CHAPTER 8 History, Physical Examination, and the Preoperative Evaluation
Gathering a Patient History
Finally, a review of systems is part of every comprehensive history. This review includes changes in the patient’s respiratory, neurologic, cardiac, endocrine, psychiatric, gastrointestinal, urogenital, cutaneous skin, or musculoskeletal systems. The otolaryngologist often may derive more insight into the patient’s problem by inquiring about constitutional changes such as weight loss or gain, fatigue, heat or cold intolerance, rashes, and the like (Box 8-1).
Physical Examination
Facies
After assessing the patient’s overall appearance, the face should be analyzed for facial asymmetry by positioning the head squarely in front of the examiner. For instance, in patients considering facial plastic surgery, a hemifacial microsomia may affect the final outcome, which should be discussed before the operation. In addition, a paretic facial nerve always is a serious finding that can be detected by observing the tone of the underlying facial musculature and overlying facial skin. Facial wrinkles are more prominent when the facial nerve is functioning. For patients recovering from facial nerve paralysis, the American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) Facial Nerve Grading System is a respected standard for reporting gradations of nerve function (Table 8-1).
Table 8-1 AAO-HNS Facial Nerve Grading System
| Grade | Facial Movement | |
|---|---|---|
| I | Normal | Normal facial function at all times |
| II | Mild dysfunction | Forehead: moderate-to-good function |
| Eye: complete closure | ||
| Mouth: slight asymmetry | ||
| III | Moderate dysfunction | Forehead: slight-to-moderate movement |
| Eye: complete closure with effort | ||
| Mouth: slightly weak with maximum effort | ||
| IV | Moderately severe dysfunction | Forehead: none |
| Eye: incomplete closure | ||
| Mouth: asymmetrical with maximum effort | ||
| V | Severe dysfunction | Forehead: none |
| Eye: incomplete closure | ||
| Mouth: slight movement | ||
| VI | Total paralysis | No movement |
Neck
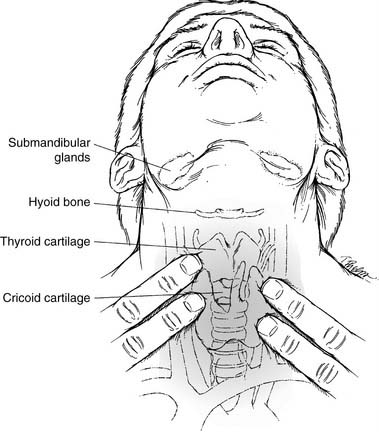
The neck, an integral part of the complete otolaryngology examination, is best approached by palpating it while visualizing the underlying structures (Fig. 8-1). The midline structures such as the trachea and larynx can be easily located and then palpated for deviation or crepitus. If there is a thyroid cartilage fracture, tenderness and crepitus may be present. In thick, short necks, the “signet ring” cricoid cartilage is a good landmark to use for orientation. The hyoid bone can be inspected and palpated by gently rocking it back and forth.
Triangles of the Neck
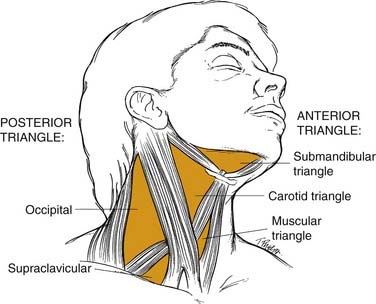
Most physicians find it helpful to define the neck in terms of triangles when communicating the location of physical findings (Fig. 8-2). The sternocleidomastoid muscle divides the neck into a posterior triangle—whose boundaries are the trapezius, clavicle, and sternocleidomastoid muscles—and an anterior triangle—bordered by the sternohyoid, digastric, and sternocleidomastoid muscles. These triangles are further divided into smaller triangles. The posterior triangle houses the supraclavicular and the occipital triangles. The anterior triangle then may be divided into the submandibular, carotid, and muscular triangles.
Lymph Node Regions
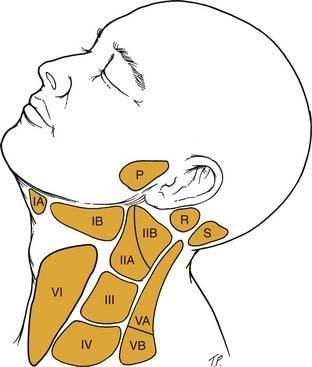
Another classification system for neck masses, endorsed by the American Head and Neck Society and the AAO-HNS, uses radiographic landmarks to define six levels to depict the location of adenopathy (Fig. 8-3). Level I is defined by the body of the mandible, anterior belly of the contralateral digastric muscle, and the stylohyoid muscle. Level IA contains the submental nodes, and level IB consists of the submandibular nodes. They are separated by the anterior belly of the digastric muscle.
Ears
Tympanic Membrane
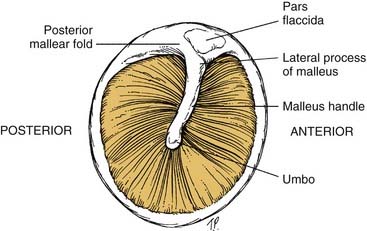
To assess the middle ear for effusions, use the tympanic membrane as a window that allows a view of the middle ear structures (Fig. 8-4). Effusions may be clear (serous), cloudy with infection present, or bloody. When the patient performs a Valsalva maneuver, actual bubbles may form in the effusion.
Hearing Assessment
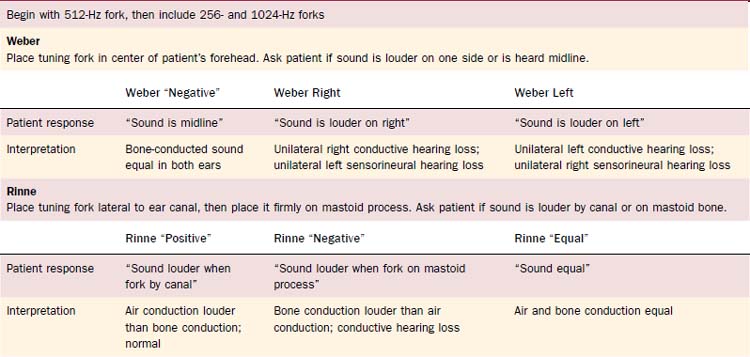
Tuning fork tests, usually done with a 512-Hz fork, allow the otolaryngologist to distinguish between sensorineural and conductive hearing loss (Table 8-2). They also may be used to confirm the audiogram, which may give spurious results because of poor-fitting earphones or variations in equipment or personnel. All tests should be conducted in a quiet room without background noise. Furthermore, one should ensure that the external auditory canal is not blocked with cerumen.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


