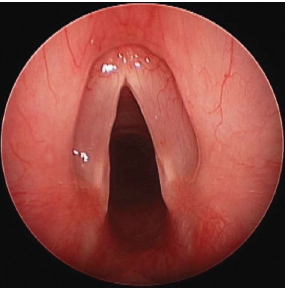
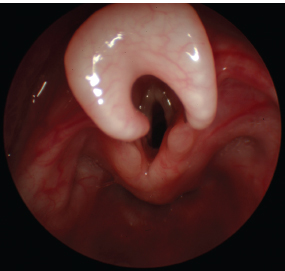
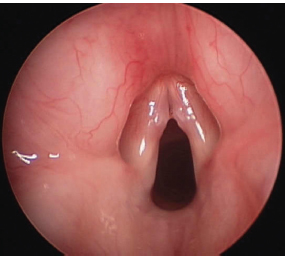
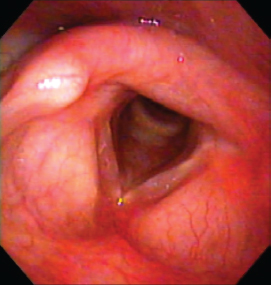
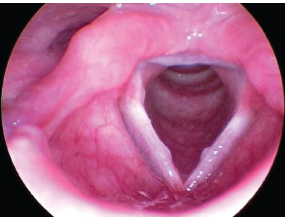
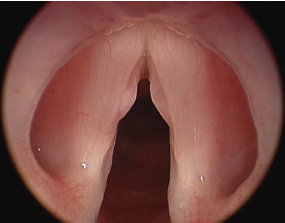
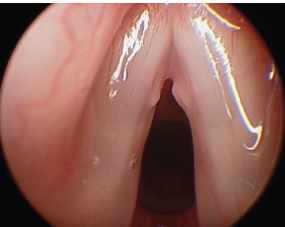
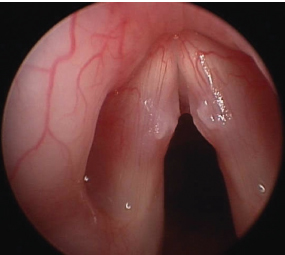
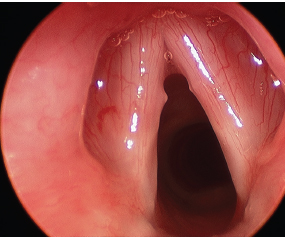
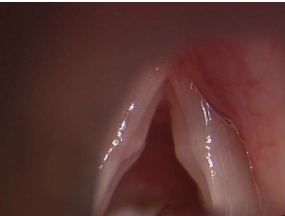
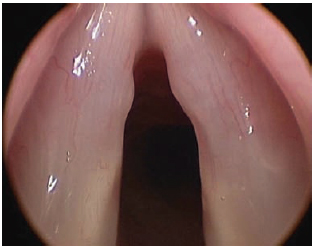
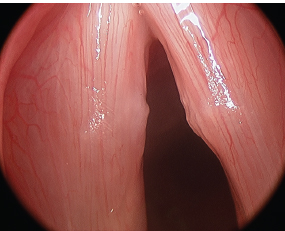
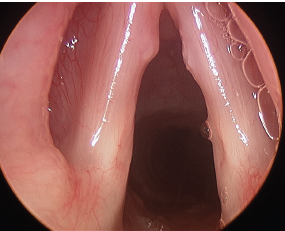
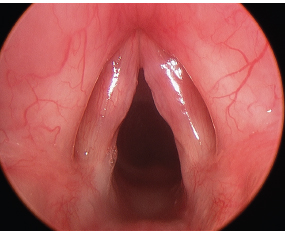
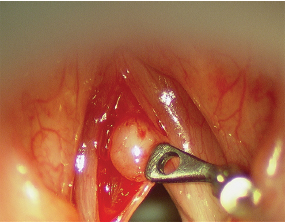
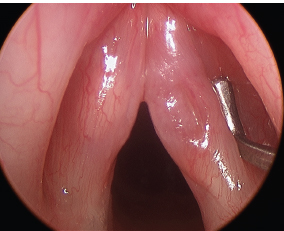
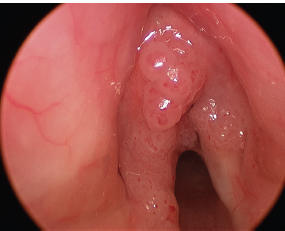
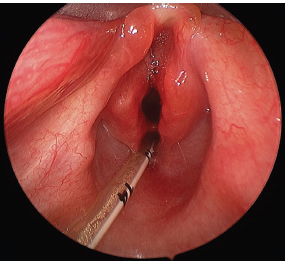
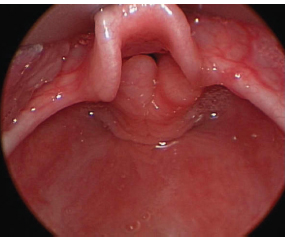
27 Children are increasingly presenting to clinicians for the evaluation of hoarseness. As young individuals, they pose their own set of difficulties. They often have no awareness, understanding, or interest in the reason for which they have been referred to the specialist. With this in mind, it is easy to understand why they may not be as cooperative as adults who seek an evaluation of their own accord. The evaluation of the hoarse child, however, is no less important than that of an adult. An accurate diagnosis is essential for appropriate management, which may prove to be lifesaving. Visualization of the laryngeal structures is the mainstay of accurate diagnosis. The techniques used to visualize the adult larynx may also be used in children (Fig. 27.1). Smaller versions of fiberoptic and rigid endoscopes are available but often pale in clarity, resolution, and light delivery. As technological advances are made in endoscopy, advances are also made in the office evaluation of the pediatric larynx. It should be stated early, however, that operative endoscopy via a general anesthetic for an accurate diagnosis should be offered if sufficient visualization cannot be obtained in the clinic and if the endoscopist feels confident in his or her operative skills, support, and facility. A missed or delayed diagnosis from failure to adequately visualize the larynx is not acceptable. The developing pediatric larynx also has a different appearance from the fully developed adult larynx. As the larynx descends into the neck of the adult, the supraglottic structures open up, exposing the true vocal folds for easier visualization. The infantile omega-shaped epiglottis and foreshortened aryepiglottic folds can at times obscure complete visualization of the child’s glottis (Fig. 27.2). The true vocal folds are also shorter in the child than in the adult. Not only are the vocal folds shorter, but also the ratio of the membranous vocal fold to the cartilaginous vocal process is nearly 1 to 1, much smaller than that in the adult (Fig. 27.3). The position and shape of the pediatric larynx dramatically differs from that of the adult. Fig. 27.1 Normal pediatric larynx seen during direct rigid endoscopy. Fig. 27.2 The omega-shaped epiglottis and shortened aryepiglottic folds make visualization of the true vocal folds more difficult in this 18-month-old child. As those who treat children know, the child is not the only patient in the room. The parents also must be involved and committed to the evaluation. An anxious parent will unknowingly and unwittingly transmit their anxiety to their child, making an occasionally difficult task nearly impossible. The key to a successful evaluation is to include both parent and child in the discussion of what will happen and what will be gained from the experience. With these issues properly addressed and with a calm and supportive parent, children are capable of cooperating with a thorough endoscopic evaluation. Fig. 27.3 These vocal nodules in the pediatric larynx extend across the total distance of the membranous fold. The ratio of the membranous fold to the vocal process is nearly 1 to 1. Videotaping