5 ![]()
Definition
It is not entirely clear what disease the ancient Greeks referred to as γλαυκωμα.1 Although it is certainly likely that some of the eyes were actually glaucomatous, it was not until the early 20th century that the true nature of the family of diseases that we now call the glaucomas was recognized.
Advances in the instrumentation of ophthalmoscopy, tonometry, and gonioscopy enabled keen observers to distinguish glaucoma from other maladies of the eye and then to subdivide the glaucomas into more distinct entities. These advances culminated in the 1930s with Barkan’s gonioscopic studies, which laid out the current system for classification of the glaucomas into those with open angles and those with closed angles.2,3
What Is Primary Angle-Closure Glaucoma?
Primary angle closure is apposition or adhesion of the iris to the trabecular meshwork as a result of crowded anterior segment anatomy in a predisposed eye. Primary angle closure must be differentiated from secondary forms of angle closure, where iris tissue blocks the angle as a consequence of another preexisting ocular disease such as neovascular glaucoma associated with diabetes or retinal vein occlusion, aphakic and pseudophakic pupillary block, uveitis, iridocorneal endothelial (ICE) syndrome, or phacomorphic glaucoma. Table 5–1 lists conditions to be considered in the differential diagnosis of secondary angle-closure glaucoma.
Neovascular glaucoma |
Central retinal vein occlusion |
Uveitis |
Iris bombé |
Iridocorneal endothelial (ICE) syndrome |
Following scleral buckling or panretinal photocoagulation |
Malignant (ciliary block) glaucoma/aqueous misdirection |
Ciliary body swelling, inflammation, or cyst |
Phacomorphic glaucoma |
Subluxated lens |
Nanophthalmos |
Posterior segment tumors |
Under What Circumstances Does Primary Angle Closure Occur? What Are Its Underlying Mechanisms?
RELATIVE PUPILLARY BLOCK
Relative pupillary block is, by far, the most common of the two mechanisms for primary angle closure.4 Predisposed eyes are usually small and hyperopic with crowded anterior segments. In such eyes, the contact between the lens and iris at the pupil is more snug than normal, as shown in Figure 5–1A. This lens–iris contact tightens with the enlargement of the crystalline lens as a normal consequence of aging. In predisposed eyes, at a critical pupillary diameter (4–6 mm), the resistance to the flow of aqueous from posterior chamber through the pupil and into the anterior chamber, called relative pupillary block, causes fluid pressure to build behind the iris as shown in Figure 5–1B. This pressure differential pushes the peripheral iris forward into the angle, against the trabecular mesh-work, causing appositional and eventually permanent synechial angle closure, as illustrated in Figure 5–1C. As a result, the intraocular pressure (IOP) rises.
The possibility of inducing acute angle closure with pharmacologic mydriasis has contributed to a reluctance among primary care physicians to dilate the pupil for diagnostic ophthalmoscopy. In a predominantly black and Caucasian population, the risk of inducing angle closure by dilating the pupil is less than 1% and is approximately 0.3% if patients are screened for family history of glaucoma and for shallow anterior chamber with a penlight.5 The recognition of retinal disorders is greatly enhanced by mydriasis. Therefore, it would appear that the benefits of earlier detection of such a common blinding condition as diabetic retinopathy alone outweigh this small risk of angle closure from pharmacologic mydriasis.
Obviously, a peripheral iridectomy, as shown in Figure 5–2, eliminates relative pupillary block by providing an alternative route for aqueous to flow from the posterior chamber into the anterior chamber, thereby equalizing the pressure difference between the two. This allows the iris to fall away from the angle structures, relieving the angle closure in areas where it has not yet become synechially attached to the trabecular meshwork.
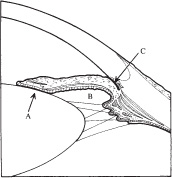
Figure 5–1. Relative pupillary block: snug iridolenticular contact at the pupil (A) with resultant increased fluid pressure in the posterior chamber relative to the anterior chamber (B) pushes the peripheral iris forward, against the trabecular meshwork, closing the angle (C). (Modified from Shields MB: Textbook of Glaucoma, 4th ed. Baltimore: Williams & Wilkins, 1998:178.)
