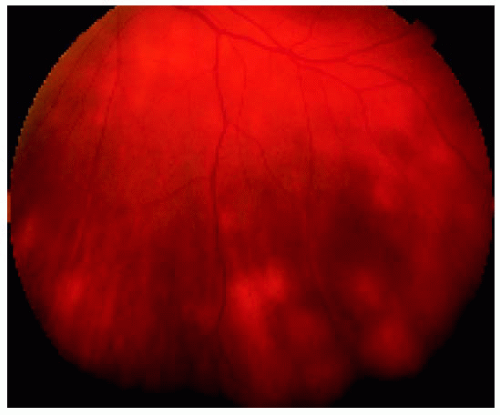 Figure 24.8. More pronounced peripheral fundus lesions located inferiorly in the same eye shown in Figure 24.7. The lesions are very similar to those seen with birdshot or sarcoid choroidopathy. |
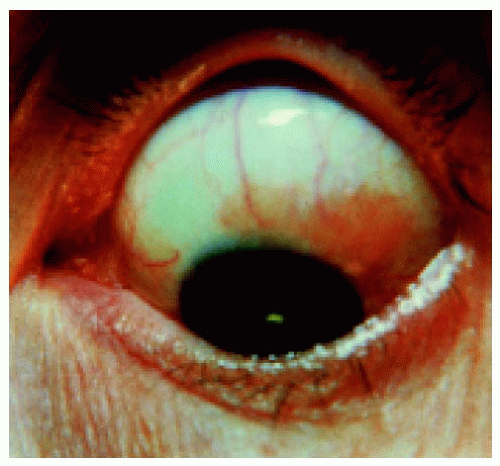 Figure 24.9. Conjunctiva of the same eye shown in Figures 24.7 and 24.8. Note the salmon patch infiltration. This is seen with lymphoid infiltration but not with birdshot choroidopathy. This is very helpful in clinical diagnosis. |
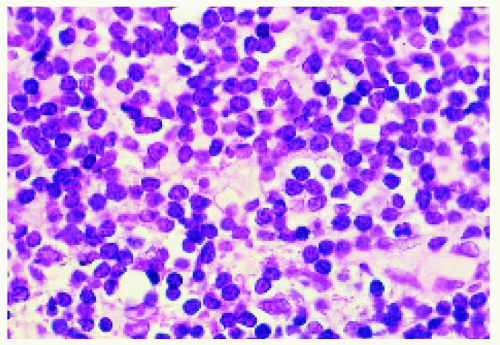 Figure 24.10. Histopathology of the lesion shown in Figure 24.9, demonstrating uniform small lymphocytes. |
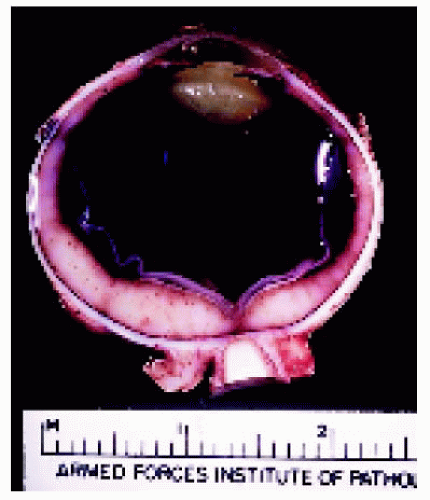 Figure 24.11. Grossly sectioned eye with BRLH. Note the marked thickening of the entire posterior uvea and the perineural infiltration adjacent to the optic nerve in the orbit. (Courtesy of the Armed Forces Institute of Pathology, Washington, D.C.) |
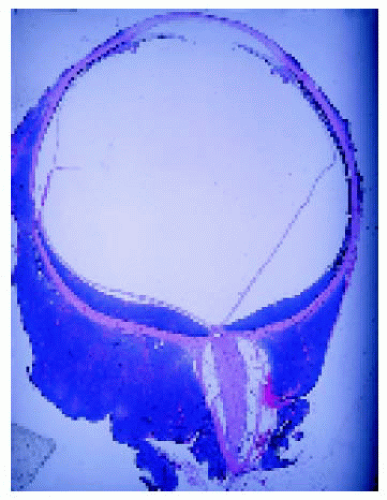 Figure 24.12. Low-power photograph of a pathology slide of an eye with uveal benign reactive lymphoid hyperplasia. The lesion has a darkblue color characteristic of lymphoid tumor. (Courtesy of the Armed Forces Institute of Pathology, Washington, D.C.) |
▪ Uveal Benign Reactive Lymphoid Hyperplasia (BRLH): Diagnostic Studies and Treatment
A case is shown with clinical appearance, fluorescein angiography, ultrasonography, magnetic resonance imaging, and response to irradiation.
