CHAPTER 162 Hearing Aids
Strategies of Amplification
The most common treatment for sensorineural hearing loss is the use of conventional hearing aid amplification. Despite substantial strides in the implementation of implantable technology, hearing aids remain the most widely used and appropriate treatment solution for most patients with hearing loss. Although hearing devices implanted worldwide during a year now number in the thousands, more than 2.4 million hearing aids were dispensed last year in the United States alone.1
Indications for Hearing Aid Use
Whether a patient is a candidate for a hearing aid is determined by three primary factors and several secondary considerations. Assuming that surgical or other medical management of the hearing loss has been exhausted, candidacy is based on the interaction of degree and configuration of hearing loss, the extent of the communication disorder resulting from the loss, motivation of the patient to address the communication disorder, and attitude toward hearing aid use.2 Generally, most patients who seek hearing aids can benefit from their use. Even in cases in which the prognosis for successful hearing aid use is guarded, an amplification solution is usually available if the patient is sufficiently motivated.
Hearing Loss Considerations
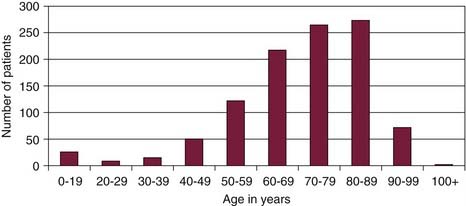
In an effort to provide a realistic view of the characteristics of hearing aid users, we evaluated data from 1860 ears of 1049 consecutive patients who were fitted with hearing aids at the Henry Ford Hospital during 2007. Patients ranged in age from 1 to 101 years old. The distribution of ages is shown in Figure 162-1. Of all patients, 81% were at least 60 years old, and 61% were 70 years or older. These percentages are typical of the hearing aid population in general. The prevalence of hearing loss is progressively greater with age, as is the use of hearing aids. Hearing aids are predominantly fitted on ears with sensorineural (88%) or mixed (11%) hearing loss. In this sample, less than 1% of hearing aid devices were fitted on ears with pure conductive hearing loss.
Auditory processing disorders in young children and in aging adults can also reduce the benefit from conventional hearing aid amplification. It is not unusual for geriatric patients who were previously successful hearing aid users to experience increasingly less success as their central auditory nervous systems change with age.3 The problem is seldom extreme enough to preclude hearing aid use, but these patients may benefit more from assistive technology to complement hearing aid use.4 Prognosis for hearing aid benefit in these patients is guarded.
Otologic and Other Factors
Physical and cognitive limitations may influence hearing aid candidacy. Physical limitations are primarily limitations pertaining to dexterity issues from arthritis and other conditions that affect a patient’s ability to manipulate certain styles of hearing aids.5,6 Limited cognitive ability can be a barrier to successful hearing aid use when a patient has difficulty remembering how to operate a hearing aid and its components.
Hearing Aid Technology
Evolution of Hearing Aid Technology
Hearing aid technology has advanced rapidly. Modern hearing aids use DSP for high-fidelity sound reproduction. They have adaptive directionality, feedback control, noise reduction, and low battery drain. They are readily programmable, providing substantial flexibility for precise fitting. Modern hearing aids also have advanced amplification strategies that reduce distortion and enhance listening comfort.7
Hearing aids have progressed since the late 1990s from analog to DSP. In analog hearing aids, acoustic signals followed an analog path that was under analog control, wherein an acoustic signal was converted by a microphone into electric energy in a continuously variable manner. In DSP hearing aids, acoustic signals are converted from analog to digital and back again, with digital control over various amplification parameters. DSP eliminated many of the barriers faced in trying to design analog circuits to fit in a small hearing aid and run on low-powered batteries. Along with flexibility inherent in enhanced programmability, modern devices provide more precise and flexible frequency shaping, more sophisticated compression algorithms, better acoustic feedback reduction, and enhanced noise reduction algorithms.8,9 The degree of sophistication of signal processing that is used in modern hearing aids seems limited only by the conceptual framework of how hearing aid amplification should work.
