Purpose
To determine the incidence of outer foveal defects after macular hole surgery and to evaluate the relationship between the defect and visual outcome.
Design
Retrospective, observational case series.
Methods
A retrospective analysis was performed on 50 eyes from 50 patients who underwent macular hole surgery with a follow-up period of 12 months or more. We evaluated the presence of outer foveal defects using time-domain optical coherence tomography and best-corrected visual acuity at several postoperative time points. The main outcome measures are the incidence of an outer foveal defect and the best-corrected visual acuity.
Results
The incidence of an outer foveal defect at 1, 3, 6, and 12 months after surgery was 49%, 50%, 47%, and 31%, respectively. There were no statistical differences in the postoperative visual acuity between eyes with and without an outer foveal defect at each postoperative time point.
Conclusions
Outer foveal defects after successful macular hole surgery were observed in approximately half of the eyes during the early postoperative period and one third of the eyes at 12 months postoperatively, suggesting that it takes longer than expected to recover the normal foveal anatomy after surgery. The presence of outer foveal defects did not significantly correlate with the visual outcome.
Since the introduction of vitrectomy for the treatment of macular hole in 1991, vitreous surgery has become the standard in therapy for the disease. The success rate of macular hole surgery after the introduction of the internal limiting membrane peeling technique has been reported to be as high as 85% to 100%.
Optical coherence tomography (OCT) has become the gold standard for the diagnosis of macular hole and for confirming the anatomic closure of the macular hole after surgery. Recent innovations in OCT enable the detailed observation of retinal anatomy, including the photoreceptor layer. Previous reports suggested that repair of the photoreceptor layer was associated with visual improvement after macular hole surgery.
In the process of macular hole closure, bridging of the inner retina was first observed. In the early postoperative period, therefore, OCT occasionally demonstrated hyporeflective defects in the outer fovea. In fact, several reports have documented the hyporeflective defects using OCT after macular hole surgery or after spontaneous closure of macular holes. However, there is little information about the incidence of this anatomic change following macular hole surgery. Additionally, the relationship between the presence of outer foveal defects and the visual outcome has not been fully understood.
The purpose of this study was to determine the incidence of an outer foveal defect after successful macular hole surgery. Also, we investigated the possible correlation between the presence of an outer foveal defect and the visual outcome.
Methods
We retrospectively reviewed patient records to identify patients who underwent pars plana vitrectomy for idiopathic macular holes performed by a single surgeon between December 1, 2004 and July 31, 2008 at a single, referral-based hospital. Inclusion criteria were stage 2-4 idiopathic macular hole and a 12-month or longer follow-up after surgery. Patients with myopia greater than 6 diopters, symptoms longer than 12 months, or history of vitreous surgery were excluded. Also excluded from the study were patients with failure to close the macular hole. Therefore, a total of 50 eyes from 50 patients (15 male and 35 female; mean age, 65.6 years) were included in this study. The study included 19 in stage 2 macular hole, 22 in stage 3, and 9 in stage 4. The staging of the macular hole was determined by slit-lamp examination and classified according to Gass classification.
Surgery was performed by a single surgeon. Informed consent was obtained prior to surgical intervention in all patients. A standard 3-port pars plana vitrectomy was performed in all patients using retrobulbar anesthesia. The crystalline lens was removed by phacoemulsification followed by intraocular lens implantation before pars plana vitrectomy in phakic eyes. After core vitrectomy, the posterior vitreous was separated from the retina, if still attached. The internal limiting membrane (ILM) peeling was performed using a microvitreoretinal blade and vitreoretinal forceps after staining the ILM with triamcinolone acetonide. After a fluid-air exchange, an air-gas exchange was performed using 20% sulfur hexafluoride (SF6), and the patient was asked to maintain a face-down position for at least 5 days.
The patients underwent complete ophthalmologic examinations including best-corrected visual acuity measurements, slit-lamp biomicroscopy, indirect ophthalmoscopy, fundus photography, and OCT examinations. Before surgery, the macular hole size was recorded using OCT, specifying its minimum, or aperture, diameter from the closest lip of the hole to its center. Preoperative examinations were performed the day before the macular hole surgery, and follow-up was scheduled at 1, 3, 6, and 12 months after the surgery. At each visit, all patients underwent visual acuity measurements, indirect ophthalmoscopy, slit-lamp examinations, fundus photographs, and OCT.
