CHAPTER 206 Glottic and Subglottic Stenosis
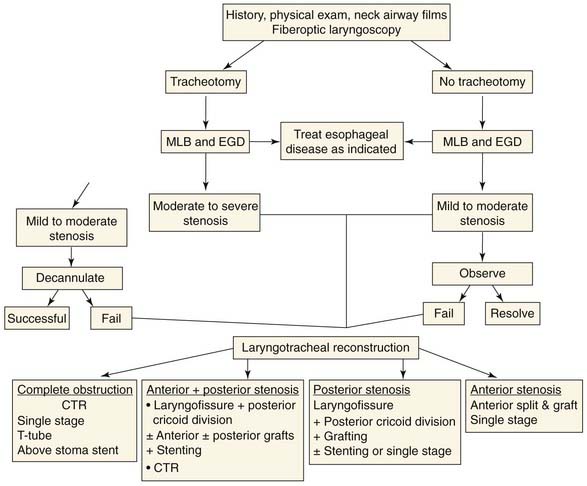
Chronic laryngeal stenosis is a partial or complete cicatricial narrowing of the endolarynx and may be congenital or acquired. The condition is rare and presents multiple problems affecting soft tissue and cartilage. Iatrogenic injuries and external neck trauma account for most cases. Chronic laryngeal stenosis in pediatric patients may be managed differently from that in adult patients, but the principles of expansion versus resection surgery remain the same. Of all laryngeal stenoses, chronic subglottic stenosis is the most common and presents significant challenges in management (Fig. 206-1).
Etiology and Pathophysiology
Congenital Laryngeal Stenosis
Congenital stenosis is secondary to inadequate recanalization of the laryngeal lumen after completion of normal epithelial fusion at the end of the third month of gestation.1 The final pathologic findings depend on the degree of recanalization. Thus if the laryngeal lumen is not recanalized and remains completely obliterated, it will result in complete laryngeal atresia; if it is partially recanalized, incomplete atresia, stenosis, or webbing will occur. The cricoid cartilage is usually abnormally developed.
Congenital Laryngeal Atresia and Web
Laryngeal atresia can occur at any laryngeal level or combination of levels. The clinical picture depends on the severity of the lesion. In complete atresia, the glottis is closed at or above the vocal cords by a firm fibrous membrane. The neonate is aphonic, tries vigorously to breathe, undergoes rapid deterioration, becomes cyanotic despite continued respiratory efforts, and soon dies of asphyxia unless immediate tracheotomy is performed.2,3 The condition is incompatible with life unless an emergency tracheotomy is performed or there is an associated tracheoesophageal or bronchoesophageal fistula. The most severe type of congenital laryngeal atresia presents as stillbirth and may not be recognized.
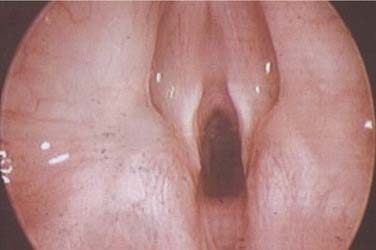
Congenital laryngeal webs account for about 5% of congenital anomalies of the larynx.4 About 75% occur at the glottic level, and the rest are supraglottic or subglottic.5 An association between anterior glottic web, the chromosome 22q11.2 deletion, and velocardiofacial syndrome has been established.6–8 All patients with anterior glottic web should have their chromosome 22q11.2 deletion status determined by standard fluorescent in situ hybridization (FISH) analysis. Most webs present at birth or in the first few months of life. The severity of the web varies. Only a few are severe enough to require airway support by intubation or tracheotomy. A laryngeal web is often an abnormality of the glottis and the subglottic cricoid region (Fig. 206-2). The differential diagnosis includes bilateral vocal cord paralysis and congenital interarytenoid joint fixation. It is important to detect associated anomalies of the larynx, the respiratory tract, and other organ systems.
Congenital Subglottic Stenosis
Congenital SGS is a clinical endoscopic diagnosis describing various histopathologic conditions that produce narrowing of the subglottic airway. Congenital SGS can be divided into membranous and cartilaginous types.9–11 The membranous type is a fibrous soft tissue thickening of the subglottic area caused by increased fibrous connective tissue or hyperplastic dilated mucous glands with no inflammatory reaction. It is usually circumferential, with the narrowest area 2 to 3 mm below the true vocal cords, sometimes extending upward to include the true vocal cords.12
The cartilaginous types are more variable, but the most common type is a thickening or deformity of the cricoid cartilage causing a shelf-like plate of cartilage, partially filling the concave inner surface of the cricoid ring and extending posteriorly as a solid rigid sheet, leaving only a small posterior opening.13
Symptoms depend on the degree of subglottic narrowing. In severe cases, respiratory distress and stridor are present at birth; in milder cases, the symptoms become evident during the first few weeks or months of life, presenting as prolonged or recurrent croup. Differential diagnosis includes subglottic hemangioma and subglottic cysts. Infants usually become symptomatic within 3 months of birth because of increased activity and increased ventilation requirements.2,9
Congenital subglottic stenosis is most often less severe than acquired stenosis and may therefore be managed more conservatively. Some patients outgrow the condition.12–14 Management depends on the degree and severity of stenosis, shape (whether the cricoid cartilage is normal or abnormal), and whether there are associated congenital anomalies.