PLATEAU IRIS SYNDROME
Plateau iris syndrome is a much less common mechanism for primary angle closure than relative pupillary block and is not affected by iridectomy.6–9 Thus, it is imperative that all eyes with primary angle-closure glaucoma be examined gonioscopically after iridectomy, to be certain that persistent angle closure/ closability from plateau iris syndrome, as shown in Figure 5–3C, is not overlooked.
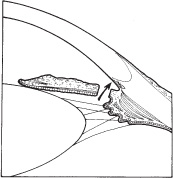
Figure 5–2. Relief of relative pupillary block with iridectomy by providing an alternate pathway for aqueous to flow from posterior to anterior chamber (arrow). With fluid pressure equal in posterior and anterior chambers, the iris falls away from the angle in areas where it is not yet synechially attached. (Modified from Shields MB: Textbook of Glaucoma, 4th ed. Baltimore: Williams & Wilkins, 1998:188.)
As the name suggests, the iris plane in plateau iris is flat and not convex. As a result, the axial anterior chamber depth is normal, or nearly so, whereas the peripheral iris contour is abnormally convex and lies in close proximity or is apposed to the trabecular meshwork, as shown in Figure 5–3A. When the pupil dilates in such an eye, iris tissue is pushed against the trabecular meshwork, closing the angle. Ultrasound biomicroscopic studies have shown that the underlying anatomic mechanism for plateau iris is abnormally anteriorly placed ciliary processes.6,9 These ciliary processes, which lie just underneath the peripheral iris roll, cause plateau iris by holding the peripheral iris forward, even after iridectomy. Because plateau iris syndrome has nothing to do with resistance to flow of aqueous through the pupil, iridectomy does nothing to resolve it.
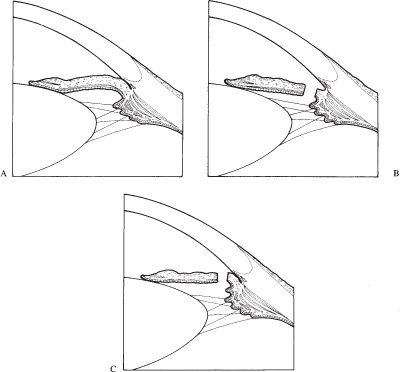
Figure 5–3. Plateau iris configuration and syndrome (A) In most eyes with an iris in plateau configuration, this is the appearance of the iris prior to iridectomy. (B) The predominant mechanism for angle closure is actually relative pupillary block and is therefore relieved by iridectomy. (C) In those rare cases where angle closure/closability persist after iridectomy, the term plateau iris syndrome is used. (Modified from Shields MB: Textbook of Glaucoma, 4th ed. Baltimore: Williams & Wilkins, 1998:179.)
Terminology can be confusing, but is useful and important. When a plateaulike iris is observed with slit-lamp biomicroscopy and gonioscopy prior to iridectomy, as shown in Figure 5–3A, it is termed plateau iris configuration. Despite this appearance of the iris and chamber angle, and the surgeon’s suspicion that iridectomy may fail to open the angle, relative pupillary block is usually the predominant mechanism for the angle closure in a majority of these eyes and, as illustrated in Figure 5–3B, iridectomy is curative of the angle closure stimulus. If plateau iris and angle closability persist after iridectomy, this rare situation, shown in Figure 5–3C, is termed plateau iris syndrome. Plateau iris syndrome is rare, but should be ruled out following iridectomy in all eyes with primary angle closure. In addition, the surgeon should have a heightened index of suspicion for the presence of plateau iris in younger and/or myopic patients with primary angle closure.
