and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Keywords
Inferior oblique overactionInferior oblique recessionInferior oblique myectomyInferior oblique anteriorizationGraded anteriorizationJ deformityNeurofibrovascular bundleExtirpation/denervation of the inferior oblique muscleHistorically, inferior oblique surgery was considered extremely difficult and was fraught with complications such as fat adherence, ciliary nerve damage with pupillary dilatation, and intraoperative hemorrhage. More recently, however, the management of inferior oblique overaction has improved substantially. The late Dr. Marshall Parks pioneered meticulous techniques that all but eliminated these complications. Another important advance has been the anteriorization procedure.
17.1 Quantification of Inferior Oblique Overaction
Selection of the appropriate surgical procedure is based on the amount of inferior oblique dysfunction. Inferior oblique overaction is clinically estimated on a scale of +1 through +4. When performing versions to test for inferior oblique overaction, make sure the abducting eye is fixing, so the adducting fellow eye is free to manifest an “upshoot.” Quantify the upshoot by bringing the fixing eye straight across to the lateral canthus, and observe the adducting eye for upshoot (Fig. 17.1).
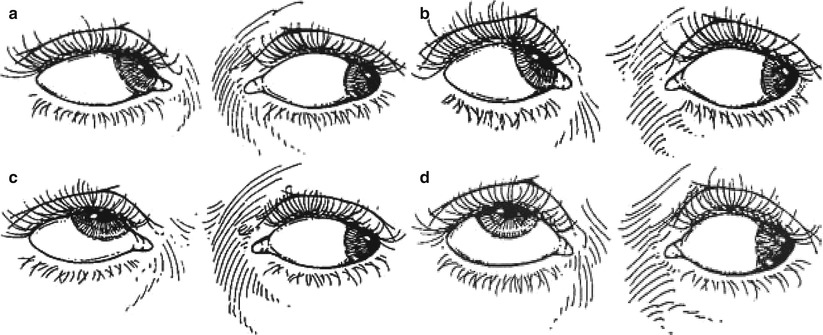
Fig. 17.1
Quantification of upshoot in inferior oblique overaction. Note that the abducting eye (left eye) is the fixing eye and is kept in straight abduction. The adducting eye (right eye) is free to manifest the overaction. One can ensure that the abducting eye is fixing by covering the adducting eye with an occluder or one’s thumb. Look behind the occluder to see the overaction. (a) Minimal upshoot (+1) of adducting eye when taken straight across. Upshoot is better seen when the abducting eye is moved up and out. (b) Upshoot (+2) of adducting eye is obvious when the abducting eye looks straight across at the lateral canthus. (c) Severe upshoot (+3) of the adducting eye is seen even with the abducting eye in straight abduction. (d) Very severe upshoot (+4) of the adducting eye is seen as the fixing eye moves straight across into abduction. In addition to a severe upshoot, there will be an abduction movement as the adducting eye is elevated into the field of action of the inferior oblique
Inferior oblique overaction causes a V pattern–Y subtype, with most of the divergence occurring from primary position to up gaze. The final quantification of inferior oblique overaction should be based on the combined characteristics of the degree of upshoot and amount of V pattern.
17.2 Indications for Surgery
The basic rule of thumb is that patients with +2 or more inferior oblique overaction are candidates for inferior oblique surgery, whereas those with +1 or less can usually be followed. Patients with minimal inferior oblique overaction but a significant V pattern (>15 PD) are exceptions to this rule. These patients should be considered for inferior oblique weakening even though versions show minimal inferior oblique overaction.
Primary inferior oblique overaction is usually bilateral and almost always requires bilateral surgery. In cases of asymmetric overaction, bilateral surgery should be performed even when one eye displays only +1 overaction, to avoid unmasking the minimal overaction. If amblyopia is present (greater than 2 Snellen lines difference), it is safer to restrict surgery to the amblyopic eye. In these patients, monocular surgery is sufficient because the sound eye is always fixing and will not manifest an upshoot.
17.3 Making Procedural Choices
Surgical management of inferior oblique muscle overaction is based on weakening or changing the function of the inferior oblique muscle. The most commonly used techniques include myectomy, recession, and anteriorization. Inferior oblique myotomy is not effective, because the cut ends of the muscle inevitably reunite or scar to sclera, causing residual inferior oblique overaction.
Myectomy weakens the inferior oblique, as removing a portion of muscle reduces the chance of local reattachment (Fig. 17.2a). An inferior oblique recession, on the other hand, acts by inducing muscle slack (thus reducing muscle tension) by moving the muscle insertion closer to the origin, up along the arc of contact of the muscle (Fig. 17.2b). Fink described an 8-mm recession site and Apt and Call [1] subsequently found this site by measuring a point 4 mm posterior and 4.4 mm superior to the inferior rectus insertion. Parks [2] suggested placing the muscle close to the vortex vein for moderate inferior oblique overaction.
