![]() 6
6 ![]()
Glaucoma Associated with Raised Episcleral Venous Pressure: The “Red Eye” Glaucomas
Kenneth W. Olander
Definition
How Is Glaucoma from Raised Episcleral Venous Pressure (EVP) Defined?
Increased EVP causing glaucoma may be seen in at least 17 clinical situations (Table 6–1). It is a type of secondary open-angle glaucoma and has four subtypes: (1) obstruction of venous drainage, (2) arteriovenous fistula, (3) ocular episcleral venous anomalies, and (4) idiopathic. This glaucoma is not rare and is commonly underdiagnosed, especially the idiopathic form and those caused by subclinical dural shunts.
| I. Venous obstruction |
1.Retrobulbar tumors |
2. Thyroid ophthalmopathy |
3. Superior vena cava syndrome |
4.Congestive heart failure |
5.Thrombosis of cavernous sinus or orbital vein |
6.Vasculitis of the episcleral and/or orbital vein |
7.Jugular venous obstruction |
8.Inversion therapy |
| II. Arteriovenous anomalies |
9. Carotid-cavernous sinus fistula |
10. Orbital varix |
11. Sturge-Weber syndrome |
12. Orbital meningeal shunts (dural shunt syndrome) |
13. Carotid jugular venous shunts |
14. Orbital vascular shunts |
| III. Idiopathic causes |
15. Sporadic |
16. Familial |
| IV. Medications |
17. Oral and topical |
Modified from Ritch, Shields, and Krupin, 1996. By permission from C.V. Mosby. |
Epidemiology and Importance
How Important and How Common Is Glaucoma from Raised EVP?
This is an important class of glaucoma because it may present at any time to anyone. The recognition of eyes with raised EVP is important for at least three reasons1:
- The episcleral veins serve as collector channels for the outflow of aqueous from the eye via Schlemm’s canal and the aqueous veins. Thus, a chronic elevation of pressure in the episcleral veins can result in the elevation of intraocular pressure (IOP) with resulting glaucoma and damage.
- The occurrence of glaucoma secondary to raised EVP dictates that an extensive medical, neurologic, and radiologic evaluation be performed, including arteriography and venography, to determine the cause of the raised EVP.
- Glaucoma secondary to raised EVP may not respond to some of the medical agents generally used in the treatment of other forms of open-angle glaucoma.
There is no single subspecialty that sees a lot of cases, as this type probably constitutes less than 1% of glaucomas. The patients typically have a red eye, but may not always notice it. Comprehensive ophthalmologists may be the first line of detection of this potentially fatal condition.2 It is almost impossible to define the exact frequency of this disease. As a glaucoma specialist, I had four cases over a 4-year period and then none for many subsequent years. Cornea specialists may see these cases of red eyes and may pick up the elevated IOPs. Neurophthalmologists may see some cases presenting with neurologic defects. Orbital specialists may see patients with pulsating exophthalmos.
A review of the literature indicates a wide range of presenting cases. Keltner et al3 saw 18 cases over 9 years, or two per year. Hieshima et al2 saw 131 cases over 12 years, or 11 per year. Regardless of how many cases are seen, treatment is often challenging and typical medical means do not work. Appropriately diagnosing and treating the underlying cause frequently cures this glaucoma, but often surgical intervention is required.
Diagnosis and Differential Diagnosis
What Is the Normal Drainage of Aqueous Out of the Eye?
It is necessary to review some basic scientific principles regarding the drainage of aqueous out of the eye and how the vascular plexus and venous pressure cause glaucoma. According to Weinreb and Karwatowski,4 it was Sidel in 1923 who was the first to inject ink into the anterior chamber and observe its appearance in the episcleral veins. They also point out that it was not until 1942 that Ascher observed clear aqueous humor laminated with blood in a vessel demonstrating an anatomic connection between Schlemm’s canal and the episcleral veins. Recent scanning electron microscopy of vascular resin casts has added significantly to our detailed understanding of this anatomy.5 It should be noted that this is a valveless system with frequent interconnections. Indeed, blood can be diverted from one system to the other, with flow in any direction, depending on the hydrostatic pressure gradient.
There is a constant flow of aqueous humor through the anterior segment of the eye. We know that the aqueous is formed by the ciliary processes, passes through the pupil, and exits in the angle. Most of the fluid enters the venous system by way of the trabecular meshwork and Schlemm’s canal; this is called convention outflow. A smaller amount of aqueous passes through the ciliary muscle and the iris to reach the superciliary and superchoroidal spaces. From there, the fluid passes through the sclera or through the loose connective tissue around the penetrating nerves and vessels. This is called unconventional outflow.
What Is Conventional Outflow?
The episcleral tissue is a loose connective and elastic tissue covering the sclera and connecting to the conjunctiva. It is continuous with the loose tissue of Tenon’s space and tightly connects to denser sclera in its deeper layers. It contains multiple blood vessels. Behind the ocular attachments of the recti, the episcleral tissue is thin and the vessels, two veins to each artery, form a wide meshed net. The arteries here come from the posterior ciliary network. In front of the attachment of the muscles, the episclera is much thicker and much richer in vessels. The meshes of the vascular net are smaller. A capillary net exists only in this anterior zone on the sclera. When there is a marked filling of this net, it is called ciliary injection. Aqueous humor drains through the trabecular meshwork into Schlemm’s canal. Arising from the outer circumference of the canal are the external collector channels that drain into the episcleral and conjunctival venous plexus. There are 25 to 35 collector channels. When one of the connects directly with a surface vein, it can be seen on slit-lamp examination and is termed an “aqueous vein.” Some 14 or more branches from the ciliary muscle also traverse the sclera to join the plexus of veins adjacent to the canal. Aqueous veins of Ascher vary in size from 0.01 to 0.1 mm in diameter. They are found near the limbus and most often inferonasally commencing in a hook-shaped bend where they come out of the sclera. They contain a clear fluid, and a laminated flow of blood and clear fluid can often be seen.6 Thus, to summarize, the aqueous drains from Schlemm’s canal into a deep scleral plexus of veins, and then via the intrascleral plexus to the episcleral plexus and the subconjunctival plexus at the limbus. In addition, from direct connections, aqueous veins pass from the deep sclera to the episcleral plexus. Under conditions of increased episcleral venous pressure, the flow will be reversed and blood is frequently seen in Schlemm’s canal with simple gonioscopy.7
What Affects the Aqueous Humor Dynamics?