Although it is usually detected during gonioscopy shortly after iridectomy, plateau iris syndrome may also appear years later. For this reason, careful gonioscopy should be performed periodically for the remainder of the patient’s life after iridectomy for primary angle closure, to detect progressive closure/closability of the angle due to plateau iris syndrome. The plateau iris syndrome may vary in its anatomic degree, depending on the physical height of the iris plateau relative to the adjacent angle structures. If the plateau is opposite the anterior trabecular meshwork or Schwalbe’s line, when the angle is crowded, the trabecular meshwork is obstructed and the IOP rises. However, in some cases the plateau may only be as high as the scleral spur or posterior trabecular meshwork so that angle crowding does not cause trabecular obstruction and elevated IOP.
Epidemiology and Importance
What Factors Anatomically Predispose Eyes to Primary Angle Closure?
AGE
The prevalence of increased relative pupillary block and primary angle closure increases with age, in tandem with the natural increase in volume of the crystalline lens and decrease in resting pupil diameter. The prevalence of primary angle-closure glaucoma peaks in the sixth decade, earlier than with primary open-angle glaucoma.
RACE
Among Caucasians, 75 to 90% of glaucoma cases are due to primary open-angle glaucoma, affecting 0.5 to 2.16% of the adult population.10 This is in sharp contrast to the much lower prevalence of primary angle-closure glaucoma in this population, ranging from 0.09 to 0.17%. Population-based studies demonstrate that this relationship is reversed in Eskimos: 2.12 to 2.9% for primary angle-closure glaucoma compared to 0.01 to 0.4% for primary open-angle glaucoma.11–16 The prevalence of primary angle-closure glaucoma is 20 to 40 times higher among Eskimos than Caucasians.
Primary angle-closure glaucoma in Asian populations has also been studied, albeit less extensively than in Eskimos. It appears that the prevalence of primary angle-closure glaucoma among Asians is intermediate between that in Caucasians and Eskimos. It has been estimated that primary angle-closure glaucoma affects more than 30 million people worldwide, at least as many as primary open-angle glaucoma.17
Primary angle closure is less common in blacks than Caucasians. When angle closure does occur in black patients, the chronic form is the most common.
SEX
Primary angle closure in Caucasians and especially among Eskimos, is more common in females, perhaps due to a smaller anterior segment. In black patients, the incidence of primary angle closure is equal in males and females.
REFRACTIVE ERROR
Refractive error definitely influences the likelihood of primary angle closure. Because hyperopes have smaller anterior segments than emmetropes or myopes, increased relative pupillary block and primary angle closure are more common in hyperopic eyes. In myopic eyes with primary angle closure, especially in younger patients, plateau iris syndrome should be suspected as a mechanism.
FAMILY HISTORY
Primary angle closure is believed to be inherited in some cases, although a positive family history does not predict the likelihood of a future attack of acute angle-closure glaucoma.
How Is Gonioscopy Most Effectively Used in the Diagnosis and Management of Primary Angle Closure?
Gonioscopy should be performed on all patients with glaucoma, on all glaucoma suspects, and on all individuals suspected of having narrow angles. Without it, identification of the underlying mechanism and therefore the appropriate treatment of any glaucomatous condition is impossible. Skillful gonioscopy is important in the diagnosis of glaucoma, but also in its treatment, for example, in performing laser trabeculoplasty and laser gonioplasty.
Visualization of the angle structures requires a contact lens. Table 5–2 lists the common gonioscopic techniques with their respective advantages and disadvantages.
KOEPPE GONIOSCOPY
Koeppe gonioscopy is a direct method of visualizing the chamber angle by using a dome-shaped goniolens, an illumination system, and a hand-held biomicroscope.