the laryngeal examination is extremely useful for many reasons. If the child is less than cooperative or if only glimpses of the larynx are obtained, documentation with videotape allows for replay, slow replay, and freeze-frame analysis of the larynx. Later comparisons of the laryngeal status are also important to track the progress of treatment. The usefulness of videotaping with frame-by-frame analysis cannot be emphasized enough. It allows the endoscopist to concentrate on obtaining the images during the endoscopy while affording replay for later review, reassessment, and for explanation of salient physical findings to the parent and child. The introduction of fiberoptic endoscopy has added tremendously in the evaluation of the aerodigestive tract in all age groups. With advancing technology, smaller fiberscopes are becoming available. This has allowed for the use of fiberscopes in even the youngest neonates for visualization of the functioning velopharynx, hypopharynx, and larynx. It is the rare case when a child cannot be evaluated by flexible endoscopy. Small, distal chip camera endoscopes, allowing for a more functional evaluation of the larynx, will likely someday completely replace the rigid angled telescope for laryngoscopy. This will especially hold true as optical quality improves (Fig. 27.4). The choice of fiberoptic endoscope is based on its size, optical clarity, ability to couple with the video-recording source, and its durability. The endoscopist should trial each prospective endoscope with his or her own video system to be certain that the image is acceptable. Smaller endoscopes allow for more comfort for the patient and therefore a longer and more agreeable evaluation, although their durability and optical quality at times are an issue. Fig. 27.4 Notice the clarity of this fiberoptic image in this office visualization of the larynx with a flexible, distal chip tip endoscope in a child. Time, perhaps, is the most important component that leads to successful and thorough endoscopy. Time in explanation, time of preparation, and length of time of the examination will significantly enhance the evaluation. Children will be more acceptable to a procedure if they understand the reasons, the expectations, and the agreed upon limits prior to proceeding. Child-friendly terms, consistency, and trust are essential for successful endoscopy. As would be expected in an adult, if the patient does not trust the endoscopist or understand what to expect, cooperation will be minimal. Children should be approached with the same concern and compassion. An accurate and complete description of the procedure should be given to the parents. If this can be done prior to the office visit, it is optimal. If the parent understands and “buys” into the procedure, it will be much easier to “sell” to the child. Children are masters at observing subtle cues from their parents to help them make decisions regarding their safety and well-being. An anxious parent may unwittingly transfer anxiety to his or her child. Topical anesthesia and decongestion can be helpful in preparing the pediatric nose for the endoscope. Care should be taken in the very young, however, as significant but transient dysphagia and reflex apnea can occur. Lidocaine and oxymetazoline are the most common agents used in combination prior to the insertion of the flexible fiberscope. The flavor and sensation of atomized nasal sprays can also be disagreeable, however. This can usually be overcome with a lollipop of the child’s choice prior to the spray. This can help mask the flavor as well as act as a reward for positive behavior. If a child is unable to sit comfortably alone for flexible endoscopy, the parent may be enlisted to help with gentle restraint. With the parent seated in the endoscopy chair, the child can sit on the parent’s lap. The parent can then give the child a gentle hug and control the hands and