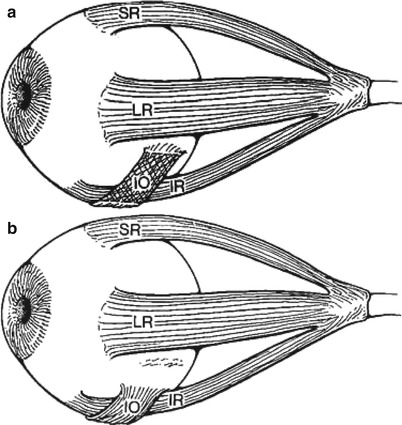
Fig. 17.2
(a) Myectomy. Cross-hatching represents the portion of the temporal inferior oblique (IO) muscle removed in the myectomy procedure. (b) Recession. The muscle is dissected, disinserted, and then reattached along the path of the inferior oblique muscle, but closer to its origin
A newer procedure, the anteriorization procedure (described below), has improved outcomes, especially for the treatment of severe inferior oblique overaction. The graded anteriorization procedure is the authors’ procedure of choice for mild to severe inferior oblique overaction.
17.4 Anteriorization Procedure
The anteriorization procedure changes the vector of forces by moving the inferior oblique muscle insertion anterior towards the inferior rectus insertion (Fig. 17.3). This changes the inferior oblique from an elevator to more of a depressor.
Fig. 17.3
Anteriorization (black) of the inferior oblique (IO) muscle consists of moving the insertion to the temporal border of the inferior rectus (IR) muscle, close to the inferior rectus insertion. Note that the new insertion is parallel to the inferior rectus muscle
17.4.1 Graded Recession: Anteriorization
The basis of the graded anteriorization procedure is that the more anterior the inferior oblique insertion, the greater the weakening effect (Fig. 17.4). This procedure tailors the amount of anteriorization to the amount of inferior oblique overaction. In the mid 1980s, the senior author (KWW) developed a modification of the anteriorization procedure based on keeping the posterior fibers behind the inferior rectus insertion, to prevent limitation of elevation, with a graded anterior placement of the muscle depending on the severity of the inferior oblique overaction. This technique, called “graded anteriorization,” was introduced in 1990, in the first edition of this book. Its results have been excellent, with over 90 % success rate for mild to severe inferior oblique overaction [3].
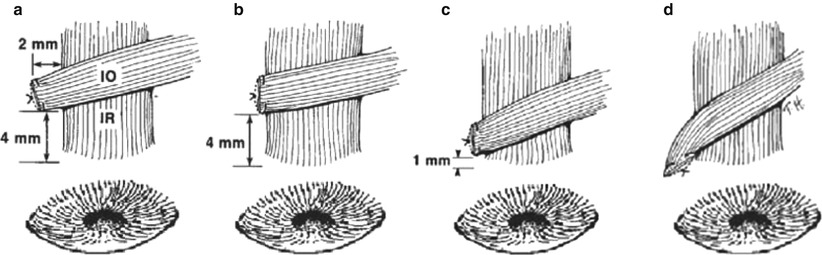
Fig. 17.4
“Graded anteriorization”: The more anterior the new insertion, the greater the weakening effect. (a) The least amount of anteriorization, for minimal inferior oblique (IO) overaction. (b) For moderate overaction, the muscle is placed 4 mm posterior to the inferior rectus (IR) insertion. (c) The anteriorization procedure for severe overaction. (d) Anteriorization of the entire inferior oblique insertion, including the posterior fibers. Anteriorization of the posterior fibers creates a “J” deformity and limits elevation of the eye
Table 17.1 shows the inferior oblique placement for a specific amount of inferior oblique overaction.
Table 17.1
Management of inferior oblique overaction
Overaction | Inferior oblique placement |
|---|---|
+1 | 4 mm posterior and 2 mm lateral to IR insertion |
+2 | 3–4 mm posterior to IR insertion |
+3 | 1–2 mm posterior to IR insertion |
+4 | At IR insertion |
DVD & IOOA | Full anteriorization with “J” deformity (usually bilateral) |
Although Table 17.1 provides guidelines for managing inferior oblique overaction, the final surgical decision must be based on a combination of factors, including the amount of V pattern and the presence of a vertical deviation in primary position. If no vertical deviation is present in primary position, then consider symmetrical surgery. Asymmetric graded anteriorization is indicated if a hypertropia is present. More anteriorization of the inferior oblique should be done on the side of the hypertropia. A full anteriorization (with no “J” deformity) on the side of the hypertropia and 4 mm anteriorization on the opposite side will correct approximately 6 PD of hypertropia. In the case of a unilateral inferior oblique overaction (e.g., associated with congenital superior oblique paresis), an anteriorization with no “J” deformity can correct up to 18 PD of hypertropia. The “J” deformity anteriorization (see below) is associated with limited elevation [4], so it is rarely used, except if performed bilaterally for severe dissociated vertical deviation (DVD) and inferior oblique overaction.
17.4.2 “J” Deformity Anteriorization
Placement of the posterior fibers at (or anterior to) the inferior rectus insertion produces a “J” deformity and will limit elevation of the eye (Fig. 17.5). The complication of limited elevation has been termed by Mims and Wood [4] as the “antielevation syndrome.” Through anatomical dissections, Stager [5] has shown that the neurofibrovascular bundle of the inferior oblique inserts into the posterior fibers and can act as a tether to hold the eye down. He found that the ligamentous structure of the neurofibrovascular bundle provides the ancillary origin for the posterior temporal fibers of the inferior oblique muscle when its insertion is transposed anteriorly. Because of these concerns, full anteriorization with a “J” deformity should be reserved for severe bilateral DVD with inferior oblique overaction. Mims stated that the senior author’s (KWW) procedure of keeping the posterior fibers posterior to the inferior rectus insertion prevents this complication.