13
Interpreting the Videostroboscopic Examination
Videostroboscopy is a distinctive tool used in the study of vocal dysfunction and laryngeal disorders. Refinements of equipment over the past two-plus decades has made the examination of the larynx easier, better, and more precise than ever before. In spite of these improvements, the diagnosis of many problems is often illusive, primarily because the laryngologic community is still in the process of learning how to interpret the videostroboscopic results, but also at times because the exam itself is deficient in uncovering an underlying problem. This chapter, then, will attempt to give insight to those who may be asked to perform this exam so that at least the evidence of disorder may be captured on electronic media. It is up to the laryngologist and the speech-language pathologist to look closely for the clues hidden in that media to effectively diagnose and eventually treat the patient. Performing a videostroboscopy is usually not a difficult task, but the goal is not just to do the exam but also to make sure the clinician gets all the information he or she requires for good patient care.
 General Observations
General Observations
Before looking specifically at the vocal folds and their function, we can make several general observations while first examining the laryngopharynx. These observations should be noted in a separate area of the videostroboscopy report so they may be easily identified. General observations include mucosal coloration and swelling, presence or absence of chronic infection (whitish mucus and debris) of the laryngopharynx, pooling of secretions in the piriform sinuses, and silent aspiration (saliva going in and out of the posterior glottis without reflex coughing).
One of the most common causes of dysphonia today is infection of the laryngopharynx with either fungal or bacterial (Staphylococcus aureus, mostly methicillin sensitive) organisms. The incidence of chronic throat infections with these organisms has skyrocketed in the past 10 to 15 years primarily because of the changes in treatment of all types of infections with antibiotics that kill normal throat flora in addition to treating the infection. The signs of chronic bacterial or fungal infection that should be noted during the general observations of the larynx include a more generalized erythema/edema affecting the larynx as a whole (false cords, epiglottis, aryepiglottic folds) as well as the hypopharynx (posterior pharyngeal wall, piriform sinuses). Erythema and/or edema of the posterior larynx (arytenoid and interarytenoid mucosa) are more likely to be secondary to acid reflux from the stomach up into the larynx (laryngopharyngeal reflux). This should be differentiated from the generalized signs of infection and noted as such in the report.
Pooling of secretions in the piriform sinuses may signify difficulty swallowing from any cause and can involve structures extending from the oral musculature to the esophagogastric junction. Documenting this in the videostroboscopy report should be followed by a suggestion that a referral for a swallow evaluation be made. Finally, silent aspiration is the end stage of severe laryngopharyngeal dysfunction. It usually includes both anatomic and neurologic deficits of the laryngopharynx that result in great impairment of swallowing.
 Visualizing the Larynx
Visualizing the Larynx
We know intuitively that everyone’s voice is a little bit different. How then is it possible to examine the human larynx and know what we need to see? The best approach to accomplish this is to go back to the basics of voice production, for therein lie the clues necessary to understand what we need to see. Consideration of the patient’s chief complaint, listening to the voice before doing any physical examination, and understanding how voice is produced are paramount to understanding how to examine a voice-disordered larynx. Even so, it must be kept in mind that the pre-examination information is not always specific. Some vocal symptoms may be classified as general, because that symptom can result from a variety of underlying problems. For example, a softer-than-normal voice may be generated by a whole host of underlying pathology including generalized systemic weakness, diaphragmatic paralysis, chronic obstructive pulmonary disease, subglottic or tracheal stenosis, vocal fold paralysis, arytenoid subluxation, and so forth. Vocal softness, then, is not very helpful in pointing the clinician in the direction of where to look for possible laryngeal problems, and the exam must evaluate for a broad range of possible problems. On the other hand, a “graty” sound to the voice is almost always indicative of a problem at the arytenoids cartilages. So in this case, we have real clues that indicate where we need to look for trouble. With experience, the voice clinician understands the implications of the pre-examination information and uses it effectively to guide the examination itself.
Instrumentation
Instrumentation used in videostroboscopy includes a telescopic device (rigid or flexible), a light source, a camera, a microphone, a strobe unit linked to the microphone’s audio signal, and a video unit typically linked to a computer for digital or analog capture. Finally, the information recorded during video and audio capture needs to be saved in a format and in such a way that it is categorized and easily retrievable. Before digital capture was readily available, the recorded material was usually saved in either VHS or Hi-8 format. With digital recordings, this information is now saved on either DVD media or hard drives.