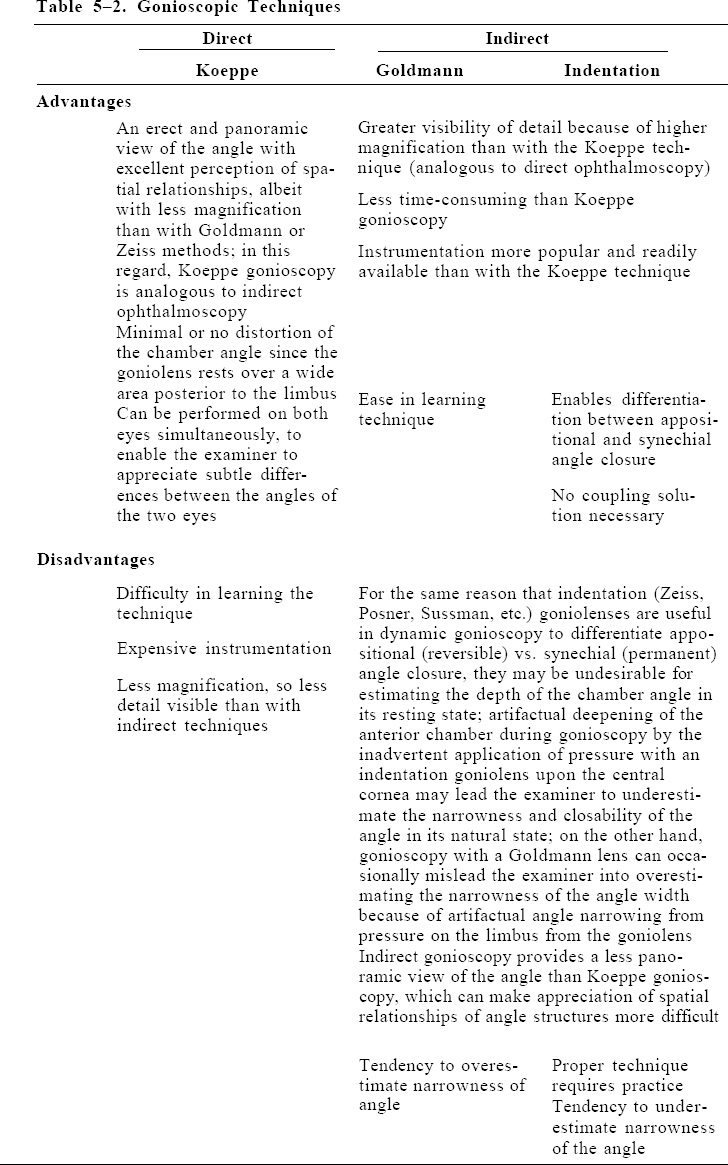
GOLDMANN AND INDENTATION GONIOSCOPY
Goldmann and indentation gonioscopy are indirect methods of visualizing the chamber angle in the mirror of a gonioprism with a slit-lamp microscope. Indirect gonioscopy provides an inverted image, but the right-left and up-down orientations are maintained.
What Questions Should Be Answered with Gonioscopy in Primary Angle-Closure Glaucoma?
Three questions should be answered with gonioscopy when evaluating a patient for angle closure:
IS THE ANGLE OPEN OR CLOSED IN ITS NATURAL POSITION?
The ideal method of observing the angle in its natural position is Koeppe gonioscopy.18 However, special instruments are required and so, from a practical point of view, indirect gonioscopy is more convenient for most ophthalmologists. Clinicians should use the method with which they are most comfortable and confident. The avoidance of artificial distortion of the angle during gonioscopy, especially with indentation lenses, is crucial to the evaluation of the natural position of the angle.
IF ANGLE CLOSURE EXISTS, Is IT APPOSITIONAL (REVERSIBLE) OR SYNECHIAL (PERMANENT)?
Indentation gonioscopy, as described by Forbes,19,20 is a technique wherein one uses a contact lens (Zeiss, Posner, Sussman, etc.) with a small area of corneal contact to push aqueous from the central to peripheral anterior chamber to artificially open the angle. Areas of appositional closure of the angle, in which the peripheral iris is resting upon but is not yet adherent to the trabecular meshwork, can be opened by moving the iris away from the angle structures with this dynamic indentation gonioscopy. This maneuver brings into view any peripheral anterior synechias where the iris is adherent to the angle.