In the steady state, the dependence of IOP on EVP is approximated by the modified Goldmann equation Po =f/c + Pev, where Po is the IOP, Pev is the EVP, ƒ is the aqueous inflow, and c is the outflow facility. This equation states that for every 1 mm increase in EVP, there is a concomitant increase of 1 mm in IOP. Numerous studies have been done to test this hypothesis. In 1968, the validity of the Goldmann equation was first tested in humans.8 It was observed that for every millimeter of mercury increase in EVP, there was only a 0.75-mm increase in ocular pressure. The term pseudofacility is used to describe the decrease in inflow, secondary to an increase in IOP, and is frequently a part of a trick question given to ophthalmology residents, as follows: “What is the tonographic outflow facility in a patient with elevated IOP due to increased EVP?” There is a natural tendency to answer that the outflow facility is abnormal because, obviously, the IOP is elevated. This would be incorrect. The tonographic outflow facility, at least in the disease process, can be and usually is normal despite the elevated IOP. This phenomenon has been studied in normal volunteers using a blood pressure cuff placed around the patient’s neck. When it is inflated, the episcleral venous pressure becomes elevated, but the IOP increases to a slightly smaller degree. This effect is small and the overall phenomenon indicates that the aqueous humor formation does not self-regulate in response to the level of IOP.9 There are no known feedback loops or anatomic connections that would allow such a regulatory process to occur. It is tempting to speculate that a chronically elevated EVP could be an important factor in all chronic open-angle glaucoma, but this has not been demonstrated to be the case.10 However, for secondary types of open-angle glaucoma, episcleral venous pressure is important (Table 6–2).
| Slit-lamp exam for “red eye”; blood in aqueous veins |
| Gonioscopy showing blood in Schlemm’s canal |
| Dilated fundus exam showing distension of retinal veins |
| Extraocular motility exam showing duction deficiencies |
| Arteriovenous fistula (AVF) screening tests showing neurologic cuts |
| Orbital exam showing bruit, vascular anomalies, or traumatic scars |
| Tonography sometimes helpful |
| Presence of exophthalmos—stable or pulsatile |
| Increased cup-to-disc ratio showing chronically increased IOP |
| EVP measurement directly elevated |
| Ophthalmodynamometry showing arteriovenous malformations |
| Orbital ultrasound showing soft tissue masses—may increase with position changes |
What Is Uveoscleral or Unconventional Outflow?
Bill11 was among the first to point out that flow through the trabecular meshwork and Schlemm’s canal seems to involve a well-designed fluid transport system. In contrast, uveoscleral flow seems more primitive and resembles a leak more than a well-designed fluid transport system.7 The aqueous humor enters the ciliary muscle fibrils through the uveotrabecular meshwork, the ciliary body space, and the root of the iris. Fluid passes between the bundles of the muscle until it reaches the supraciliary and suprachoroidal spaces. The aqueous humor leaves the eye through the spaces around the penetrating nerves and blood vessels and through the sclera. Even large molecules, such as horseradish peroxidase, can pass through intact sclera. Uveoscleral flow seems to be present in most species, but the amount of aqueous humor transported by the system varies considerably, being approximately 3% in rabbits and 50% in some species of monkey; in humans it is estimated that 5 to 25% of the total outflow is through this unconventional pathway. Direct measurement of uveoscleral flow is very limited, and the human eyes that have been studied may be atypical. Also, outflow increases up to fourfold when the anterior segment is inflamed. It appears that uveoscleral flow increases when the IOP is raised from atmospheric pressure to the level of the EVP; however, above this pressure level, uveoscleral flow is largely independent of IOP. The main resistance to uveoscleral flow is the tone of the ciliary muscles. Factors that contract the ciliary muscles, such as pilocarpine, lower the flow, whereas drugs that relax the ciliary muscles, such as atropine, increase the flow. The prostaglandins significantly increase uveoscleral outflow, and the effects of a prostaglandin/pilocarpine combination are largely unstudied. A few studies indicate that epinephrine may lower IOP by increasing uveoscleral outflow. Cyclodialysis is an older operation designed to lower IOP by detaching a portion of the ciliary body from the scleral spur. There is evidence that this acts to increase uveoscleral outflow.7
What Is the Normal Venous Drainage of the Orbit?
The main venous supply from the orbit is provided by the superior ophthalmic vein, the inferior ophthalmic vein, and the central retinal vein (Fig. 6–1).12 The supply to the eyelids is supplemented by branches of the superficial temporal and facial veins. These vessels have no valves, are markedly tortuous, and display many plexiform anastomoses. They communicate with the veins of the face, with the pterygoid plexus, and with the veins of the nose. They ultimately drain into the cavernous sinus.
The superior ophthalmic vein is formed near the root of the nose via communication from the angular vein and the supraorbital vein. It passes into the orbit above the medial palpebral ligament and then accompanies the ophthalmic artery across the optic nerve and under the superior rectus to the superior orbital fissure, where it is usually joined by the inferior ophthalmic vein. It then leaves the orbit to enter the cavernous sinus. The inferior ophthalmic vein forms as a venous plexus on the orbital floor. It takes branches from the lower lid, tear sac, inferior rectus, oblique muscles, and the two inferior vortex veins. The blood flow passes posteriorly, forming two veins, getting into the medial compartment of the supraorbital fissure, and then into the cavernous sinus. A lower branch may pass through the intraorbital fissure to the pterygoid plexus.
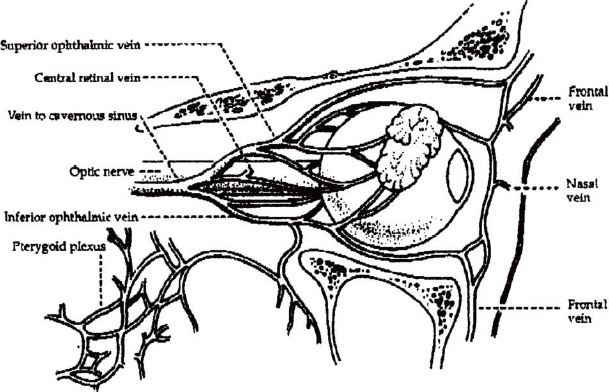
Figure 6–1. Venous drainage of the orbit. Superior ophthalmic vein, inferior ophthalmic vein and facial veins are the three principal routes of orbital venous drainage. (From Ritch, Shields, and Krupin, 1999. By permission from C.V. Mosby.)
The central retinal vein is a confluence of all of the branches of the retinal venous circulation. The upper veins form a superior papillary vein and the lower and inferior papillary vein, which unite in the region of the optic cup. About 10 mm behind the globe, the central retinal vein turns downward at a right angle to leave the optic nerve. It usually passes through the sheath of the optic nerve and emerges behind the artery, where it runs posteriorly and passes through the oculomotor foramen to enter the cavernous sinus directly. The cavernous sinus drains primarily through the superoinferior petrosal sinuses into the internal jugular vein. A small amount drains through the external jugular veins, and still less through the suboccipital plexus into the vertebral and deep cervical veins. The cavernous sinus also has connections with the ipsilateral pterygoid plexus and the contralateral cavernous sinus. Facial veins communicate with the superior ophthalmic vein through the nasal, frontal, and lacrimal eyelid veins and communicate with the inferior ophthalmic vein through the infraorbital vein. The facial veins drain mainly into the external jugular veins.4,6
How Is the EVP Measured?