 Figure 24.13. Wide-angle fundus photograph showing diffuse thickening of the entire posterior aspect of the choroid in the left eye. This is subtle in the photograph, but was quite elevated when viewed with binocular indirect ophthalmoscopy. The fundus has a diffuse orange color, resembling a diffuse choroidal hemangioma. |
 Figure 24.14. Closer view of the area nasal to the disc, showing the choroidal thickening and red-orange color to the fundus. Note also the hyperemia of the disc. |
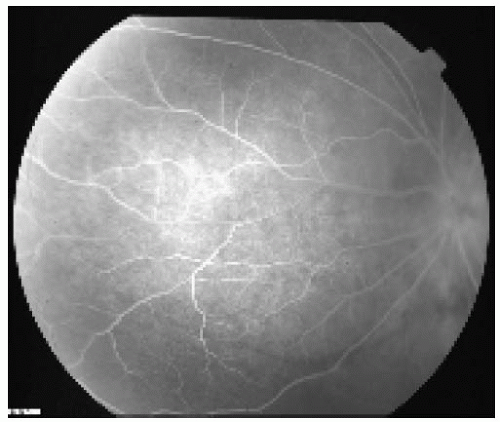 Figure 24.15. Fluorescein angiography focused on the region nasal to the optic disc, showing very subtle hyperfluorescence of the choroidal infiltration and subtle horizontal choroidal folds inferiorly. |
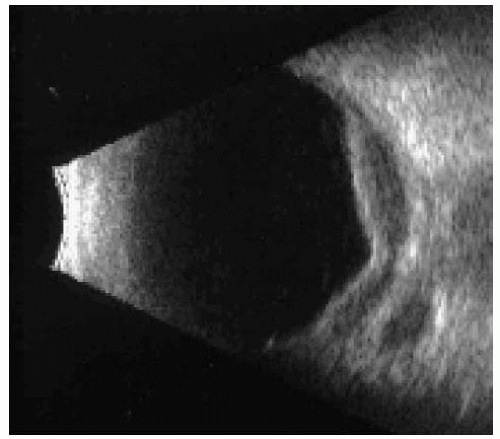 Figure 24.16. B-scan ultrasonogram, showing choroidal thickening with low to medium internal reflectivity. Note the echolucent area posterior to the sclera within the orbital fat. This nodule of orbital involvement is a common and typical finding in uveal benign reactive lymphoid hyperplasia but can also be seen with extrascleral extension of diffuse uveal melanoma and in true malignant lymphoma of the choroid. |
 Figure 24.17. Axial magnetic resonance imaging in T1 -weighted image with contrast, showing diffuse, irregular, hyperintense thickening of the choroid. |
