Chapter 62 Hypoglossal Facial Anastomosis
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
Connection of a graft with the normal facial nerve followed by redirection of some of these fibers to the paralyzed side is termed cross-facial grafting. This method can provide some symmetry of movement, while avoiding other motor deficits. This procedure partially compromises the normal nerve, however, and provides a scant supply of neural elements to the recipient muscles, leading to inconsistent results.1,2 As a consequence, this procedure has not met with widespread acceptance.3,4 Combinations of cross-facial grafting and traditional nerve substitutions may also be employed.5–8
Nerve/muscle pedicle grafts such as temporalis muscle transfer have been used with some success, but have also yielded inconsistent results.9 Because the results of nerve/muscle pedicle grafts and cross-facial grafts have been disappointing, modifications of these procedures have been developed that use combination cross-facial grafting and microvascular free muscle flaps for facial reanimation.9,10 More recently, a modification of the traditional temporalis transfer has been used that incorporates the temporalis tendon alone instead of a portion of the muscle.11
PATIENT SELECTION
In cases of known facial nerve discontinuity in which direct repair or grafting is impossible, the CN XII/VII anastomosis should be performed as soon as reasonably possible. Muscle atrophy and degeneration proceed rapidly after denervation.12 Early repair provides axonal growth to the muscles and limits the amount of muscle degeneration.
The severed nerve also begins to experience fibrosis.13,14 In early anastomoses, new axons fill the nerve sheath before fibrosis and potentially allow a greater supply of axons to the muscles. Although earlier anastomosis gives a better functional result, the CN XII/VII anastomosis is also effective after a prolonged denervation and should be considered up to 2.5 years after injury.4,15 Return of function can occur 4.5 years after injury.16
SURGICAL TECHNIQUE
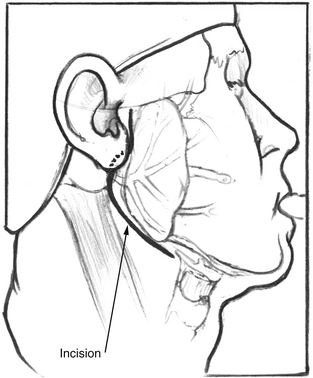
After satisfactory general endotracheal anesthesia has been obtained with the patient in the supine position, the neck is extended, and the face is turned toward the side opposite the paralysis. The ear, face, and neck are prepared and draped using sterile technique. A standard lazy S parotidectomy incision is made in the preauricular crease and extended behind the lobule and then anteriorly about 2 cm below the angle of the mandible (Fig. 62-1). In cases where the patient has had a prior postauricular incision for craniotomy, the postauricular incision may also be used for the superior aspect of the incision. This is particularly true if a mobilization of the facial nerve out of the fallopian canal is planned.
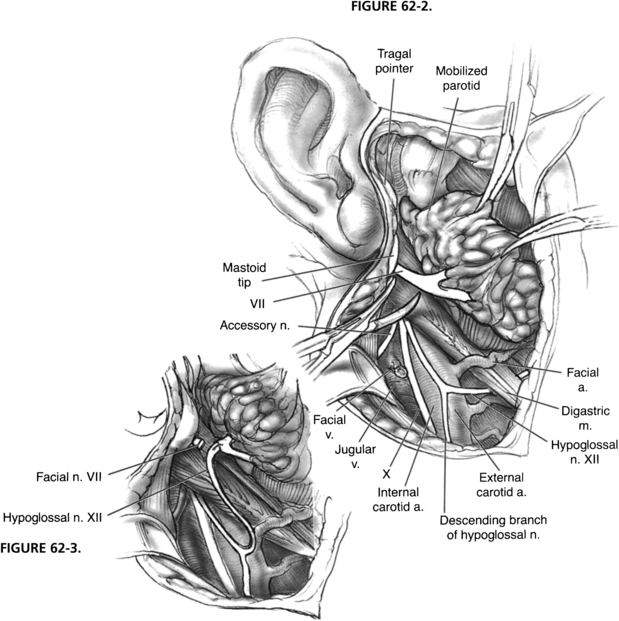
The hypoglossal nerve is identified by retracting the sternocleidomastoid muscle posteriorly and exposing the great vessels of the neck. The posterior belly of the digastric muscle is retracted superiorly, and the hypoglossal nerve is found coursing inferiorly with the great vessels and then turning anteriorly as it supplies the ansa cervicalis, which descends in the carotid sheath (Fig. 62-2). The hypoglossal nerve is followed anteriorly and medially as it enters the tongue muscle. The nerve is freed from its fascial attachments in the neck. The network of veins and arteries entering the internal jugular vein and external carotid artery should be controlled during this maneuver. After the nerve is freed from its attachments, it is divided as far anteriorly as is possible to gain sufficient length. The free hypoglossal nerve is rotated superiorly. Directing the nerve medial to the digastric muscle in this rotation gives the most length, but is unnecessary for a satisfactory anastomosis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