Laryngologists today use either a rigid telescope (70 or 90 degree) or a flexible endoscope connected to the videostrobe system. Rigid endoscopy remains the gold standard for clear and precise video capture and is usually well tolerated with or without local anesthesia to the pharynx. With the recent advent of distal chip flexible scopes (the camera resides at the far end of the scope), endoscopic examination is available with less distortion of the laryngopharynx from pulling forward on the tongue. In addition, we can now visualize laryngeal function more fully and naturally (see later), putting the larynx through its paces while capturing a very good picture of this organ. Some clarity is sacrificed, but the functional information gained is better overall.
The Vocal Folds
As a review, voice is produced when the lining tissue of the anterior vocal folds, the mucosa, is put into oscillation and changes a steady stream of air into a rhythmically interrupted air stream.1 We may separate the vocal folds into their two distinct but interactive parts: the anterior vocal fold (membranous soft tissue) and the posterior vocal fold (arytenoid cartilage). The arytenoids are connected to their respective vocal fold ligaments and thyroarytenoid muscles at their vocal processes and along their anterior faces. For all intents and purposes, the medial arytenoid mucosa does not vibrate enough to contribute to the voice under normal conditions but it may in some dysphonias. Please refer to Chapters 2 and 3 for a more detailed discussion of laryngeal anatomy, histology, and physiology.
Anterior Membranous Vocal Folds
The anterior vocal folds include the vocal ligaments, the medial and lateral thyroarytenoid muscles, the overlying vocal fold mucosa, and the connective tissue holding everything together. Dysphonia occurs most often when the vocal fold mucosal waves are disturbed. Thus, observation of the mucosal waves with videostroboscopy is a must. Mucosal waves are described as being present or absent and as having amplitude and speed. In addition, the mucosal waves of one vocal fold must be compared with and described in relation to their counterpart waves on the opposite vocal fold. These latter observations are most important as normal sound production depends upon mucosal waveforms that are nearly identical from side to side. The best voices are generated when mucosal waves are equal, symmetric, and in phase bilaterally.
Videostroboscopy should be aimed, in part, at obtaining enough visual information to describe the mucosal waves completely. This includes:
 A clear picture of both vocal folds at rest and during phonation.
A clear picture of both vocal folds at rest and during phonation.
 Release of enough supraglottic tension to see the vocal folds as completely as possible.
Release of enough supraglottic tension to see the vocal folds as completely as possible.
 Observation of the mucosal waves bilaterally with phonation. This requires good tracking of the vocal sound by the stroboscopic machine.
Observation of the mucosal waves bilaterally with phonation. This requires good tracking of the vocal sound by the stroboscopic machine.
Once the video and audio signals are captured, they can be stored within the computer or, more commonly, on removable storage data (DVD, large-capacity hard drive). The most common commercially available hardware and software include ways to store and recover data rather easily and quickly.
After the pictures are captured, saved, and stored, they should be replayed in both normal-speed and slow-speed modes to further examine what is happening during phonation. With this review, we want to look for and comment on:
 Specific areas where the mucosal waves may be absent on one or both vocal folds.
Specific areas where the mucosal waves may be absent on one or both vocal folds.
 The relative sizes of the mucosal waves on each side (normal, too large, or too small).
The relative sizes of the mucosal waves on each side (normal, too large, or too small).
 Whether the mucosal waves are starting and traveling at the same time or whether one side is going “early” and the opposite side lags behind. This is described as either symmetric (normal and equal) or asymmetric (different and unequal).
Whether the mucosal waves are starting and traveling at the same time or whether one side is going “early” and the opposite side lags behind. This is described as either symmetric (normal and equal) or asymmetric (different and unequal).
 An estimate of the percentage of phonatory time spent with symmetric/asymmetric mucosal waves.
An estimate of the percentage of phonatory time spent with symmetric/asymmetric mucosal waves.
Information gathered about the specifics of the mucosal waves will aid the laryngologist in the search for causes of the patient’s dysphonia. For more information on the specifics of each vibratory parameter, please see subsequent chapters.
Posterior Cartilaginous Vocal Folds
Even though the anterior vocal folds are the area of sound generation, dysphonia may also be caused by posterior vocal fold abnormalities. Close observation of the positions, movements, and interactions between the arytenoid cartilages are also an important part of a videostroboscopic exam. Once we begin to closely pay attention to the posterior larynx and the movements of the arytenoids, we will uncover a whole host of things that could be causing phonatory problems and that were never thought of before.