The episcleral vessels can easily be differentiated from the conjunctival vessels by the relative mobility of the latter when they are in touch with the tip of a pressure chamber (Table 6–3). The episcleral veins are differentiated from the anterior ciliary arteries by the narrower caliber, straighter course, and slightly darker color of the veins. Glaucomatous damage develops in certain patients because of elevated EVP. For an instrument to be practical in the clinical environment, it should be easily operated by one observer, require little calibration, be of compact size, permit stereopsis before and during the measurement, and provide good reproducibility. Such an instrument, called a venomanometer, has been developed by Zeimer and associates.13 Basically, the instrument is mounted directly on the slit lamp. It looks similar to an applanation tonometer. There is a flexible transparent tip of molded silicone rubber covering an air-sealed piston. There is a rotating dial that controls the position of the air-sealed piston. The position of the piston determines the volume of air in the chamber and therefore its pressure. The instrument is available currently for approximately $850 according to personal communications with Peter Netland, M.D., Ph.D.
Blood test for thyroid disease |
Look for exophthalmos—stable or pulsatile |
Listen for bruit in orbit or neck |
Do x-ray/computed tomography (CT) scan of skull, orbit, foramen |
Do electroencephalogram (EEG) |
Examine carefully for skin lesions suggestive of congenital vascular disease or scars indicating trauma |
Performing systemic measurement of venous pressure in arms |
Get a complete neurologic examination |
Order selective external and internal carotid arteriogram |
Order orbital venogram |
Consider digital subtraction angiogram or color Doppler ultrasound |
The EVPs in normal eyes and in eyes with open-angle glaucoma have not been shown to be significantly different. However, Kupfer10 and Talusan and Schwartz14 have reported that ocular hypertensive eyes have a slightly lower EVP than normal eyes. There are some problems in measuring the EVP. Most of these problems are of an anatomic nature. Different observers may select different blood vessels, which may yield slightly different readings. Also, the selection of the end-point indication of increased EVP is somewhat arbitrary. Tissue compressibility has been reported to be negligible, and the pressure required to blanch the vessel to the one-half point accurately reflects the intraluminal pressure. No evidence has been found for regional differences in EVP within the quadrant of an eye or between the two eyes. There is a significant correlation of EVP with age. The normal EVP runs 7.6 ± 1.3 mm Hg. When the EVP is raised by some disease process, the IOP is usually increased as well; however, the relationship between the pressure increases is more complex in the chronic situation than in the acute, experimental situation. Many conditions, for example carotid cavernous fistula, that increase EVP also cause ocular ischemia, and that reduces the aqueous humor formation and IOP. Also, acute elevations of EVP increase the facility of outflow, whereas chronic elevations of pressure may produce secondary changes in the angle structures, and ultimately decrease the outflow facility.
What Clinical Conditions Cause Raised EVP?
Various clinical conditions may result in elevated EVP. As discussed below, patients may present with a multitude of ocular and/or systemic signs and symptoms. The steps in an evaluation include a history; measurement of visual acuity, IOP, and EVP; slit-lamp examination; neurophthalmic examination, gonioscopy; and fundus examination. Figure 6–2 delineates various steps that may help in the diagnosis.