The most recent technologic advance in hearing aids is the growing opportunity of wireless connectivity, permitting communication from one hearing aid to another and from hearing aids to other electronic devices and signal sources.10
Hearing Instrument Components
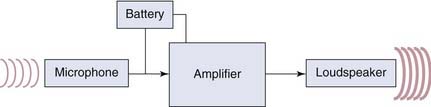
A hearing aid is an amplification device that consists of three basic components: a microphone, an amplifier, and a receiver. The power source for the amplifier is a battery. Most hearing aids also have some external controls, such as a program button or volume control on the hearing aid, or a remote control. A schematic of the basic components is shown in Figure 162-2.
Sound can also be delivered to the amplifier of a hearing aid via direct audio input, wherein a sound source reaches the hearing aid directly via a wire connector or “boot” that connects to a BTE hearing aid. One of the most common alternative input transducers is the telecoil, or t-coil. A telecoil allows the hearing aid to receive electromagnetic signals directly, bypassing the hearing aid microphone. The telecoil is often used with the telephone to reduce background noise, and to minimize the potential for feedback that occurs when placing a device near the microphone. A telecoil can be activated by a manual control on the hearing aid, by remote control, or automatically when the hearing aid senses an electromagnetic field.11
The telecoil can also be used to provide input for remote-microphone sources. The signal from the remote microphone is transmitted in some form to a loop of wire, which transmits the signal electromagnetically to the telecoil of the hearing aid.11 This type of technology is often used in a classroom situation, to allow the signal delivered from the remote-microphone worn by a teacher to be directly input to the hearing aid worn by the student.12 This technology minimizes the degradation of the auditory signal caused by background noise and distance.
A hearing aid may have some other form of wireless transducer, such as a frequency-modulated (FM) receiver or Bluetooth or other modern wireless connectivity. An FM receiver can be built into a hearing aid or attached as a boot on a BTE hearing aid. The FM receiver acts like an FM radio, receiving signals from a transmitter and directing them to the amplifier of the hearing aid.13 Increasingly, modern hearing aids are equipped with other wireless connectivity solutions, so that the hearing aid amplifier can receive signals directly from mobile phones, computers, or personal music players.10
Electroacoustic Characteristics
With linear amplification, the same amount of amplification, or gain, is applied to an input signal regardless of the intensity level of the signal so that low-intensity sounds are amplified to the same extent as high-intensity sounds. Figure 162-3 shows an example of a linear input-output function. In this example, for every dB increase in the input, there is a corresponding dB increase in the output. Fitting of linear hearing aids was a standard approach in the early years of hearing aids and remains applicable for conductive hearing loss and some mild sensorineural hearing losses. A problem with this type of amplification is that it does not address the nonlinearity of loudness growth that occurs with sensorineural hearing impairment. Many patients with sensorineural hearing loss do not hear low-intensity sounds, but can hear high-intensity sounds normally or even excessively loud owing to recruitment phenomena. Because a linear device amplifies soft and loud sounds identically, if a low-intensity sound is made loud enough to be audible, a high-intensity sound is likely to be too loud for the listener.14
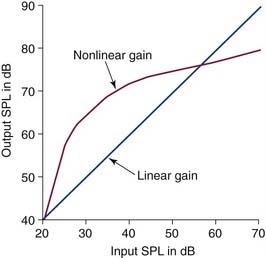
In nonlinear amplification, the relationship between input and output is not constant, so that low-intensity sounds are amplified to a greater extent than high-intensity sounds; this is shown schematically in Figure 162-3. The overall effect is to make low-intensity sounds audible; moderate sounds comfortable; and high-intensity sounds loud, but not too loud.
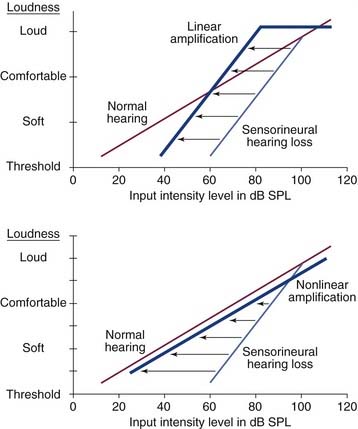
Nonlinear amplification is designed to address two problems with sensorineural hearing loss: reduced dynamic range, and loudness growth that is different from that of a normal ear. Dynamic range in this case is a term used to describe the decibel difference between the level of a person’s threshold of hearing sensitivity and the level that causes discomfort. In an individual with normal hearing, this range is 0 to about 100 dB hearing level (HL). In a patient with sensorineural hearing loss, the range is reduced. A patient with a 50-dB hearing loss and a discomfort level of 100 dB has a dynamic range of only 50 dB. Compression circuitry is used to boost the gain of low-intensity sounds so that they are audible, but to limit the gain of high-intensity sounds so that they are not uncomfortable. Figure 162-4 illustrates the difference between linear output and dynamic-range compression as it relates to an ear with sensorineural hearing loss and nonlinear loudness growth.