Arytenoid Position
The normal position of the arytenoid cartilages is sitting upright on the posterior cricoid rim. When viewing during videostroboscopy, we see the arytenoids from above. Thus under the mucosa at the posterior end of each aryepiglottic fold lies the superior process of the arytenoid. The medial face of the arytenoid should be fully observable, and the posterior and medial extent of each arytenoid with the smaller corniculate cartilage attached directly to the superior arytenoid may be seen. The right and left cuneiform cartilages are frequently mistaken for the superior apex of the arytenoid. The cuneiforms look somewhat like a flattened sphere residing at the posterior end of the aryepiglottic fold, and aside from being a “curiosity” in humans, they do add some weight to those folds (Fig. 13.1A).
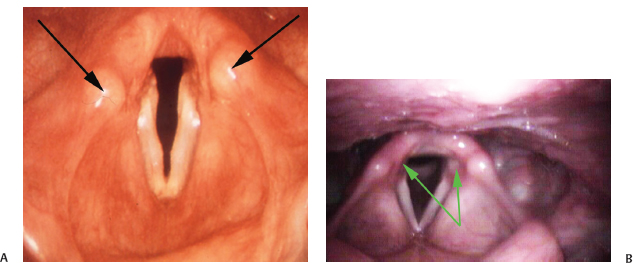
Fig. 13.1 (A) Normal larynx. The arrows indicate cuneiform cartilages in the aryepiglottic folds. Folds are in a partially adducted position. Both vocal folds are seen in their entirety. The medial surfaces of the arytenoids are slightly visible, which is normal. The posterior arytenoids (and corniculates) are equal bilaterally and not excessive. Superior processes are equal (left partially covered by cuneiform). Cuneiforms: right slightly anterior to left. Aryepiglottic folds and false cords are equal. The epiglottis is deformed. (B) Normal larynx. The arrows demonstrate how the medial surfaces of the arytenoid cartilages are easily visible. Folds are abducted, and the entire length of both membranous vocal folds is visible.
The “position” of the arytenoids is actually described in relation to the normal (upright) position of the cartilage in the cricoarytenoid joint. At rest, we should be able to see the medial surface of the arytenoids easily, and in addition we should see the entire membranous vocal fold as well (Fig. 13.1B). Deviations from this relationship occur when the arytenoid is tilted in any direction away from its normal vertical location. The position may be described as being normal, too effaced (falling laterally and posteriorly), or too far medial and anterior (covering a portion of the vocal fold).
Arytenoid Movement
Examination of the posterior larynx continues with the gross movements of the arytenoid cartilages. These movements may be described individually for their speed (brisk/fast, normal, sluggish/slow), regularity (smooth, hesitant), and excursion (full, limited in either adduction or abduction). These descriptions give us clues to underlying problems but also make us think constantly about what is happening in the posterior larynx. In the past, the posterior larynx and the movement of the arytenoid cartilages have been an area much overlooked because we did not have the videostrobe in most of our offices, but those times are past.
After examining the individual arytenoid movements, we should then compare one side with the other just as we did with the anterior vocal folds and the mucosal waves. In this regard, we should ask the following questions and describe our results in the overall report:
- Did the arytenoid movements begin at the same time? Stepping through the stroboscopy frame by frame allows us to make this determination.
- Is there underrotation or overrotation of one arytenoid cartilage during phonation?
- Do the vocal folds “line up” at the vocal processes of the arytenoids or is there a vertical height difference between the vocal folds?
Differences in movement onset from side to side and rotational deviations of an arytenoid usually signify synkinetic reinnervation after nerve injury. Disparity in the vertical height of the vocal folds with phonation is sometimes difficult to see in a two-dimensional video. However, it is very important to look for this because an uneven closure of the glottis will cause a voice that sounds worse than it appears during laryngeal visualization from above.
 Observing Voice Production
Observing Voice Production
There is something special about good vocal production. The voice is an intimate part of an individual’s personality, the way one interacts with others, and a beacon of an individual’s health. It is no wonder then that the perception of a voice being “abnormal” raises immediate questions in the listener. As we have outlined earlier, there are specific irregularities of both the anterior and posterior vocal folds that may generate a dysphonic voice and be observed directly. There are also, however, aspects of voice production that are directly responsible for dysphonia that could go unnoticed if we are not thinking of them all the time. It is sometimes helpful to the physician ordering the video to mention these possibilities, not in a long and exhaustive list but as something one has observed during the testing.