arms. An assistant can also help steady the head. The amount of physical restraint is kept light as long as the child does not move or reach for the fiberscope (Fig. 27.5). Demonstration of the action of the endoscope, capturing a head shot of the patient with the endoscopic camera and allowing the child to feel the fiberscope prior to insertion, can also be helpful to induce trust of the child. Once the endoscopy has begun, stops along the way can be made to accommodate the child. With brief stops during insertion at the child’s request, the child gains the understanding that he or she has some control during the endoscopy, and the procedure can then generally proceed with fewer interruptions. Once the endoscope is positioned, it should be left in place until the child can settle. When the movement of the scope ceases, discomfort and anxiety decreases and cooperation increases giving a better assessment. Again, videotaping the examination allows for later explanation of the visualized structures to both the child and the parent. Frame-by-frame analysis can also be used when only brief glimpses of the desired anatomy are seen. Biofeedback can also be used and demonstrated with the videoendoscopy. The advantage of the flexible endoscope is its nearly universal utility. It would be extremely unlikely that a child could not be examined by a fiberscope. It also allows for the functional evaluation of the nasal cavity, velopharynx, hypopharynx, larynx, and swallow, which cannot be done with the rigid endoscope. The disadvantage to the fiberscope lies in its relatively poor optics and at times inadequate light delivery for videostroboscopy. Fig. 27.5 This child is undergoing fiberoptic nasopharyngoscopy. The child is seated in the parent’s lap who hugs him and controls his hands and arms. An assistant, a speech pathologist, steadies the head with gentle restraint. Cooperative children, generally over the age of 5, can also be examined by the rigid endoscope. The advantages of the rigid angled endoscope are its clarity, quality, and brightness. Videostroboscopy has been found to be helpful in evaluating mucosal and submucosal lesions (Fig. 27.6). The typical 10-mm angled rigid endoscope can be used in most instances. Occasionally, the oropharyngeal inlet is narrowed by tonsillar hypertrophy. This can make insertion of the 10-mm endoscope difficult. Smaller angled telescopes are available and have been found to be useful. A 4-mm narrow-view angled endoscope with the light post on the viewing side has been helpful in children with large tonsils. The narrower or less blunt tip of the smaller endoscopes, however, can feel sharper in the posterior pharynx if the mucosa is touched, and so care must be taken to avoid contact with the pharyngeal walls. Superior light and optics, however, are provided by the rigid endoscopes. The techniques and preparation for rigid indirect laryngoscopy in children are similar to those used in adults. A clear, age-appropriate explanation of the procedure is very helpful in obtaining patient compliance. Although it is up to the endoscopist’s preference, fiberoptic endoscopy is often performed first to obtain an image of the larynx. If tolerated reasonably well, then rigid endoscopy can be introduced. This guarantees that some images of the larynx will be obtained yet it affords a chance to record images of the larynx with greater clarity, as well. Again, it should be emphasized that video recording during the endoscopy is extremely useful. Fig. 27.6 Bilateral vocal nodules with posterior glottic edema and pachydermy consistent with laryngopharyngeal reflux observed via office rigid videoendoscopy. There are times during the evaluation of the pediatric larynx when office visualization does not yield an accurate diagnosis. Children may not be able to adequately comply with the fiberoptic exam in the office while awake. An incomplete examination due to anatomic