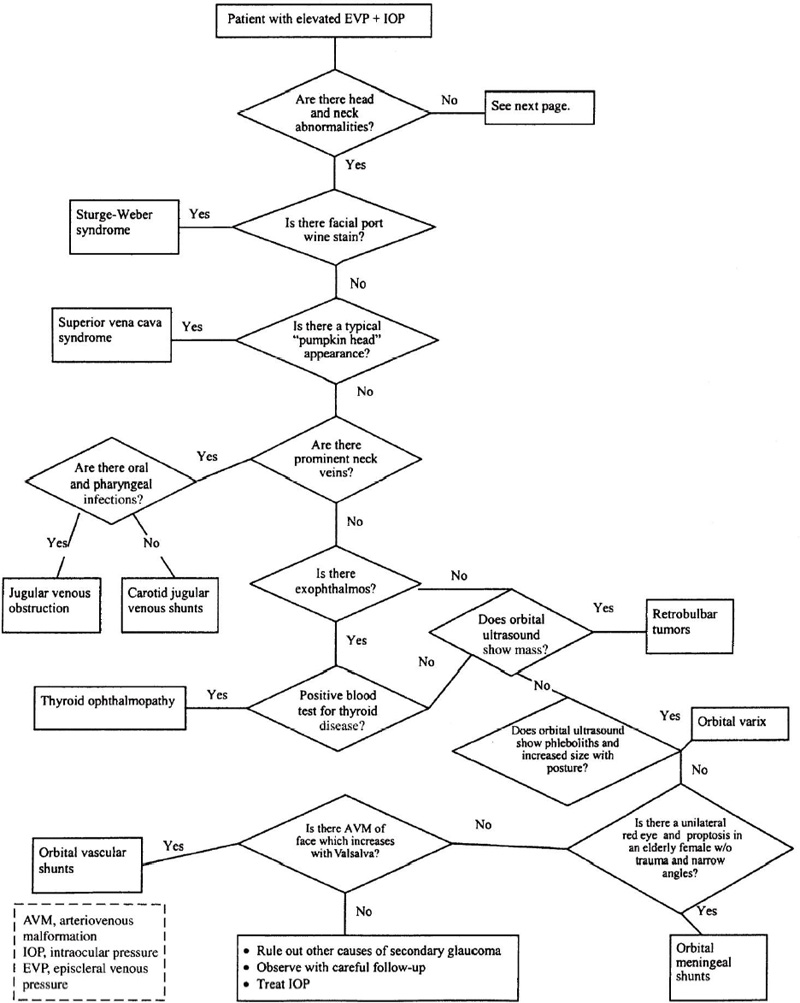
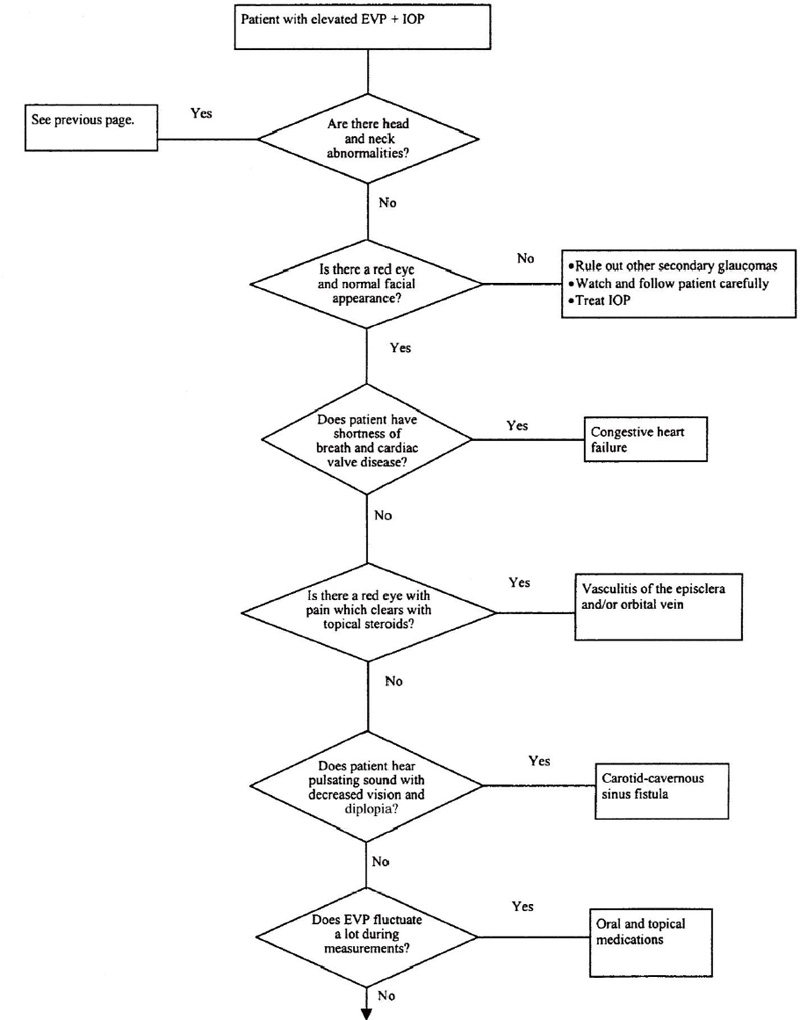
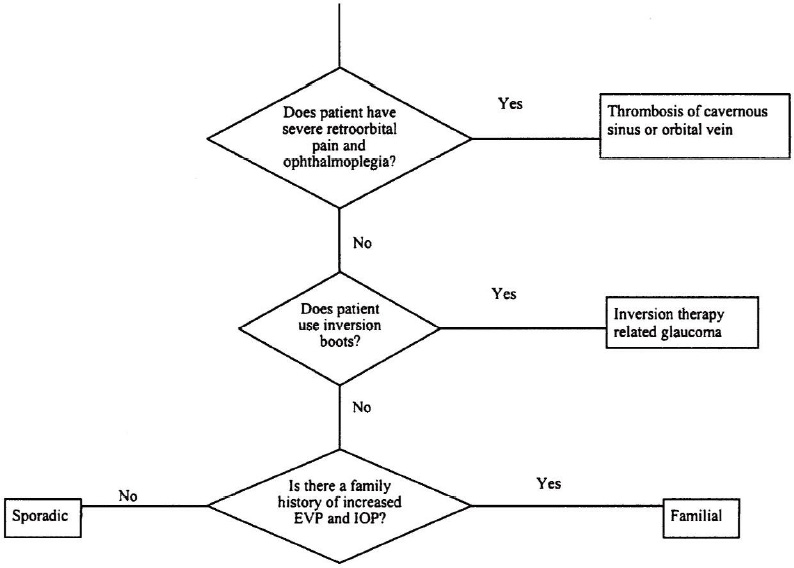
Figure 6–2. Algorithm for diagnosing causes of increased EVP.
What Venous Obstruction Problems Cause Raised EVP?
Orbital venous abnormalities and lymphangiomas have been generally classified on morphologic grounds; however, this has led to a confusing scientific dialogue. The members of the Orbital Society have recently issued a statement classifying orbital vascular malformations based on their hemodynamic relationships (Table 6–4). Orbital vascular malformations fall into three categories: no flow, venous flow, and arterial flow. Assignment to each group is based on pertinent clinical and imaging criteria. Mixed forms with both no flow and venous components are grouped with the venous flow category.15
Do Retrobulbar Tumors Cause Glaucoma?
Any orbital tumor that compresses the venous system may result in glaucoma secondary to backup in venous system drainage apparatus. Nordman et al reported 14 cases caused by a variety of tumors in 1961 (translation cited by Weinreb and Karwatowski4). This condition would generally be diagnosed with a computed tomography (CT) scan or an ultrasound. Intraocular tumors, such as ciliary body melanomas, may present with engorgement of the episcleral veins, which are called the “sentinel vessels.” However, these engorged vessels are localized over the tumor site and are restricted to a single quadrant, and glaucoma is not commonly seen.
Does Thyroid Ophthalmopathy Cause Glaucoma?
Thyroid eye disease is known by a variety of names, and the hormonal defect of this condition is unclear. Patients can be hypothyroid, euthyroid, or hyperthyroid when the problems begin. The physical findings are variable, and include exophthalmos, chemosis, and dilated conjunctival and episcleral vessels. Histopathologically, there is infiltration of the orbit including rectus muscles with lymphocytes, mast cells, and plasma cells. IOP can be increased for several reasons, including elevated EVP. Elevated EVP may result from the retrobulbar infiltration process.16 Jorgenson and Guthoff16 reported that 5 of 35 patients with endocrine orbitopathy had increased IOP in primary gaze. EVP was high, being between 16 and 23 mm Hg. It was speculated that compression of the ophthalmic veins by swollen extraocular muscles resulted in abnormal EVP and subsequently raised IOP. Also, the contraction of extraocular muscles resulted in the abnormal EVP and subsequently raised IOP. Also, the contraction of extraocular muscles may cause abnormally high IOPs in some specific directions of gaze. Usually fibrosis of the inferior rectus muscle significantly increases IOP in upgaze.4 The presence of exophthalmos with abnormal blood tests and either orbital ultrasound or CT scan of the orbit showing enlarged extraocular muscles will aid in the diagnosis of this condition.
| No flow malformations |
Hemodynamically isolated |
Applicable to so-called lymphangiomas |
| Venous flow malformations |
Applicable to so-called primary varices |
Including distensible and nondistensible varieties |
Including mixed forms with venous and no flow components (grouped here to |
emphasize the clinical importance of the venous relationship) |
| Arterial flow malformations |
Arteriovenous malformations or arterialized veins distal to them |
Applicable to so-called secondary varices |
From Harris GJ: Orbital vascular malformations: a consensus statement on terminology and its clinical implications. Am J Ophthalmol 1999;127:453–455. By permission from Elsevier Science. |
Does Superior Vena Cava Syndrome (SVCS) Cause Glaucoma?