Nonlinear amplification is achieved with compression circuitry. Compression is a term that is used to describe how the amplification of a signal is changed as a function of its intensity. Compression techniques are used to limit the maximum output of a hearing aid and to provide nonlinear amplification across a wide range of inputs.14,15
Numerous nonlinear compression strategies have been developed to address the dynamic-range issue, and they vary in approach and complexity. Some strategies are designed to provide compression over a portion of the dynamic range. Partial dynamic-range compression typically provides linear amplification for low input signals and some level of compression when the input reaches a certain level. Other strategies are designed to provide compression over a wider portion of the dynamic range. Wide dynamic-range compression has as its basis the enhanced amplification of quiet sounds and reduced amplification of loud sounds, and is designed to package speech into a listener’s residual dynamic range. For most systems, dynamic-range compression can be altered in multiple frequency bands. In this way, if a patient’s dynamic range is reduced in one frequency range and nearly normal in another, the compression can be tailored to the frequency band where it is needed, and the other band can act as more of a linear amplifier.14–16
An amplifier also contains circuitry that limits its output. It is important that the output level of a hearing aid be limited to some maximum because high-intensity sounds can be damaging to the ear and uncomfortable to the listener. The classic method of limiting output, known as peak clipping, does not allow the peaks of signals to exceed a certain level. This method commonly causes distortion for high-intensity inputs. Compression limiting, the current standard method of output limiting, allows the amplifier to become nonlinear as input signals reach a predetermined level, so that the amount of gain is diminished significantly near the maximum output level.14,15
Other Hearing Aid Features
Today’s hearing aids include many features that make an important contribution to successful hearing aid fitting: directionality, noise reduction, feedback reduction, program management, automatic adaptivity, and data logging. During normal hearing, sound pressure waves reach the tympanic membrane after the acoustic signal has been modified by the resonance characteristics of the pinna, concha, and ear canal. These changes to the acoustic signal greatly aid the localization of a sound source in space, and contribute to the ability to hear in the presence of background noise.17 With hearing aid use, sound is received by the microphone, which is removed from the location of the tympanic membrane. The signal from the microphone does not include the spatial cues provided by the ear, reducing the ability to hear in background noise.
Most hearing aids can be changed from an omnidirectional to a directional setting. Typically, omnidirectional microphones are used in quiet environments.18 Directional microphones are beneficial in background noise so that the microphone sensitivity is focused in a desired direction. In some instruments, the directionality feature is activated manually by the patient. In other instruments, it can be activated automatically and adaptively when the hearing aid senses background noise, changing the amount of directionality based on the extent of the noise.19
Noise reduction circuitry is available in most modern hearing aids to reduce unwanted background noise in an effort to improve patient comfort and speech recognition. The sophistication of noise reduction strategies has advanced dramatically,20 and a thorough description is beyond the scope of this chapter. A simple example might serve to illustrate how the problem can be approached. The frequency and intensity of ongoing speech is highly variable and of short duration, whereas some background noise is relatively constant in nature. A DSP hearing aid can easily detect the difference in time constant and reduce the gain of the hearing aid in the frequency band of constant noise. Modern strategies use increasingly sophisticated algorithms to improve comfort and audibility in noise.
Acoustic feedback occurs when the amplified sound emanating from a receiver is directed back into the microphone of the same amplifying system. Physical separation of the microphone and receiver is the most effective way to reduce feedback. Another feedback reduction mechanism is feedback suppression circuitry. With feedback suppression, the hearing aid recognizes the occurrence of feedback based on frequency, intensity, and temporal characteristics. It reduces amplification in the offending frequency range to reduce feedback or uses phase cancellation of the feedback signal to eliminate audible feedback.21,22
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