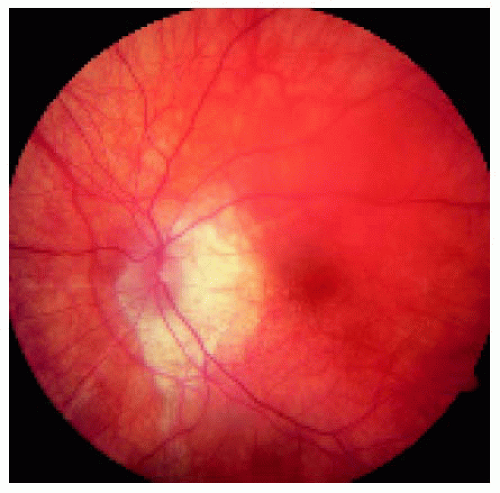 Figure 24.18. Appearance of the same eye 2 years after external beam irradiation, showing resolution of the choroidal infiltration. There is some peculiar subretinal fibrosis temporal to the optic disc. |
▪ Uveal Benign Reactive Lymphoid Hyperplasia (BRLH) Masquerading as Birdshot Choroiditis or Sarcoidosis
Uveal reactive lymphoid hyperplasia can cause a clinical appearance very similar to “birdshot choroidopathy” or choroidal sarcoidosis. The finding of a salmon-colored lesion in the conjunctiva suggests lymphoid hyperplasia, and a biopsy can confirm the diagnosis and exclude sarcoidosis and birdshot choroidopathy. A bilateral case is illustrated.
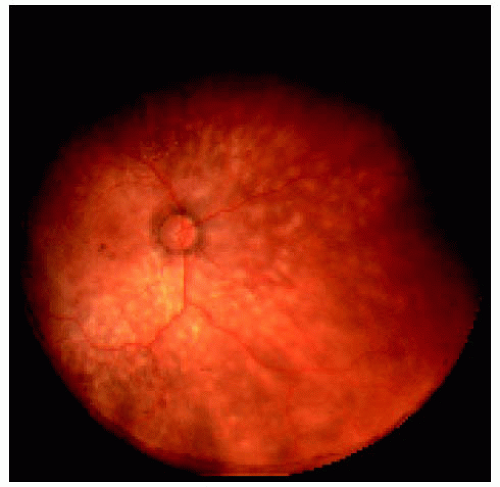 Figure 24.19. Wide-angle fundus photograph of the right eye in a 60-year-old man, showing numerous discrete yellow-orange deposits in the choroid. |
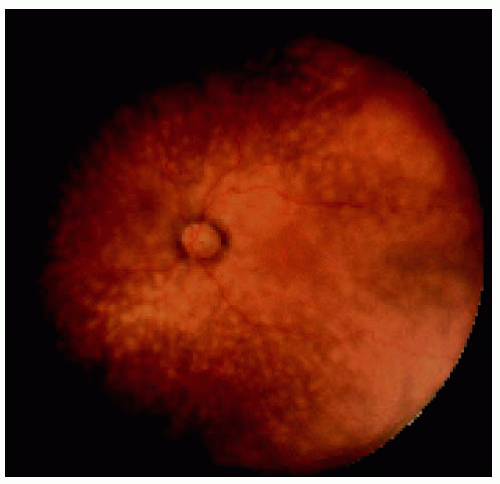 Figure 24.20. Identical findings in the left eye. |
 Figure 24.21. Closer view of the posterior pole in the right eye, showing macular edema and concentration of the focal choroidal lesions inferior to the optic disc. |
 Figure 24.22. Posterior pole of the left eye, showing similar changes. The patient was referred for a choroidal biopsy to exclude sarcoidosis and birdshot choroidopathy. |