Obstruction of the superior vena cava will result in increased venous pressure in those areas in which it provides venous drainage. These patients show edema and cyanosis of the face and neck as well as dilated vessels in the head, neck, chest, and upper extremities. Obstruction may increase the intracranial pressure, causing headaches, stupor, vertigo, seizures, and mental changes. Ocular findings include exophthalmos, papilledema, and prominent blood vessels in the conjunctiva, episclera, and retina.17 The IOP is usually elevated and is greater when the patient is in the supine position. It has been reported that glaucomatous cupping occurs infrequently with this syndrome, despite the elevated IOP. Some researchers propose that cupping does not occur because the IOP is counterbalanced by elevated intracranial pressure.17 Before the advent of antibiotics, this syndrome was commonly caused by mediastenitis secondary to the pulmonary infections of syphilis or tuberculosis. Presently, malignancy is the cause of 97% of these cases. Occasionally, aortic aneurysm, enlarged hilar nodes, and intrathoracic thyroid disease may be involved. Diagnosis is suggested by the clinical appearance of the face and neck, “pumpkin head” appearance, and by altered neurologic status accompanied by frequent complaints of headaches. The glaucoma is bilateral and usually gives rise to no subjective complaints. The site of obstruction may be demonstrated by venography or scintigraphy, but not without attendant hazards. These tests are generally not warranted. SVCS is usually more frequent on the right side, with a ratio of 4:1, and at present the most common cause is bronchogenic carcinoma.18
Does Congestive Heart Failure Lead to Glaucoma?
A report in the German-language literature by Bettelheim19 has demonstrated that elevated EVP in pulmonary hypertension can cause glaucoma and it was termed “cardiogenesis glaucoma.” No details are available, as the original article has not been translated into English. Nevertheless, this type of glaucoma points out that many case reports in the literature present intriguing diagnostic questions that remain unanswered. Another cardiac abnormality causing bilateral corkscrew episcleral veins occurred in a 56-year-old woman with an insidious onset of redness in both eyes, developing over a course of 6 months.20 She had a history of rheumatic heart disease and had marked tricuspid valve incompetence. She did not have elevation of her IOP. The important concept in this article concerns the use of orbital color Doppler ultrasound to detect this unusual episodic biphasic blood flow present in both superior ophthalmic veins. Similar Doppler flow patterns were demonstrated on both of this patient’s internal jugular veins. Even though the patient was not in congestive heart failure at the time of her exam, it appears that the congestive effect in this patient was caused by tricuspid incompetence transmitting the ventricular pressure as reversed flow in the superior ophthalmic veins. Nevertheless, it was not a constant arterialized reversal of flow seen in a typical carotid cavernous sinus fistula. The noninvasive nature of color Doppler imaging and its ability to perform in an outpatient clinic makes it a choice over standard angiography in many situations.
Does Thrombosis of the Cavernous Sinus or Superior Ophthalmic Vein Cause Glaucoma?
Occlusion or thrombosis of the superior ophthalmic vein or the cavernous sinus is a nonspecific finding that may be caused by such disorders as tumors of the skull base or nasopharynx. Sometimes no cause can be found. Brismar and Brismar21 described eight cases with increased EVP and glaucoma. Typically, these patients will have third, fourth, and sixth cranial nerve palsies. Retroorbital pain associated with ophthalmoplegia is typical, and more serious underlying causes need to be ruled out. Septic cavernous sinus thrombosis is not difficult to distinguish because of its fulminant nature. Many of these cases show spontaneous remission. Improvement with steroid therapy does not help in establishing the etiologic cause. Extensive clinical and radiologic evaluation should be done on these patients to discern a more serious underlying disorder. These tests would include carotid angiography, tomography of the skull base, and nasopharyngoscopy with blind biopsies. Orbital phlebography has a definite value in the diagnosis of these patients. Infrequently, it is quite a challenge to distinguish between Talosa-Hunt syndrome and aseptic cavernous sinus thrombosis. Although the IOP was normal in these eight cases, many of them had abnormalities of the optic nerve and visual field defects that had not been clearly described. Conjunctival venous dilations and retinal venous dilations were present in a number of these cases.
Does Vasculitis of the Episcleral and/or Orbital Veins Cause Glaucoma?
Patients with anterior scleritis may have elevated IOP related to raised EVP. In a German-language article by Jorgensen and Guthoff,16 64 patients were described with dilated vessels and glaucoma. Raised EVP was the cause of the elevated IOP. Jorgensen and Guthoff described cases of spontaneous carotid cavernous fistula, Sturge-Weber syndrome, orbital tumors, endocrine ophthalmopathy, anterior scleritis, and idiopathic cases. A variety of pathophysiologic mechanisms were involved. After systemic steroid therapy, both raised IOP and elevated EVP returned to normal.
Can Jugular Venous Obstruction Cause Glaucoma?
In 1946, Meyer22 described a type of secondary glaucoma due to inflammatory jugular phlebostenosis and called it “glaucoma exogenicum.” He traced clinically the cause of glaucoma to jugular phlebostenosis caused by proliferative endophlebitis. He claimed that the bulk of blood entering the head is drained off by the internal jugular veins on either side of the neck. A relatively small amount of venous blood passes through the external jugular veins, and another very small portion returns by way of the suboccipital plexus into vertebral and deep cervical veins and from there into the anominate veins. In Meyer’s era the primary cause of the jugular endophlebitis could be traced to oral infections, such as acute tonsillitis, and other pharyngeal infections. Meyer found that the application of leeches in the treatment of purulent phlebitis in the lower extremities was beneficial, and he stated that previously ophthalmologists had used leeches in glaucoma cases. They applied leeches over the temporal region in glaucoma patients and this application resulted in a temporary decongestion of the eye. He claimed that “recalibration” of the jugular veins with leeches in inflammatory obstruction brings on a total decongestion of the whole head area and therefore has a permanent therapeutic effect.
Does Inversion Therapy Lead to Glaucoma?
The IOP typically increases as the body assumes a more dependent posture. When the body is totally inverted in a vertical orientation, the IOP rapidly rises to a level approximately double the normal erect posture. Eleven patients had their EVP and gonioscopy performed in the supine and inverted positions.23 The IOP rose rapidly; within 10 seconds 70% of the increase had occurred and within 1 minute a constant value was reached. It was felt that the rapid rise in pressure was due to mechanical compression of the orbital contents against the globe, and that congestion and expansion of the uveal tissue from increased venous and arterial pressure within the orbit also played an important role. The investigators felt that the sustained increase in venous pressure in the orbit and additional contributions to the IOP may be due to a net increase in the rate of aqueous production. Alterations in the rate of uveoscleral outflow may also be a factor. They found that for every 0.83 mm Hg increase in EVP, there was a 1 mm Hg increase in IOP.