The extent of synechial versus appositional closure is of critical importance because, following relief of relative pupillary block with iridectomy, the control of intraocular pressure will depend on the fraction of trabecular meshwork circumference not yet closed with synechias. Areas of synechial closure remain closed following relief of the angle closure mechanism and are therefore permanently unavailable for aqueous outflow except in certain cases of acute angle closure where fresh peripheral anterior synechias can be successfully broken with laser gonioplasty or surgical goniosynechialysis.21–23 The extent of appositional versus synechial angle closure was a much more serious issue prior to the introduction of laser iridectomy, when surgical peripheral iridectomy was required to relieve pupillary block. In cases where surgical iridectomy failed to control the IOP, a second trip to the operating room for a filtration operation was then necessary.
IF OPEN, IS THE ANGLE CLOSABLE?
What Role, If Any, Does Provocative Testing Play in the Management of Primary Angle-Closure Glaucoma?
Provocative testing has little, if any, role. Before the availability of modern laser iridectomy techniques, the relief of pupillary block required a surgical iridectomy. Although relatively safe, this procedure poses the usual uncommon but unavoidable risks of intraocular surgery. In the past, to minimize unnecessary surgical iridectomies, provocative tests were employed to try to estimate the closability of the angle in a particular eye by inducing angle closure artificially. Although provocative tests are rarely used today, it is useful to be aware of their existence and physiologic bases.24–26
The ideal provocative test for angle closure would be physiologic, simple, not time-consuming, reproducible, and safe. No provocative test meets all of these criteria. A positive provocative test is no guarantee that a patient will indeed develop angle closure, just as a negative test does not assure immunity from a subsequent angle closure attack. Why, then, should one bother with provocative testing? These tests can be used as adjuncts to bolster one’s clinical impression, and they are useful in the rare circumstance where laser iridectomy is unavailable or not possible. Ultimately, the decision to treat an asymptomatic patient with laser iridectomy because of narrow angles rests on the clinical judgment of the ophthalmologist. If the ophthalmologist decides that laser iridectomy is not necessary in a patient with narrow angles, the patient should be alerted to the symptoms and dangers of acute and subacute angle closure and should have periodic examinations including careful gonioscopy. The role of provocative testing in answering the question of closability of the angle is minor, especially when one considers the availability and safety of modern laser iridectomy.
Diagnosis and Differential Diagnosis
How Does the Patient with Primary Angle Closure Present to the Ophthalmologist?
Primary angle closure presents one of three clinical pictures: acute, subacute, or chronic:
ACUTE PRIMARY ANGLE-CLOSURE GLAUCOMA
Acute angle-closure glaucoma presents as an emergency with abrupt onset and rapid elevation in IOP. The striking signs and symptoms are listed in Table 5–3. The differential diagnosis of acute primary angle-closure glaucoma, as shown in Table 5–4, must be considered. Uveitic, neovascular, and other secondary acute glaucomas can mimic primary angle closure and lead to incorrect diagnosis and inappropriate treatment.