Acquired Laryngeal Stenosis
Internal Laryngeal Trauma
Most cases of internal laryngeal injury are iatrogenic, secondary to prolonged endotracheal intubation, which is the most common cause of chronic laryngeal stenosis. Approximately 90% of cases of acquired chronic subglottic stenosis in infants and children occur secondary to endotracheal intubation.12,14 The reported incidence of stenosis after intubation ranges from less than 1% to 8.3%.15–19 This rate is much lower than the 12% to 20% reported in the late 1960s and early 1970s because of recognition of the problem and institution of preventive methods. Despite improvement in neonatal care, the incidence has stabilized at around 1% over the past 10 years.19,20 These figures may underestimate the true incidence of the disease in the pediatric population because many infants who are intubated do not survive the primary illness. In addition, some acquired subglottic stenosis may not be recognized unless an infection of the upper respiratory tract develops or the patient requires reintubation later in life. The areas most commonly injured are the subglottic region in children and the posterior endolarynx in adults.21
In children, the subglottic region is especially prone to injury from endotracheal tube intubation for various reasons. First, the cricoid cartilage is the only area in the upper airway that has a complete circular cartilaginous ring, preventing the outward extension of traumatic edema. Second, the pseudostratified, ciliated, columnar respiratory epithelium lining this region is delicate and tends to deteriorate under the stress of an indwelling tube. Third, the subglottic submucosa is made up of loose areolar tissue that allows edema to develop easily and quickly. Fourth, the subglottic region is the narrowest portion of the pediatric airway.12
The pathophysiology of acquired subglottic stenosis is well described in the literature.3,22–24 The endotracheal tube causes pressure necrosis at the point of interface with tissue, leading to mucosal edema and ulceration. As ulceration deepens, normal ciliary flow is interrupted, with mucociliary stasis leading to secondary infection and perichondritis. With further infection, chondritis and cartilaginous necrosis occur, especially with collapse of the airway during inspiration. Healing occurs by secondary intention with granulation tissue proliferation in the areas of ulceration and deposition of fibrous tissue in the submucosa. Primary healing of the laryngeal injury is hindered by the presence of loose and mobile subglottic mucosa, poor blood supply to the cartilage, and constant motion of the larynx associated with swallowing and head movement.23,25 Study of intubated larynges from infants of 22 to 40 weeks’ gestation who survived a few hours to 300 days showed acute injury was almost invariable and up to 100% of the subglottic epithelium was lost within a few hours of intubation, but progression of injury was relatively short lived. Ulcer healing started after a few days, rapidly progressed from day 10, and, in most cases, was complete after 30 days. This study suggests that longstanding acute injury of the subglottis is the exception rather than the rule, even with the endotracheal tube remaining in place.23
Duration of intubation and the size of the endotracheal tube are the most important factors in the development of laryngeal stenosis. No definite safe time limit for endotracheal intubation has been established. Severe injury has been reported after 17 hours of intubation in adults22 and 1 week after intubation in neonates.26 Several studies in adults have shown that a 7- to 10-day period is acceptable, after which prolongation of intubation is accompanied by an increased incidence of laryngotracheal complications.21 Premature infants tolerate more prolonged intubation (weeks rather than days). Explanations include relative immaturity of the laryngeal cartilage in the neonates (more hypercellular with scant gel-like matrix) rendering it more pliable, thus yielding to pressure,27 and the high location of the neonatal larynx in the neck with its posterior tilt and funnel shape.25
Other Causes of Laryngeal Stenosis
Laryngeal stenosis may occur secondary to laryngeal injury resulting from laryngeal surgery. Emergency cricothyroidotomy through the cricothyroid membrane28 and high tracheotomy can produce severe stenosis, particularly in children. Supraglottic stenosis and collapse may be related to prior laryngeal or tracheal injury. Acquired anterior glottic web can occur after excision of a laryngeal polyp or papilloma in the anterior commissure area if the anterior portions of both vocal cords are denuded simultaneously.29 Laryngeal stenosis also is described after endoscopic microsurgery with modalities such as electrocautery or laser.30
Chondroradionecrosis can lead to scarring and stenosis shortly after radiotherapy or as long as 20 years later.31 Intralaryngeal burns from fumes, smoke inhalation, or caustic lye ingestion can give rise to chronic laryngeal stenosis.32
Chronic Inflammatory Disease
Chronic inflammation secondary to gastroesophageal reflux (GER) may cause laryngeal stenosis. GER in children can be classified as physiologic, functional, pathologic, or secondary.33 Many airway manifestations have been attributed to GER including stridor, recurrent croup, exacerbation of subglottic stenosis, and chronic cough. Diagnosis is difficult unless the index of suspicion is high.34 The role of GER on the outcome of pediatric laryngotracheal reconstruction remains unknown.35 Until this is clear, the authors recommend that GER is investigated and treated in patients undergoing laryngeal reconstruction during the perioperative period.
