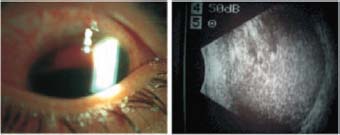
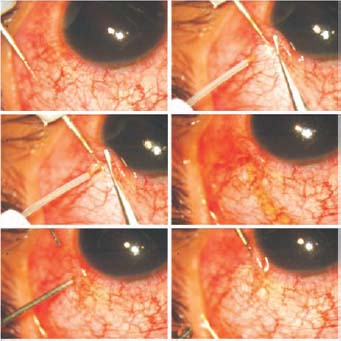
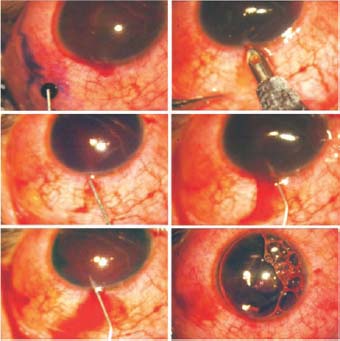
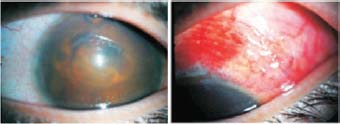
The patient in this case was an 11-year-old child who had already undergone extracapsular cataract extraction and iris claw lens implantation for a traumatic cataract 6 years previously. The patient presented 6 days after severe blunt trauma that resulted in hemophthalmos. The child was in severe pain and the intra-ocular pressure was very high. The lids were swollen. We did not expect light to penetrate through so much dark blood, but the patient did have very limited light perception. There was blood everywhere in the eye. A B-scan revealed that both the vitreous and the anterior chamber were full of blood. The anterior chamber showed a blackball hemorrhage over three quarters of the eye and dark red blood over the rest of the eye (Fig. 48.1). Ultrasound B-mode did not show a posterior chamber, as if this cavity too had been squeezed by the blood. To treat this patient successfully, the anterior chamber would have to be cleared and the intra-ocular pressure should be brought under control. My colleagues and I planned to evaluate the patient’s progress and refer her to a vitreoretinal surgeon if the vitreous did not clear up spontaneously within a reasonable period. Figure 48.1. Initial presentation of the eye shows a blackball hemorrhage in the anterior chamber. A B-scan shows that the vitreous is full of blood. From a surgical standpoint, mere paracentesis was impossible because the angle structures would be thoroughly clogged with blood. Starting the treatment from the vitreous side would have been a blind procedure unless an endoscopic device was available with vitrectomy. We reasoned that tapping into the posterior chamber would yield some results because aqueous fluid could not flow freely and was collecting in the posterior chamber. TECHNIQUE Anesthesia Perform the operation under general anesthesia. Surgical Technique In our case, the eye was observed to be highly congested. Touching on the cornea indicated that the intra-ocular pressure was very high. Figure 48.2. Blackball hemorrhage. The conjunctiva is slid toward the limbus and held down about 1 mm behind the surgical limbus. An activated 300-µm Fugo blade tip is passed along the blunt diamond conjunctival retractor that holds down the conjunctiva, through the conjunctiva, through the sclera and the ciliary body, and into the posterior chamber. Pigment and a minimal amount of blood flows out along with the aqueous. The posterior chamber is rinsed with saline to ensure that no blood remains in the cavity. Postoperative Management Twenty-four hours after surgery, the eye was quiet. The anterior chamber showed a medium-sized air bubble. Slightly dark red blood occupied three quarters of the anterior chamber and movement of the air bubble indicated that the blood was fluid (Fig. 48.4). Two days later the anterior chamber was cleared with repeated saline irrigation and aspiration. On the fourth day after surgery, the anterior chamber was clear and the iris claw lens was visible (Fig. 48.5). There was no congestion in the eye, and the patient had light projection in all directions. A well-formed bleb appeared to be formed from clear aqueous. Blood filled many lymphatic vessels running parallel to the limbus. Figure 48.3. Trypan blue dropped on the conjunctival open wound confirms continued fluid drainage. The anterior chamber is opened at the 12 o’clock position. The anterior chamber is repeatedly washed with urokinase 1:10,000. Finally, a large air bubble is placed in the anterior chamber. Figure 48.4. One day after surgery. Filtration is restored; some blood has entered the lymphatics. A large air bubble is present in the anterior chamber. Figure 48.5. Four days after surgery. The anterior chamber is almost clear. The conjunctiva apart from the surgical site shows no congestion. The bleb is well formed. At this point it is still too early to determine this patient’s prospects for vision recovery. But this case successfully proves that it is possible to drain the posterior chamber of a badly damaged eye that has high intra-ocular pressure. The prospect affords both patient and surgeon some breathing room and the confidence to plan subsequent treatment to restore sight. Suggested Reading Kellan R, Fugo RJ. Device increases safety, efficiency of cataract surgery. Ophthalmol Times. 2000;25:7–9. Roy FH. Course of Fugo blade is enlightening, surgeon says. Ocular Surg News. 2001;19:35–38.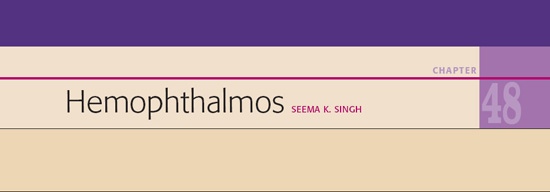
 hat follows is a description of the surgical management of a case of hemophthalmos using the Fugo blade in surgical procedures that were unimaginable only a few years ago.
hat follows is a description of the surgical management of a case of hemophthalmos using the Fugo blade in surgical procedures that were unimaginable only a few years ago.

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