What Arteriovenous Anomalies May Lead to Glaucoma?
Various arteriovenous anomalies that may cause glaucoma are described below.
Does Carotid-Cavernous Sinus Fistula (CCSF) Cause Glaucoma?
CCSF can be subdivided into (1) etiologic (i.e., spontaneous or traumatic), (2) hemodynamic, (i.e., high or low flow), and (3) anatomic (i.e., direct or dural). CCSFs provide a free communication between the internal carotid artery and the surrounding cavernous sinus resulting in high blood flow and high mean pressure in the shunt.3 A reversal of the blood flow in these vessels leads to congestion of the orbital veins and soft tissue. Shunting of the blood may produce ocular ischemia, and there may be a pulsatile exophthalmos. Patients with CCSF often (75%) give a history of previous trauma. Many of these patients have a dramatic appearance with pulsatile exophthalmos, chemosis, lid edema, vascular engorgement, and restriction of ocular motility. The conjunctival episcleral veins have a tortuous corkscrew appearance. These findings usually occur on the same side as the fistula, but because of connections between the cavernous sinuses, the findings may be bilateral or alternating.7 Occasionally, the clinical findings may mimic thyroid disease. Typically, the patient is a young man who presents soon after a severe head injury with the above findings. In cases of nontraumatic etiology, the patients are typically postmenopausal women. They generally have no bruit, their proptosis is minimal, and their eyes do not pulsate. Most commonly, patients present because of chronic red eye. The increased IOP in nearly every patient can be severe and may cause blindness.24 These patients often complain of a noise in their ears, and a bruit is often present over the frontal or temporal regions or on the globe. The IOP is elevated because of the increased EVP, although angle closure and neovascular glaucoma have been reported.25,26 Skull films, orbital ultrasonography, or CT or magnetic resonance imaging (MRI) scans confirm the diagnosis along with the initial clinical impression, but arteriography provides the most detailed information about these fistulas. Treatment can be difficult and is usually reserved for individuals who have severe pain, incapacitating bruit, progressive glaucomatous vision loss, or other serious complications.27 A variety of embolization and balloon catheter techniques have been developed with increasing success, but there is still a fairly high morbidity and mortality.
Does Orbital Varix Cause Glaucoma?
Orbital varices are typically found in young persons who have a history of intermittent unilateral proptosis beginning in early childhood. The proptosis may be worsened by increasing the venous pressure in the head and neck such as found in the Valsalva maneuver or bending over. Patients present with dilated veins in the eyelid, anterior orbit, sometimes acute orbital hemorrhage, or thrombophlebitis. Approximately 50% of these patients will have other systemic venous abnormalities involving the scalp, palate, and forehead, and rarely it may be associated with Klippel-Trenaunay-Weber syndrome. The conjunctiva may show multiloculated cysts, which may be misdiagnosed as orbital lymphangioma. Orbital venography will show venous angioma composed of a network of large, dilated, and tortuous veins overlying the frontal bone draining into a dilated angular vein. In a typical patient, as reported by Rathburn et al28 in 1970, the dye flowed into a single inferior ophthalmic varix and then into the cavernous sinus. The superior ophthalmic vein was not involved. There was no evidence of intercranial venous abnormality in the cavernous sinus. Their patient required surgery because of intermittent exophthalmos and an incapacitating headache. Following surgical removal of the varix, the headaches disappeared, as did the cosmetic deformity. The diagnosis of orbital varix can be further delineated using orbital radiography, which may show orbital phleboliths and an enlarged orbit. Ultrasonography and CT scan show a soft tissue mass, and ultrasonography will show the mass to enlarge during the Valsalva maneuver. Glaucoma is uncommon in this condition because of the transient nature of the malformation, and generally the glaucoma, when present, does not respond to medical therapy.4
Is Glaucoma Apparent in Sturge-Weber Syndrome?
Sturge-Weber syndrome, also known as encephalofacial angiomatosis or encephalotrigeminal angiomatosis, is seen with a flat facial hemangioma that follows the distribution of the fifth cranial nerve. A meningohemangioma, which may produce a seizure disorder in the child, may also be present. The meningohemangioma may be associated with calcification easily revealed by skull x-rays occurring as early as age 1 year. The association of facial hemangiomatous nevi with neurologic impairment was first clinically delineated by Sturge in 1879 in a young girl, as cited in Bodensteiner and Roach.29 In 1922, Weber wrote the first report of the radiologic features of the syndrome. In this condition, the classic manifestations include the facial port-wine stain, a contralateral hemiparesis, hemiatrophy of the brain, and mental retardation with a homonymous hemianopsia. Other features include glaucoma, dental abnormalities, and skeletal lesions. There is no clear genetic pattern, and two affected individuals almost never arise in the same family. The syndrome presents in all races and with equal frequency in both sexes. A variant of the condition is called Klippel-Trenaunay-Weber syndrome, which is seen in children who have extensive involvement of the limbs and trunk. The glaucoma seen in Sturge-Weber syndrome occurs in anywhere from 30 to 70% of patients. It may be associated with outflow obstruction by congenital malformation of the anterior chamber angle. It may be related to hypersecretion from an associated angioma of the choroid and most probably is related to the EVP of the episcleral hemangioma. The prominent neurologic features include seizures, focal neurologic defects, and mental retardation. Port-wine stains are progressive lesions, and the location of the port-wine stain predicts its response to pulse dye laser treatment. Concerning the ocular manifestations, the glaucoma is usually unilateral when the cutaneous lesion affects one side, but bilateral cases do occur. The management of the glaucoma is difficult and typically requires surgery.7
The visual field defects may occur as a manifestation of involvement of the cerebral cortex. A choroidal hemangioma is present in about 40% of the cases and is sometimes very subtle and difficult to identify. It typically is described as the “tomato catsup fundus.” Glaucoma is especially common if there is involvement of the upper eyelids, and presents in early infancy 60% of the time. Some researchers advocate goniotomy as the best surgical option in younger patients because of its low complication rate and its reasonable success.30 Because of the multiple etiology, other authors believe a combined trabeculotomy/trabeculectomy is best for early onset glaucoma.31 When either of these procedures fail, the Ahmed glaucoma valve implant has been studied in a fairly large group of Sturge-Weber patients and has an acceptable success rate.32 No matter what surgery is done, approximately 25% will experience intraoperative or early postoperative choroidal detachment resulting from a rapid expansion of the choroidal hemangioma with effusion of fluid into the suprachoroidal and subretinal spaces. Maintaining a normal to high IOP throughout the surgery through the injection of a viscoelastic material into the anterior chamber may help prevent some of these intraoperative complications. Posterior sclerostomy, followed by anterior chamber reformation, should be performed in the event that an expulsive suprachoroidal hemorrhage occurs. Extreme caution is advised to prevent penetration of the choroid, because penetration would lead to a disastrous hemorrhage.