Types of Stenosis
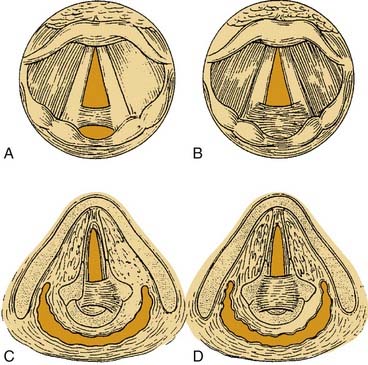
Pressure necrosis of the mucosa overlying the vocal process of the arytenoid occurs, followed by ulceration and granulation tissue formation on the medial surface of the body of the arytenoid cartilage. A similar process occurs to a variable degree in the interarytenoid area with involvement of the interarytenoid muscle, causing fibrous ankylosis of one or both cricoarytenoid joints.36 Posterior glottic scar frequently extends downward to the subglottic region. It is important to differentiate between a complete posterior glottic stenosis, in which the scar is located in the interarytenoid space and posterior commissure, and an interarytenoid adhesion, in which the scar is between the vocal processes of the arytenoids with a small posterior, mucosally lined sinus tract in the posterior commissure area (Figs. 206-3 and 206-4A). The scarring of the posterior commissure may be confined to the submucosa (see Fig. 206-4B) or extend into one (see Fig. 206-4C) or both (see Fig. 206-4D) cricoarytenoid joints.

The voice is generally good because of the adducted position of the vocal cords. The major symptoms are referable to the airway. In mild or moderate cases, the patient may be able to ventilate without a tracheotomy and may experience only exercise intolerance. Patients who have a more severe stenosis may need a tracheotomy for adequate respiratory exchange. Diagnosis by indirect laryngoscopy is difficult and may be confused with bilateral vocal cord paralysis.37 Diagnosis at direct laryngoscopy is made by careful observation of the posterior commissure. The true vocal cords are closely approximated because the vocal processes, and occasionally the arytenoid bodies, are tethered together by heavy scar. A posterior sinus tract should be carefully sought and is particularly difficult to see in the pediatric larynx. Unlike vocal cord paralysis, in posterior glottic stenosis the cricoarytenoid joints are partially or completely immobile on a passive motion test. Palpation of the arytenoids shows that they may be rocked in an anteroposterior direction but will not slide from side to side. Complete total glottic stenosis rarely occurs in isolation and is usually accompanied by supraglottic or subglottic stenosis. In children, it is a sequela of endotracheal intubation, lye ingestion, and thermal burn.
Prevention
Factors important in reducing the incidence of laryngotracheal stenosis include:
Diagnosis of Congenital and Acquired Laryngeal Stenosis
Laryngeal stenosis is diagnosed by a thorough history and physical examination, radiologic evaluation, and endoscopic examination of the airway and esophagus.38 Other investigations such as pulmonary function tests also may be helpful.
Endoscopic Examination
Indirect laryngoscopy alone is inadequate for diagnosis. Direct endoscopic visualization of the larynx is essential to study the stenosis carefully. Flexible fiberoptic endoscopy assesses the dynamics of vocal cord function and the upper airway, including the trachea.39 In patients with severe burns with neck contractures, flexible endoscopy may be the only method to visualize the larynx. Flexible retrograde tracheoscopy through the tracheotomy site may provide useful information in some cases.
Rigid and flexible endoscopy of the airway and esophagus should be performed in the operating room with the patient under general anesthesia. The rigid telescope is especially important in the examination of children because it better visualizes the small larynx. However, it is important to recognize that the airway lumen should be measured by passing bronchoscopes or endotracheal tubes of known sizes and cannot be gauged by the use of telescopes alone.40
Flexible endoscopy and spiral CT with mutiplanar resolutions have to be considered complementary techniques to rigid endoscopy in the preoperative evaluation and follow-up of children with laryngotracheal stenosis.41