OCT examinations were performed using Stratus OCT (Carl Zeiss Meditec, Inc, Humphrey Division, Dublin, California, USA) after pupil dilation using fixation on an internal target to define the center of the fovea and recording 10 horizontal transfoveal scans and 10 vertical scans by a single expert examiner. Particular attention was paid to the outer layers of the fovea, especially outer foveal hyporeflective defects over the retinal pigment epithelium (RPE). If at least 1 of the scans showed an outer foveal defect, the scans from that eye were selected for analysis.
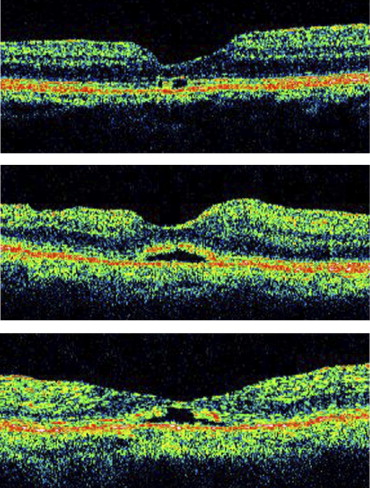
The definition of outer foveal defect for the purpose of this study was the appearance of an outer foveal hyporeflective defect on OCT images. We divided the outer foveal defects seen on OCT into 4 groups: outer layer defect, foveal detachment, complex, and unclassified ( Figure 1 ). The outer layer defect type included a complete disruption of the photoreceptor inner and outer segment (IS/OS) junction with a hyporeflective empty space between them. The foveal detachment type included an elevation of the outer foveal layer with a continuous IS/OS junction. The complex type demonstrated foveal detachment with a disruption of IS/OS junction.
Visual acuity data were converted to the logarithm of the minimal angle of resolution (logMAR) and analyzed using StatView software (Abacus; Abacus Concepts, Inc., Berkeley, California, USA). The t test was used to compare preoperative and postoperative visual acuities.
Results
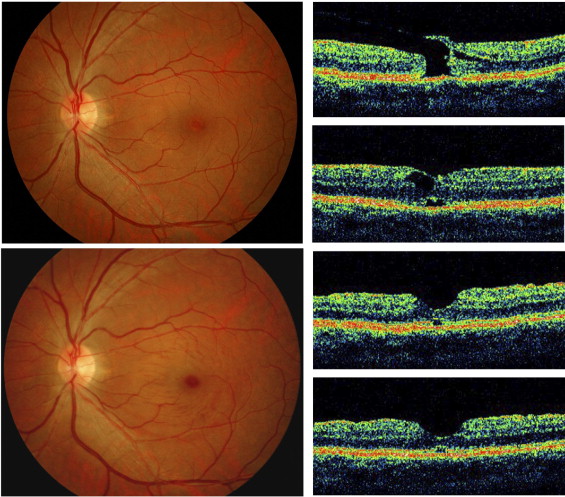
The incidence of an outer foveal defect at 1, 3, 6, and 12 months was 49% (23/47), 50% (21/42), 47% (17/36), and 31% (15/48), respectively ( Table 1 ). The types of outer foveal defects in the 23 eyes at 1 month included outer layer defects in 18 eyes (78%) and foveal detachment in 4 eyes (17%). At 12 months, all 15 eyes with defects were classified as outer foveal layer defects ( Figure 2 ).
| Postoperative Time | ||||
|---|---|---|---|---|
| 1 Month | 3 Months | 6 Months | 12 Months | |
| Outer layer defect | 18 (78%) | 20 (95%) | 16 (94%) | 15 (100%) |
| Foveal detachment | 4 (17%) | 1 (5%) | 0 | 0 |
| Combined | 1 (4%) | 0 | 0 | 0 |
| Unclassified | 0 | 0 | 1 (6%) | 0 |
| Total | 23/47 (49%) | 21/42 (50%) | 17/36 (47%) | 15/48 (31%) |
We compared the preoperative and postoperative characteristics between eyes with and without an outer foveal defect at each visit. There were no statistical differences in visual acuity at the 12-month follow-up time point between eyes with and without defects ( Table 2 ). Also, preoperative macular hole stage was not associated with the presence of defects. Eyes without an outer foveal defect had better improvement in visual acuity, but the difference was not statistically significant. Similar results were found at the 1-, 3-, and 6-month follow-up examinations, although preoperative macular hole size was significantly smaller in eyes with a defect than in eyes without a defect at the 1-month visit (365 μm vs 464 μm).