issues, poor cooperation, or if the accuracy of the diagnosis is in question due to a failure in treatment are indications for further physical examination. In these instances, it may be necessary to take the child to the operating room for further evaluation. It may be that operative endoscopy, with a general anesthetic, is required to allow a thorough and more complete visual as well as tactile examination of the larynx (Fig. 27.7). Although the techniques are similar to adult microlaryngology, in pediatric microlaryngol-ogy the instrumentation is smaller, airway management has different concerns, and the general anesthetic is often approached differently. This tool and approach, however, should be an integral part of the assessment of the pediatric larynx. Requirements for pediatric direct laryngoscopy include the appropriate instrumentation, support staff, and expertise to perform operative endoscopy. Comfort with the management of the pediatric airway is essential to the safe and accurate assessment of the pediatric larynx during general anesthesia. Beyond the expertise of the surgeon, a well-trained operating room staff and an anesthesiologist comfortable with the pediatric patient and airway are also required. Fig. 27.7 These are symmetric vocal nodules at the midpoint of the membranous vocal fold. Again, the membranous to cartilaginous vocal fold ratio is 1 to 1. Telescopic examination or microscopic examination of the pediatric vocal folds may uncover pathology that was not otherwise recognized in the office. It has been shown by Dailey et al. that office endoscopy can miss or incorrectly diagnose 10 to 20% of adult laryngeal pathology.1 Although this has not been studied in the pediatric larynx, it is likely that similar if not higher inaccuracies occur. An accurate assessment and diagnosis is required for proper treatment regimens. There are many different techniques for operative endoscopy in the pediatric larynx. Spontaneous ventilation with direct assessment of the vocal folds by telescopes, whether zero-degree or angled, or by a microscope gives a magnified view of the vocal fold. Comfort with microlaryngeal surgical techniques is important for the evaluation of the pediatric larynx. Palpation of the vocal folds is then possible to assess for the presence of an intracordal cyst. Sulcus vocalis may also be recognized with palpation and manipulation of the vocal fold itself. Recognition of lesions other than vocal nodules is important, as these pathologic conditions may require vastly different therapies including surgery. Fortunately, the most common finding in a dysphonic child is vocal nodules. Vocal nodules are a thickening of the superficial layers of the vocal fold in discrete areas generally in the middle of the membranous vocal fold. Although attributed to vocal trauma, the exact etiology for vocal nodules is not known. Quiet children can have vocal nodules, whereas screamers may not. Vocal nodules also have different appearances. Soft tissue lesions that are often diagnosed as vocal nodules may have very different physical appearances. This also confirms our lack of understanding of the etiology of vocal nodules (Figs. 27.8 to 27.15). It is important that the pediatric voice specialist be able to recognize different lesions of the vocal fold. It may be especially difficult to distinguish between a submucosal cyst and a vocal nodule in children (Fig. 27.16). This differentiation is exceedingly important, however, as the primary treatment regiment is vastly different. Intracordal cysts may require surgical intervention or removal, whereas vocal nodules are often successfully treated with voice therapy alone (Fig. 27.17). Fig. 27.8 Small asymmetric nodules and anterior vocal fold. Fig. 27.9 Larger left vocal nodule with asymmetry when compared with the right vocal fold. Fig. 27.10 Bilateral nodules with an angry thickened mucosal covering. Fig. 27.11 