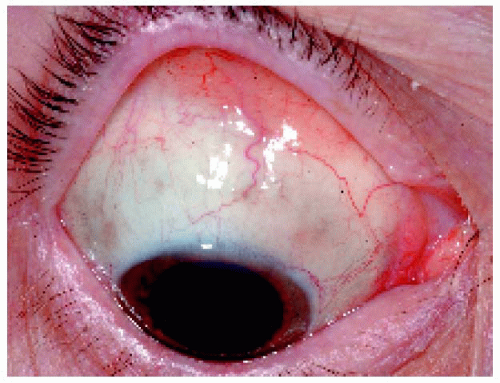 Figure 24.23. Salmon-colored lesion found in the superior fornix of the right eye. A conjunctival biopsy rather than a choroidal biopsy was done, and the diagnosis of reactive lymphoid hyperplasia was confirmed. |
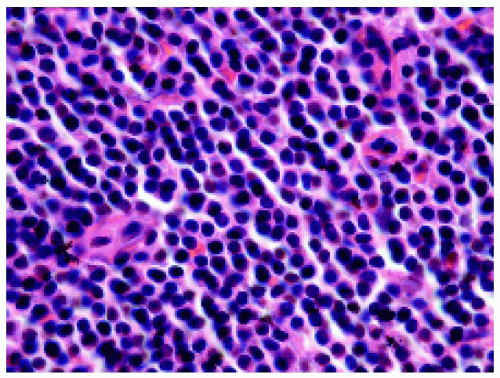 Figure 24.24. Histopathology, showing well-differentiated lymphocytes compatible with mucosal-associated lymphoid tissue (MALT) lymphoma. |
▪ Uveal Benign Reactive Lymphoid Hyperplasia (BRLH): Wide-Angle Imaging, Ultrasonography, and Magnetic Resonance Imaging
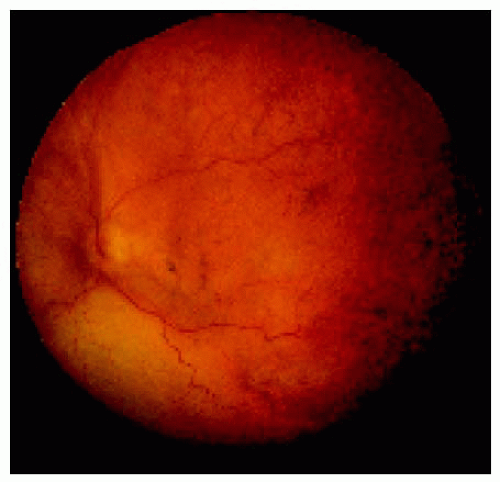 Figure 24.25. Fundus appearance of the left eye of a 66-year-old man with benign reactive lymphoid hyperplasia of the choroid. There is a diffuse red-orange choroidal thickening and a secondary retinal detachment inferiorly with shifting subretinal fluid. |
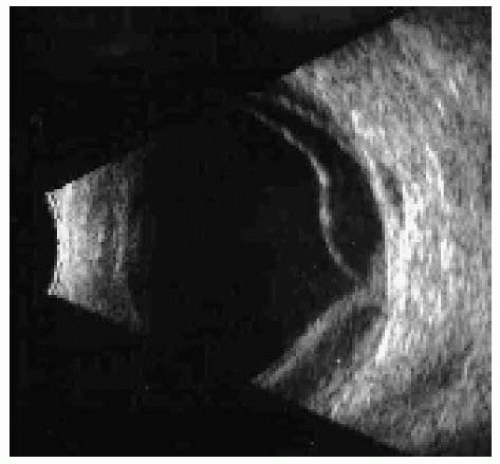 Figure 24.26. B-scan ultrasonogram, showing diffuse thickening of the choroid and secondary retinal detachment. Also note the small echolucent area posterior to the sclera, which represents simultaneous adjacent orbital involvement. |
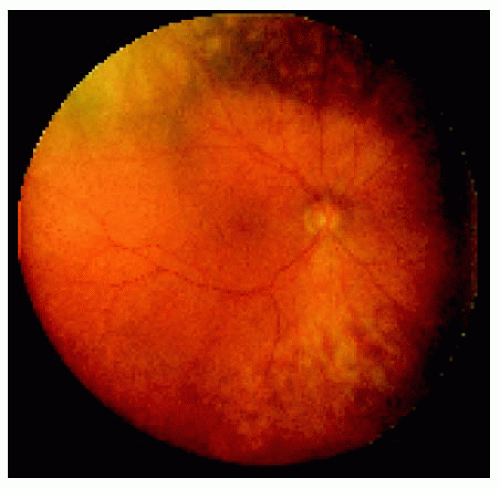 Figure 24.27. Benign reactive lymphoid hyperplasia of the choroid in the right eye of a 44-year-old man. The pigment epithelial alterations suggest that the lesion and the retinal detachment are beginning to resolve. |
