Chapter 49 Hypertension
Introduction
Hypertension is the leading risk factor for cardiovascular disease (CVD) and mortality worldwide,1 with a projected number of 1.56 billion individuals with hypertension by 2025.2
Hypertension has profound effects on both the structure and function of the vasculature in the eye. The retinal, choroidal, and optic nerve circulations undergo a range of pathophysiological changes in response to elevated blood pressure resulting in a spectrum of clinical signs known as hypertensive retinopathy, choroidopathy, and optic neuropathy, respectively.3 Hypertension is also a major risk factor for many other eye diseases, including the development and progression of diabetic retinopathy,4 retinal vein occlusion,5 retinal arterial macroaneurysm,6 and possibly age-related macular degeneration and glaucoma.3,7
Hypertensive retinopathy
Definition and classification
Retinopathy is the most common manifestation of hypertension which develops due to acute and/or chronic elevations in blood pressure. Hypertensive retinopathy is broadly divided into different stages.8 The initial response to elevated blood pressure is vasospasm and an increase in vasomotor tone, with consequent narrowing of retinal arterioles to control for optimal blood volume (“vasoconstrictive” phase). This stage is seen clinically as generalized or diffuse retinal arteriolar narrowing.
Very severe hypertension (i.e. “malignant hypertension” phase) may lead to optic disc swelling which may reflect underlying hypertensive encephalopathy with raised intracranial pressure.3,7–9
The above phases of hypertensive retinopathy are not always sequential. For example, in patients with acutely raised blood pressure, signs of retinopathy reflecting the “exudative” stage (e.g. retinal hemorrhage) may be present without features of the “sclerotic” stage (e.g. arteriovenous nicking). Furthermore, elevated blood pressure does not fully explain all the pathophysiological mechanisms of hypertensive retinopathy. Other processes involved in the pathogenesis of hypertensive retinopathy signs include inflammation,10 endothelial dysfunction,11 abnormal angiogenesis,12 and oxidative stress.13 In fact, hypertensive retinopathy signs are detected frequently in persons without a known history of hypertension.14
There have been many different classifications for hypertensive retinopathy. Traditionally, the Keith–Wagener–Baker system classifies patients with hypertension into four groups of increasing severity.15 However, it is difficult to distinguish early retinopathy grades (e.g. group 1 signs are not easily distinguished from group 2 signs).9,16 A simplified classification of hypertensive retinopathy based on prognosis of different signs from recent population-based data has been proposed9:
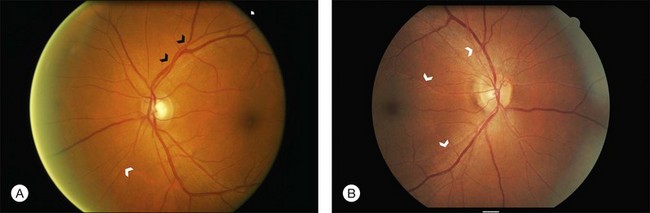
2. Mild: Generalized arteriolar narrowing, focal arteriolar narrowing, arteriovenous nicking, arteriolar wall opacification (silver or copper wiring), or a combination of these signs (Fig. 49.1).
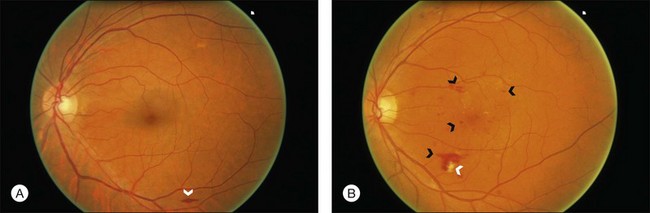
3. Moderate: Hemorrhages (blot, dot, or flame-shaped), microaneurysms, cotton-wool spots, hard exudates, or a combination of these signs (Fig. 49.2).
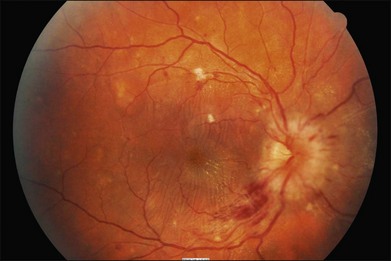
4. Malignant: Signs of moderate retinopathy in combination with optic disc swelling, in the presence of severely elevated blood pressure (Fig. 49.3).
Recently, the application of digital retinal photography and imaging software has allowed measurements of retinal vessel widths to quantify generalized arteriolar narrowing objectively.17,18 Studies using such methods show that generalized retinal arteriolar narrowing is strongly related to blood pressure and risk of hypertension.19,20 There is also evidence that retinal venular diameter may convey independent prognostic information.21 However, the measurement of retinal vessel width using these methods require specialized computer software and trained technicians and is thus not yet widely available for clinical use.