Is Glaucoma Caused by Orbital-Meningeal Shunts— the Dural Shunt Syndrome (DSS)?
Dural fistulas are communications between the cavernous sinus and an extradural branch of the external or interior carotid artery. The fistulas generally have lower blood flow and lower mean pressure. The clinical appearance in these patients is far less dramatic than the appearance of those with CCSF. These patients lack bruits, and have a variable exophthalmos and variable limitations of motility. However, the conjunctival episcleral vessels have the same corkscrew, arterialized appearance and the IOP is elevated. This condition is commonly seen in elderly women with no precedent history of trauma. Dural fistulas can close spontaneously and may not require treatment. All attempts should be made to control the elevated IOP with medications until the dural shunt resolves. In most of these cases, the elevated IOP is secondary to EVP and is a well-recognized feature of DSS. However, shallowing of the anterior chamber is a rare finding, as is ocular ischemia with rubeosis. Fiori et al33 presented three cases with elevation of IOP and angle shallowing, while one case also exhibited rubeotic glaucoma. Abnormalities of vision can also occur with vascular disorders involving the occipital lobe. Arteriole and venous disease may cause loss of visual field, distortion of vision, visual hallucinations, and palinopsia. Seven patients have been so described by Kupersmith et al,34 although there is no mention of glaucoma in these patients. These dural shunts frequently have been misdiagnosed early in the course of the disease, and conditions to be ruled out include migraines, cluster headaches, endocrine ophthalmopathy, chronic conjunctivitis, episcleritis, iritis, and orbital tumor.35 An unusual carotid artery fistula was reported by Nagaki et al36 in a 77-year-old woman following routine cataract surgery. At the 1-month follow-up visit, a choroidal detachment was noted in the eye and a CT scan showed enlargement of the superior ophthalmic vein. Furthermore, cerebral angiography revealed fistulas between the meningeal branch of both the internal and external carotid arteries and the cavernous sinus. Neurosurgical treatment was performed and the symptoms disappeared.
Are Carotid-Jugular Venous Shunts Associated with Glaucoma?
Atypical causes of “red eye shunt syndrome” were reported in 1961.4 The researchers studied 14 cases of glaucoma caused by increased EVP with an extraocular origin. They believed that the fistula was from the carotid artery directly into the jugular complex, and was a low-flow fistula. They did tonographic studies in the patients and concluded that there was a relatively normal outflow facility. As cited by others, Nordman is credited by Weinreb and Karwatowski4 with reporting intraocular vascular shunts concerning arteriole venous fistulas, increased EVP, and glaucoma. Further detailed analysis on this subject is unavailable at this time due to a lack of translation.
Do Intraorbital Vascular Shunts Cause Glaucoma?
Arterial venous shunts in the orbit are quite rare, and most are a part of more extensive intracranial or facial arterial venous malformations (AVMs). Of over 600 orbital tumors studied by Wright,37 only three were AVMs. These lesions were congenital with numerous large feeding arteries, a central nidus, and numerous dilated draining veins. In contrast to the AVMs, arterial venous fistulas are characterized by a single arteriovenous connection within the vascular mass. Most of these fistulas in the orbit occur after an injury to an ethmoidal artery caused by fracture of the ethmoid bone and rupture of the artery into the ophthalmic venous system. Recently, it has been reported that a spontaneous arterial venous fistula occurred in the orbit of a 73-year-old woman with a 1-year history of mild proptosis.38 She did in fact have a glaucoma, and the hemodynamic characteristics of this fistula were quite complicated. The conclusion was that a complete analysis of the hemodynamics by means of selective cerebral angiography was needed for differential diagnosis between these conditions.
Lacey et al39 have undertaken a systematic review of these lesions as part of a continuum of research on the subject of vascular lesions of the orbit. They presented a large collection of patients seen over a 20-year period with orbital vascular malformations studied in a variety of ways. They were specifically interested in the distensible venous malformations. What was unique about their study was that a selected group of patients underwent intraoperative venography and embolization of their malformations. Direct intralesional venography identified the extent of the lesion and the drainage pathway. Pressure was used to achieve control of outflow, which upon angiography confirmation was followed by injection of a cyanoacrylic glue mixture into the lesion to form a cast. The vascular lesion and its cast were excised in a relatively blood-free procedure. This may represent the current state of the art for dealing with these lesions. The authors comment that it is particularly important that the hemodyamics of the venous malformation be understood before embolization is performed. Occlusion of the drainage pathway of a lesion will lead to expansion or stasis within any remaining portion if it is not completely excised. Such altered hemodyamics may favor postoperative thrombosis or hemorrhage and this may be the cause of some of the more serious complications that have been seen in the past.
Do Idiopathic or Sporadic Cases of Increased EVP Occur and Cause Glaucoma?
Patients with dilated episcleral vessels with elevated IOP frequently occur with exophthalmos. These are typically caused in the conditions of carotid cavernous fistula, dural arteriovenous shunts, orbital varices, and pulsatile exophthalmos. Dilated episcleral veins without exophthalmos have been described in patients with dural arteriovenous fistulas, in familial cases, in idiopathic cases,40 sometimes in patients with Sturge-Weber, in patients with advanced glaucoma, and in those with extraocular venous obstruction. Talsman et al41 reported six unilateral cases and one bilateral case of dilated episcleral veins with elevated IOP without exophthalmos. They were careful to rule out the common causes of this syndrome. Their workup included orbital venography and carotid arteriography. Inflammatory stenosis of the jugular veins and superior vena cava obstruction were ruled out on clinical grounds. Intraocular tumors were also excluded because there were no sentinel vessels. They believe that this condition is common. Moreover, the authors stressed that mistakes often occur in working up patients who have a chronic red eye and have been erroneously described as having a chronic conjunctivitis. Absence of diffuse congestion of the conjunctival vessels with elevation of IOP and accompanying glaucomatous optic disc cupping and pallor should alert the clinician to initiate a serious workup.
Are There Familial Causes of Increased EVP and Glaucoma?
Glaucoma associated with idiopathic elevated EVP was found in two members of a family and reported by Minas and Podos42 in 1968. Both were affected unilaterally with large episcleral veins, significantly elevated EVP, raised IOP, cupping of the disc, open angles with budding shunt vessels, and glaucomatous field loss. One of the patient’s mother had a similar picture in both eyes. Neither case was found to have any of the entities known to produce elevated EVP.