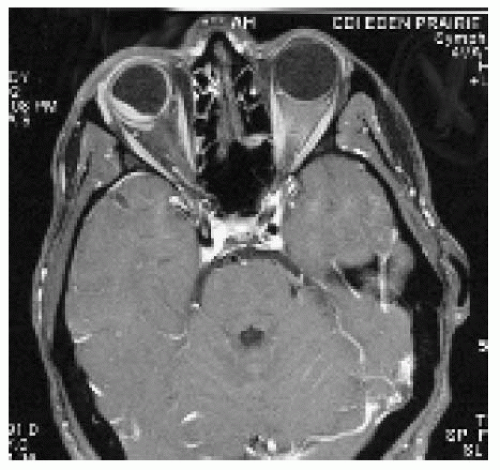 Figure 24.28. Axial magnetic resonance imaging in T1 -weighted image with gadolinium enhancement and fat suppression, showing a diffuse enhancing lesion of the choroid with orbital involvement posterior to the sclera. |
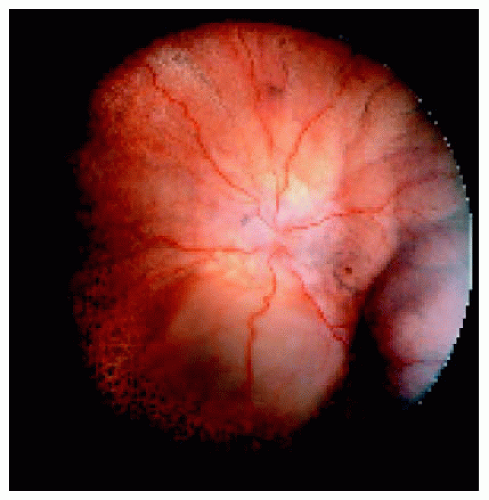 Figure 24.29. Resolving benign reactive lymphoid hyperplasia with secondary retinal pigment epithelium proliferation. The inferotemporal mass resembles a ciliochoroidal detachment as seen with uveal effusion syndrome. However, it was a solid lymphocytic infiltration of the peripheral choroid and ciliary body. |
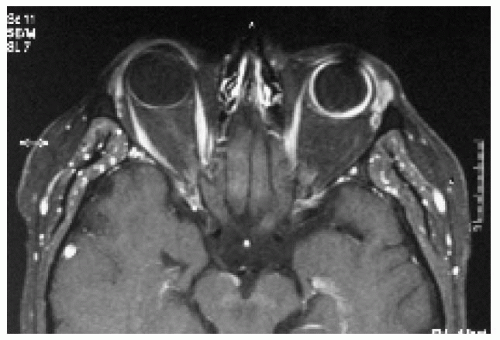 Figure 24.30. Axial magnetic resonance imaging in T1 -weighted image with gadolinium enhancement and fat suppression, showing a diffuse enhancing lesion of the left choroid. Uveal effusion mostly involves the peripheral choroid and ciliary body and is less likely to cause thickening of posterior choroid. |
Primary Intraocular Lymphoma
General Considerations
Primary central nervous system lymphoma (PCNSL) is an unusual variant of lymphoma that affects the brain, meninges, and often the intraocular structures (1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42). If the eye is involved first, it is called primary intraocular lymphoma (PIOL) (42), which is the term that we will employ here whether or not the central nervous system (CNS) is affected.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