| Signs | Symptoms |
|---|---|
| Significant elevation of intraocular pressure (IOP) The very high pressure suppresses aqueous production; as a result, the pressure is often subnormal for a variable period of time following relief of the acute angle closure attack, even if much of the angle is permanently closed with synechiae Fixed, mid-dilated pupil (commonly vertically oval) Steamy cornea (epithelial edema due to elevated IOP) Anterior chamber flare and cells (may have “pseudo KPs,” but never true keratatic precipitates) Shallow peripheral anterior chamber (van Herick et al28); axial depth of the anterior chamber varies with the mechanism of angle closure, e.g., shallow with malignant glaucoma or nanophthalmos, deeper with relative pupillary block and normal or nearly so with plateau iris Gonioscopy: the diagnosis of acute angle closure requires gonioscopic confirmation of a closed angle; if the cornea is too hazy for visualization of the angle structures, topical glycerin may help to clear epithelial edema and permit examination of the angle Important: remember to perform gonioscopy on the fellow eye since primary angle closure is almost always bilateral; if the angle in the fellow eye is wide open, suspect a diagnosis other than primary angle closure such as neovascular, uveitic, or phacomorphic glaucoma (see Table 5–4) Indentation, “dynamic,” or “compression” gonioscopy with a Zeiss, Posner, Sussman, or another similar lens can be used to assess the extent of synechial (permanent) versus appositional (reversible) angle closure; this provides a clue as to the fraction of the angle that will open when the mechanism for angle closure is eliminated, usually with iridectomy; compression gonioscopy is also therapeutic for an acute attack (it pushes aqueous from the central to peripheral anterior chamber, which temporarily opens the angle so that aqueous can reach the trabecular meshwork and escape from the eye)Sector gray atrophy of the iris stroma; rarely, this atrophy can cause a spontaneous and lasting cure of angle closure by altering of the lens/iris interface, relieving relative pupillary block Glaukomflecken (permanent whitish anterior lens opacities, which are evidence of an existing or prior acute elevation in IOP) Disc hyperemia and edema early in the acute attack, the disc becomes atrophic later, with the extent of pallor often outweighing that of cupping Nonspecific visual field constriction, which is occasionally reversible, especially in younger patients Bradycardia | The headache and nausea of acute angle closure often masquerade as a nonocular medical illness, the negative workup of which delays diagnosis and treatment of the angle closure attack, thereby increasing the chances of a poor outcome Pain (browache) |
SUBACUTE (INTERMITTENT, PRODROMAL, OR SUBCLINICAL) PRIMARY ANGLE-CLOSURE GLAUCOMA
Subacute angle closure is characterized by periodic and self-limited attacks of mild ocular pain and blurred vision.27 The history provided by the patient is often vague, but the examiner should listen carefully. Complaints of colored rainbows around lights, signifying corneal edema, should automatically trigger a gonioscopic examination, even if the IOP is normal and the angle seems deep upon slit-lamp examination. These rainbows differ from the monochromic halos around lights of which a patient with cataract might complain. Halos are not due to corneal edema, and therefore are not colored. Symptoms of subacute angle closure are typically greatest in the evening and usually improve by morning, presumably due to lessening of angle closure from the miosis of sleep. Because subacute angle closure can progress to acute or chronic angle closure, it is important to suspect it and perform gonioscopy on all patients giving a peculiar history of intermittent eye or brow discomfort or dull ache, blur, or transient monocular visual loss, even if the peripheral anterior chamber appears deep upon slit-lamp examination. The slit-lamp examination can mislead the examiner into assuming, incorrectly, that the angle is open. If angle closure is allowed to continue undetected, progressive irreversible synechial angle closure will result. This condition often leads to a glaucomatous situation no longer manageable with laser iridectomy, but only with filtration surgery.
Anterior uveitis |
Neovascular glaucoma |
Iridocorneal endothelial (ICE) syndrome |
Central retinal vein occlusion |
Ciliary body swelling, inflammation or cysts |
Following scleral buckling or panretinal photocoagulation |
Malignant (ciliary block) glaucoma/aqueous misdirection |
Phacomorphic glaucoma |
Subluxated lens |
Phacolytic glaucoma |
Nanophthalmos |
Posterior segment tumors |
CHRONIC PRIMARY ANGLE-CLOSURE GLAUCOMA
Chronic angle closure has no symptoms. It develops over a long period of time, occasionally in patients with preexisting primary open-angle glaucoma. Therefore, it is essential that all glaucoma patients have initial and periodic gonioscopy, no matter how deep the peripheral anterior chamber appears at the slit lamp. When the IOP control in a patient being treated for chronic open-angle glaucoma becomes more difficult than previously, gonioscopy may reveal that chronic angle closure has begun, with varying amounts of appositional and/or synechial closure. In a predisposed, usually hyperopic, eye, as the patient ages and the crystalline lens enlarges, relative pupillary block increases, which can cause slowly progressive angle closure. This situation is occasionally discovered at the time of laser trabeculoplasty that has been scheduled for what is believed to be uncontrolled open-angle glaucoma. In such cases, laser iridectomy is necessary to relieve pupillary block and interrupt the progression of permanent synechial angle closure. Following the elimination of the underlying cause of the angle closure, medical therapy, laser trabeculoplasty, or surgical therapy are employed, as needed, for IOP lowering.