Does Chronic Use of Systemic and/or Topical Medications Affect the EVP and Glaucoma?
The effects of various pharmacological agents on EVP have been evaluated in numerous studies. One report on pilocarpine demonstrates decreased EVP; however, these measurements were reported relatively high and were probably unreliable.43 Another investigator found that pilocarpine decreased EVP,44 and a third study found that there was no effect from pilocarpine and acetazolamide on EVP.45 Similarly, studies evaluating epinephrine’s effect had equivocal results.46,47 Clondine seems to decrease EVP, but the changes are too small to account for any change in the IOP.48 Also, in rabbits exposed to oxygen, there was a decrease in IOP and EVP.49 Some experiments have shown that exposure of the eye to cold decreases EVP.50 Recently, Netland et al51 has used calcium channel blockers in the management of low tension and open angle glaucoma. Sawada et al52 reported prevention of visual field defect progression with brovincamine in eyes with normal tension glaucoma. An interesting study analyzing topical verapamil and decreased EVP was reported by Abreu et al.53 They studied 20 normal human subjects in a prospective, double-masked, randomized, crossover placebo study. The authors reported that calcium channel blockers are frequently used for the treatment of various cardiac disorders including angina pectoris, cardiac arrhythmia, systemic hypertension, and Raynaud’s phenomenon. The calcium channel blockers reduce vascular resistance and help prevent vasospasm by blocking the entry of calcium into the cells. The ocular effects of calcium channel blockers were studied a few years ago with a flurry of activity, and their potential clinical role became apparent, especially in treating patients with normal tension glaucoma. There is typically an arterial vasodilation with reduction of arterial blood pressure. The reduction in IOP caused by calcium channel blockers may be due at least in part to increased outflow facility, with resultant effect on EVP.
Treatment and Management
It is apparent that the treatment and management of the 17 causes of increased EVP and glaucoma is challenging and individualized. In general, management of the glaucomas would involve medical treatment first, using combinations of drug classes, advancing to laser trabeculoplasty if the angle structures are normal and accessible. Filtration surgery, generally of the guarded variety with or without antimetabolites, would be the next choice. In advanced cases, implantation of glaucoma valves with or without antimetabolites or possibly cyclodestructive procedures should be considered. There are no large studies comparing surgical procedures because these conditions are relatively uncommon and present sporadically to a variety of practitioners. We should, however, be reminded that the red eye glaucomas may be a more common cause of glaucoma than is universally recognized. A careful and thorough evaluation and treatment of the underlying cause is required.
Future Considerations
Epstein9 in 1997 was the first to point out that there are some basic aspects concerning increased EVP that need investigation. First, his measurements have shown that reducing the IOP by filtering operations in the syndrome of open-angle glaucoma associated with elevated EVP does not change EVP. He concluded that the pressure in these vessels must be determined by something other than the rate of outflow of aqueous humor. After successful filtration surgery, aqueous humor is no longer restricted by the regular outflow system to enter the episcleral veins against the venous back pressure but is free to bypass the system and escape into the extravascular tissue at low IOP. Second, Epstein reports that in certain cases where there is increased EVP of idiopathic origins, no blood has been seen gonioscopically in Schlemm’s canal either before or after surgery. This despite the fact that filtration operations have made the IOP considerably lower than the pressure in the episcleral veins on the surface of the globe. It was suggested that obstruction may lie within or beyond Schlemm’s canal. Similar phenomena may be involved in the pathogenesis of reduced aqueous humor outflow, as is commonly seen with chronic elevation of EVP.
In light of the current trends to perform nonpenetrating filtering surgery,54,55 it would be interesting to know what the EVP changes are once this “lake of aqueous” has been created in the midscleral space. Once identified, pharmacologic modulation may enhance filtration and long-term success.
Pharmacologic manipulations of the EVP in unoperated eyes are another area of active research. Abreu et al53 did a prospective, randomized, double-masked, crossover, placebo-controlled study testing one eye of 20 normal subjects with either the calcium channel blocker verapamil or placebo. Their results indicate that a single drop and a 2-week administration of topical verapamil decreased IOP and EVP significantly, with more pronounced reduction at the 2-week treatment than after a single dose treatment. The mechanism of the calcium channel blockers has been discussed by Netland et al51 and Sawada et al.52 There may be a future in this area of investigation, especially concerning the treatment of low-tension glaucoma patients. Because the calcium flux can affect the aqueous humor dynamics, there may be a hydrostatic component caused by an efferent arterial blood pressure and ciliary body perfusion and an osmotic component caused by an effect on the active secretion of sodium, calcium, and other ions by the ciliary epithelium. The mechanism may be modulation of aqueous outflow by decreasing EVP.
The complexity of the control mechanism for vascular plexus involved in episcleral venous drainage has recently been examined by Selbach et al,5 using scanning electron microscopy of vascular resin casts of the rat and rabbit eye. They also did fluorescein immunohistochemistry to investigate the multiple neuropeptides in these areas. They discovered that the episcleral arteriovenous anastomosis connects arterioles directly with the episcleral venous plexus, which also drains the aqueous humor. The nerve fiber layer plexus around the episcleral arteriovenous anastomosis is far more dense than around the arteriovenous connections at the limbal arcade. They concluded that there is an elaborate innervation in this area that may be involved in subtle modulations of the blood flow and possibly of the aqueous humor outflow dynamics. Basic anatomic research would be helpful in humans, as well as possible pharmacologic manipulation of these various neuropeptides.
References
1. Bigger JF: Glaucoma with episcleral venous pressure. South Med J 1975;68:1444–1448.
6. Warwick R: Eugene Wolff’s anatomy of the eye and orbit, 7th ed. Philadelphia: WB Saunders, 1976.
10. Kupfer C: Clinical significance of pseudofacility. Am J Ophthalmol 1973;75:193–204.
14. Talusan ED, Schwartz B: Episcleral venous pressure. Arch Ophthalmol 1981;99:824–828.
16. Jorgensen JS, Guthoff R: The role of episcleral venous pressure in the development of secondary glaucoma. Klin Monatsbl Augenheilkd 1988;193:471–475.
18. Lokich JJ, Goodman R: Superior vena cava syndrome. JAMA 1975;231:58–61.
33. Fiore PM, Latina MA, Singleton BJ, et al: The dural shunt syndrome. Ophthalmology 1990;97:56–62.
37. Wright JE: Orbital vascular anomalies. Trans Am Acad Ophthalmol Otolaryngol 1974;78:606–616.
48. Krieglstein GK, Langham ME, Leydhecker W: The peripheral and central neural actions of clonidine in normal and glaucomatous eyes. Invest Ophthalmol Vis Sci 1978;17:149.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