It has been argued that the clinical assessment of hypertensive retinopathy signs is of limited additional value in the management of patients with hypertension.22 Most international hypertension management guidelines, however, including those of the US Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC), the British Society of Hypertension and the European Society of Hypertension (ESH), and the European Society of Cardiology (ESC),23–25 still emphasize that hypertensive retinopathy, with left ventricular hypertrophy and renal impairment, is an indicator of target organ damage, and that its presence should be an indication for a more aggressive approach in managing these hypertensive patients.24 Whether the retinal examinations should be performed by physicians using the direct ophthalmoscope, by ophthalmologists, or via standardized assessment using digital retinal photography remains unclear.
Epidemiology
In the past 30 years, epidemiological studies that have used retinal photography and standardized assessment methods to document and define hypertensive retinopathy have contributed to a greater understanding of the epidemiology, risk factors, and systemic associations of hypertensive retinopathy signs in the general population with different racial samples.26
With the exception of optic disc swelling, hypertensive retinopathy signs are generally common in persons 40 years of age or older, even in the absence of diabetes mellitus, with prevalence ranges from 2 to 17%.27–33 These studies also demonstrate that hypertensive retinopathy signs increase with age, and may vary by race/ethnicity (Chinese have a higher prevalence of hypertensive retinopathy than Caucasian whites) and possibly gender (men have higher rates than women).
While it is well established that hypertensive retinopathy signs are strongly correlated with blood pressure levels,26,34,35 new epidemiological studies show three particularly interesting features. First, there is now good evidence that some signs, particularly generalized retinal arteriolar narrowing, may precede the development of hypertension.19,20,36 In some studies, normotensive persons with this sign were more likely to develop hypertension and, among those with mild hypertension, were more likely to develop the severe stages of hypertension.37 Thus, generalized retinal arteriolar narrowing, possibly reflecting more widespread systemic peripheral vasoconstriction, may be an early preclinical marker of hypertension.
Second, new studies in children have demonstrated that the association between retinal arteriolar narrowing and elevated blood pressure can be observed even in children as young as 4–5 years of age. These findings suggest that the impact of elevated blood pressure on the retinal microcirculation occurs in early life,38,39 which may then “track” through to adulthood, even before the onset of overt hypertension.
Third, there is now evidence to show that the patterns of associations of specific retinopathy signs vary with current and past blood pressure levels. Generalized retinal arteriolar narrowing and arteriovenous nicking, for example, are related not only to current blood pressure levels, but also to blood pressure levels measured in the past, suggesting these two retinal signs reflect the cumulative effects of long-standing hypertension and are persistent markers of chronic hypertensive damage. In contrast, focal arteriolar narrowing, retinal hemorrhages, microaneurysms and cotton-wools spots are related only to concurrently measured blood pressure, mirroring the effects of short-term blood pressure changes.35
Finally, retinal venular diameter, not traditionally considered part of the spectrum of hypertensive retinopathy signs, may convey additional information regarding the state of the retinal vasculature and systemic health. Studies found that retinal venular widening or dilation is also related to elevated blood pressure levels,20,21,34,40 suggesting that the venule may exhibit different optimal flow characteristics across the vascular network compared with arterioles in the presence of hypertension.41 Whether retinal venular dilation should be included as part of the classification of hypertensive retinopathy remains unclear at this time.
Relationship with stroke
In one large multicenter US study, middle-aged, generally healthy persons with moderate hypertensive retinopathy signs were more likely to have subclinical MRI-defined cerebral infarction, cerebral white matter lesions, and cerebral atrophy than those without these signs.42–45 Furthermore, persons with moderate hypertensive signs at baseline were more likely to develop an incident clinical stroke,46 incident lacunar stroke,47 cognitive impairment,48 and cognitive decline49 than persons without these signs, even controlling for traditional risk factors. Another large cohort study based in Rotterdam, Netherlands, have further reported associations of larger retinal venular diameter with incidence of hemorrhagic stroke and the development of dementia.50,51
Some recent studies further demonstrated that hypertensive retinopathy may allow further refinement and subtyping of stroke. In a multicenter study of patients with acute stroke, different hypertensive retinopathy signs were associated with specific stroke subtypes.52 For example, retinal arteriolar narrowing was associated with lacunar stroke, while retinal hemorrhages were linked with cerebral hemorrhages. These findings suggest that hypertensive signs reflect specific cerebral microvasculopathy and may further help to understand the underlying pathologic mechanisms.47,52–54
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