Small but symptomatic nodules in the mid-membranous portion of the vocal folds. Fig. 27.12 Mildly asymmetric vocal fold nodules in a pediatric larynx. Fig. 27.13 Small symmetric nodules. Fig. 27.14 Small nodules of different size and consistency. Fig. 27.15 These nodules have some asymmetry. There was no evidence of an intracordal cyst on closer examination. Sulcus vocalis is a pocket of mucosa that extends deep into the lamina propria. Sulcus vocalis lesions have been classified as superficial to very deep, with extension and occasionally scarring to the vocal ligament (Fig. 27.18). As it is in adults, the treatment of sulcus vocalis in children is controversial. Excision of this lesion without subsequent scarring is exceedingly difficult. Voice therapy alone, however, may not resolve the dysphonia. Despite the controversy in treatment modalities, an accurate diagnosis is helpful, as it may explain an inadequate or incomplete response to appropriate voice therapy. Viral lesions from the human papilloma virus are the most common mass lesions on the pediatric larynx (Fig. 27.19). They may recur and cause significant voice disturbance as well as respiratory embarrassment. Significant airway obstruction can result from growth of these viral lesions. Office endoscopy is usually diagnostic and may also be used to follow the course of the disease, but surgical intervention is often required for debulking the viral growths to prevent obstruction of the airway. Fig. 27.16 The left vocal fold has an intracordal cyst. The only hint of the cyst is the yellow hue to the submucosal mass. The cyst was confirmed by exploration of the vocal fold. The right or contralateral side has a sulcus vocalis. Fig. 27.17 An intracordal cyst is seen through an incision in the left vocal fold. Fig. 27.18 On the right true vocal fold, the lesion seen is a pocket of mucosa, invaginating into the lamina propria, sulcus vocalis. The left vocal fold has an intracordal cyst. Fig. 27.19 Recurrent respiratory papilloma across the vocal folds and anterior commissure. Congenital anomalies of the larynx may present in newborns or later in children. A few examples of congenital anomalies of the larynx include glottic web, laryngotracheal cleft, laryngomalacia, and supraglottic or saccular cysts (Figs. 27.20 to 27.22). Many of these are readily identifiable with office endoscopy, but some require direct laryngoscopy for confirmation. Fig. 27.20 A small laryngeal web is seen across the true vocal folds. Fig. 27.21 This larynx has a large laryngotracheal cleft. There is a congenital cleft in the posterior glottis, between the arytenoids extending down through the cricoid cartilage. The tube seen is inserted into the esophagus, and the cleft is seen anterior to it. Fig. 27.22 The arytenoids are seen prolapsing into the glottis inlet in this patient with laryngomalacia.The shortening aryepiglottic folds were incised, and the prominent cuneiform cartilages were trimmed to treat this patient. Pediatric laryngeal pathology should be readily assessed with diagnostic endoscopy. Endoscopy may be performed in the office or in the operating room under general anesthesia. The tools and techniques are similar to those used for assessing adults. The approach, however, may be different. It is important to modify the approach to the child and the parent in the evaluation of the pediatric patient for successful diagnosis and treatment. 1. Dailey SH, Spanou K, Zeitels SM. The evaluation of benign glottic lesions: rigid telescopic stroboscopy versus suspension microlaryngoscopy. J Voice 2007;21:112–118
Imaging in Pediatric Patients
 Fiberoptic Endoscopy
Fiberoptic Endoscopy

 Rigid Endoscopy
Rigid Endoscopy
 Operative Endoscopy
Operative Endoscopy
 Common Findings in Pediatric Laryngeal Imaging
Common Findings in Pediatric Laryngeal Imaging


 Conclusion
Conclusion
Reference
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