The final observations needed from a videostroboscopic examination are those telling us how the vocal folds are working together to produce a sound. For this we need to put the vocal mechanism through its paces with more than just a sustained “a” or “i” sound. Several specific vocal tasks have been found useful, helping to uncover and observe laryngeal function during voicing. With time and practice, we may find equally good or better methods of “stretching the limits” of the voice to uncover somewhat hidden vocal deficiencies, but for now we mention those that have been helpful to date.
Glissando
Voicing from low pitch to high pitch approximates the patient’s vocal range. More importantly, however, observation of the vocal fold stretching during this exercise may uncover a unilateral or bilateral superior laryngeal nerve weakness. Mild weaknesses are not easily identified, so performing this task on every patient gives us a sense of what is normal and what is not. Close observation of shifting or twisting of the larynx (posterior glottis deviation in relation to the horizontal plane of the epiglottis) is still easier to detect than a difference in vocal fold stretching, but if both are present, then the diagnosis may be made (Fig. 13.2).
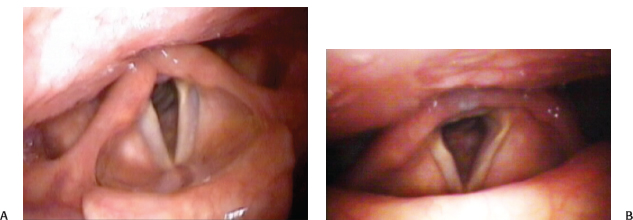
Fig. 13.2 (A) Left superior laryngeal nerve weakness. Notice the asymmetry of tension between the right and left vocal folds. (B) Left superior laryngeal nerve weakness. Note the shift of posterior glottis to the left. The left vocal fold is thinner than the right.
Humming
Producing a humming sound with lips closed usually releases a lot of tension during vocal output. This allows better visualization of the vocal folds with less supraglottic closure from the false cords. In addition, the patient will generally hum in a lower tone, making it easier to see the mucosal waves and any variability from one side to the other. This task is not possible to perform, however, with a rigid endoscope through the mouth but is something that can be done when stroboscopy is being performed with a flexible scope through the nasal cavity.
Voicing at Different Pitches
As just mentioned, the mucosal waves are most easily seen at lower pitches where the amplitude of vibration is greater. At higher pitches, however, we may uncover more disparity between the vocal folds and their mucosal waves. The vocal folds are elongated, thinner, and farther apart during phonation. We may then make observations between the vocal fold mechanism at high pitch when compared with that of low pitch.
Intermittent Voicing
When the voice is produced with short bursts in quick succession, we can see the interactions of the arytenoid cartilages upon each other and how easily the arytenoids move over the cricoarytenoid joints. We can also observe whether or not the internal laryngeal muscles relax quickly or whether there is a delayed relaxation phase. If we suspect or see some delayed relaxation, then we should try at that time to corroborate that finding with possible delayed relaxation of the entire larynx after swallowing. Normal laryngeal movement with swallowing includes a quick upward movement of the larynx of at least 2 to 3 cm followed by a quick relaxation back to baseline. If relaxation is delayed greater than 1 second, then that should be noted in the report. Delayed relaxation is usually caused by neurologic disease, so a consultation with a neurologist should be suggested to the ordering physician in the report if that has not already been done.
 Comments
Comments
Up to this point, we have discussed extensively what needs to be included in a videostroboscopy report to the laryngologist. Because it is not the purview of this chapter to completely explain what the laryngologist will do with this material, one may wonder why all these details were believed to be important at all! Therefore, a short example is given to demonstrate how the information gathered during videostroboscopy is vital to good patient care. This detailed examination may be used not only for uncovering the cause of a vocal problem but also for planning the medical and surgical care necessary for its improvement. We will illustrate this process with a very common problem seen in laryngology, dysphonia secondary to unilateral vocal fold immobility.
Unilateral Vocal Fold Immobility
When a patient presents with immobility of one vocal fold, the physician immediately thinks of a list of possible causes for this abnormality. Problems leading to vocal fold immobility generally include dysfunction of the laryngeal muscle(s), the arytenoid cartilage, or the cricoarytenoid joint. Thus the list includes, but is not limited to, vocal fold paralysis, arytenoid cartilage subluxation (arytenoid cartilage in its joint but out of place), and cricoarytenoid joint arthrodesis (fixation). Videostroboscopy can give us valuable clues in differentiating between these conditions. For instance, an immobile vocal fold with noticeable movement of the muscles attached to the lateral arytenoid (muscular process) may signal an arytenoid subluxation (the arytenoid cartilage being displaced anteromedially or posterolaterally) or a cricoarytenoid joint or joint capsule fixation (trauma, arthritis, fixation after paralysis) (Fig. 13.3).
On the other hand, no noticeable internal laryngeal muscle movement usually signifies a real vocal fold paralysis, and then it becomes important to identify the resulting deficits after muscle atrophy, synkinetic reinnervation, and patient compensations are complete. These factors will determine what kind of surgery is needed for the best laryngeal rehabilitation. In this regard, we are interested in essentially three observations: any opening at the anterior glottis, any opening at the posterior glottis, and any pooling of secretions (mucus) in the piriform sinuses. An open anterior glottis alone may be treated with either injectable materials into the vocal fold or an anterior vocal fold medialization procedure (eg, type I thyroplasty). If the posterior glottis is open during phonation, however, the voice will be very breathy (phonation with one breath lasts for about four syllables), and the patient will have intermittent penetration/aspiration with swallowing (choking, coughing). These symptoms stem from posterior laryngeal incompetence, and closing the anterior glottis alone will not completely rehabilitate the voice and will do nothing to improve swallowing. Something will most likely need to be done to the posterior larynx (arytenoid) to obtain the best surgical outcome, and the operations that best handle posterior glottic deficiencies are the arytenoid adduction procedure (rotating, sliding, and stabilizing the arytenoid cartilage at the midline) or the adduction arytenopexy (a suture fixation of the arytenoid cartilage at the midline). These arytenoid procedures are almost uniformly done in combination with an anterior vocal fold medialization because if the posterior glottis is open, then the anterior glottis will also be open, and past experience and studies have shown that a “direct” approach to both the posterior and the anterior vocal folds gives the highest patient satisfaction.2

Fig. 13.3 (A) Left arytenoid subluxation anteriorly. The arrows point out that the medial surface of the left arytenoid cartilage cannot be seen and that the full length of the left vocal fold cannot be visualized. (B) Another case of arytenoid subluxation. The left arytenoid is falling forward. Again, the medial surface of the left arytenoid cartilage cannot be seen, and the posterior part of the left vocal fold is obscured by the left arytenoid cartilage. Over 50% of the left vocal fold is obscured by the upper arytenoid. The upper rim of the left posterior cricoid is visible. Of note, the patient has fungal laryngopharyngitis.
Lastly, the presence of pooled secretions (saliva, mucus) in the piriform sinus signals real problems with swallowing. Vagal nerve involvement may be just the recurrent laryngeal nerve, resulting in nonrelaxation of the cricopharyngeus muscle (upper esophageal sphincter) or possibly a combination of the recurrent laryngeal nerve plus the pharyngeal branches of the vagus. Whatever the case, a cricopharyngeal myotomy may be added to a combination arytenoid adduction and type I thyroplasty for attempted complete rehabilitation of the patient presenting with a very breathy or aphonic voice and dysphagia. Thus by paying attention to the details seen on clinical examination of the voice and larynx, we now have a more complete picture of why the voice is dysphonic and how we can proceed to help our patient regain more normal laryngeal function.
 Conclusion
Conclusion
Our ability to visualize laryngeal anatomy and physiology to a fine degree has opened up our diagnostic capabilities with disease and dysfunction in this area. Knowledge of what is valuable and important for the laryngologist’s diagnostic workup and what is necessary to capture on a detailed videostroboscopic examination is vital in the overall care of the patient. In the final analysis, a well-done videostroboscopic exam will hasten the time to correct diagnosis, allow for a more thorough laryngeal evaluation, and help uncover the root cause of the dysphonia.
References
1. Hirano M. Phonosurgery: Basic and Clinical Investigations. Nara, Japan: Otologia (Fukuoka); 1975:239–298
2. Slavit DH, Maragos NE. Arytenoid adduction and type I thyroplasty in the treatment of aphonia. J Voice 1994;8:84–91
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