The depth of the peripheral anterior chamber as visualized at the slit lamp, although very useful in most cases for estimating the closability of the angle, can be very misleading and must not take the place of careful gonioscopy.28 Unless careful gonioscopy is periodically performed on all glaucoma patients, the assumption that an angle, based on the slit-lamp examination, is open and not closable can lull the ophthalmologist into a dangerously false sense of security. In the early stages of chronic angle-closure glaucoma, permanent synechial angle closure can progress despite normal IOP, especially if aqueous suppressant therapy, such as carbonic anhydrase inhibitors or topical beta-blockers, are used. Eventually, a critical fraction of the circumference of the trabecular meshwork becomes permanently closed with synechias. At this point, the remaining fraction of the angle that is still open provides insufficient facility of outflow to keep pace with aqueous production, and the IOP rises. In many such cases, following relief of pupillary block with iridectomy, the pressure remains high despite medications and laser trabeculoplasty, and filtration surgery is required. In chronic primary angle-closure glaucoma, even if glaucoma medications successfully lower the IOP, laser iridectomy is necessary to preserve that portion of the angle not yet closed with peripheral anterior synechias. It is very difficult to predict in which cases of primary angle closure the IOP will be controlled with iridectomy alone, and which cases will require filtration surgery. Because laser iridectomy is relatively safe compared to filtration surgery, it should be performed, if possible, in all cases. Then if the IOP remains unacceptably high, despite the maximum benefit from glaucoma medications and laser trabeculoplasty to the remaining open angle, surgery can be performed.
Treatment and Management
How Is Primary Angle Closure Treated?
The first goal in the management of primary angle closure is to eliminate relative pupillary block with an iridectomy. The initial evaluation of primary angle closure and its management is depicted in Figure 5–4, culminating in laser iridectomy. In the case of acute angle closure, the cornea is often too edematous to permit laser. One must first break the attack medically to allow the cornea to clear. Acute angle closure is an emergency and must be resolved quickly to protect the optic nerve from pressure-induced damage and to prevent permanent synechial angle closure. Then, once iridectomy has eliminated relative pupillary block, the patient must be carefully reevaluated for the important, but often neglected, management necessary after iridectomy, which is diagrammed in Figure 5–5.
How Is an Attack of Acute Primary Angle Closure Treated?
MEDICAL THERAPY
Drugs that are useful in the treatment of acute angle closure glaucoma are listed in Table 5–5.
Hyperosmotic Drugs Hyperosmotics are the cornerstone of medical therapy for acute angle-closure glaucoma. Because they lower the IOP by shrinking the volume of the vitreous, hyperosmotics work independently of neuromuscular action of the iris and of the production of aqueous. Until iris muscular paralysis due to pressure-induced ischemia is relieved by the lowering of IOP provided by hyperosmotic drugs, pilocarpine, a direct parasympathomimetic, cannot stimulate the pupillary sphincter to cause needed miosis. Also, since the production of aqueous humor is significantly depressed by the acute pressure elevation, aqueous suppressants such as beta-blockers and carbonic anhydrase inhibitors, although helpful, cannot by themselves break an acute attack.
If at all possible, the patient should have nothing to eat or drink prior to the administration of hyperosmotics and for 2 hours afterward. Ice chips can be given for thirst, if necessary. In addition, oral hypersomotics commonly cause nausea and occasional vomiting in the already ill patient. This can interfere with their administration and retention. Injectable antiemetic medication can be useful in this situation. The patient should be observed closely and not discharged from the office immediately after hyperosmotics. Possible side effects are headache, confusion, cardiac arrhythmia, and subdural or subarachnoid hemorrhage.
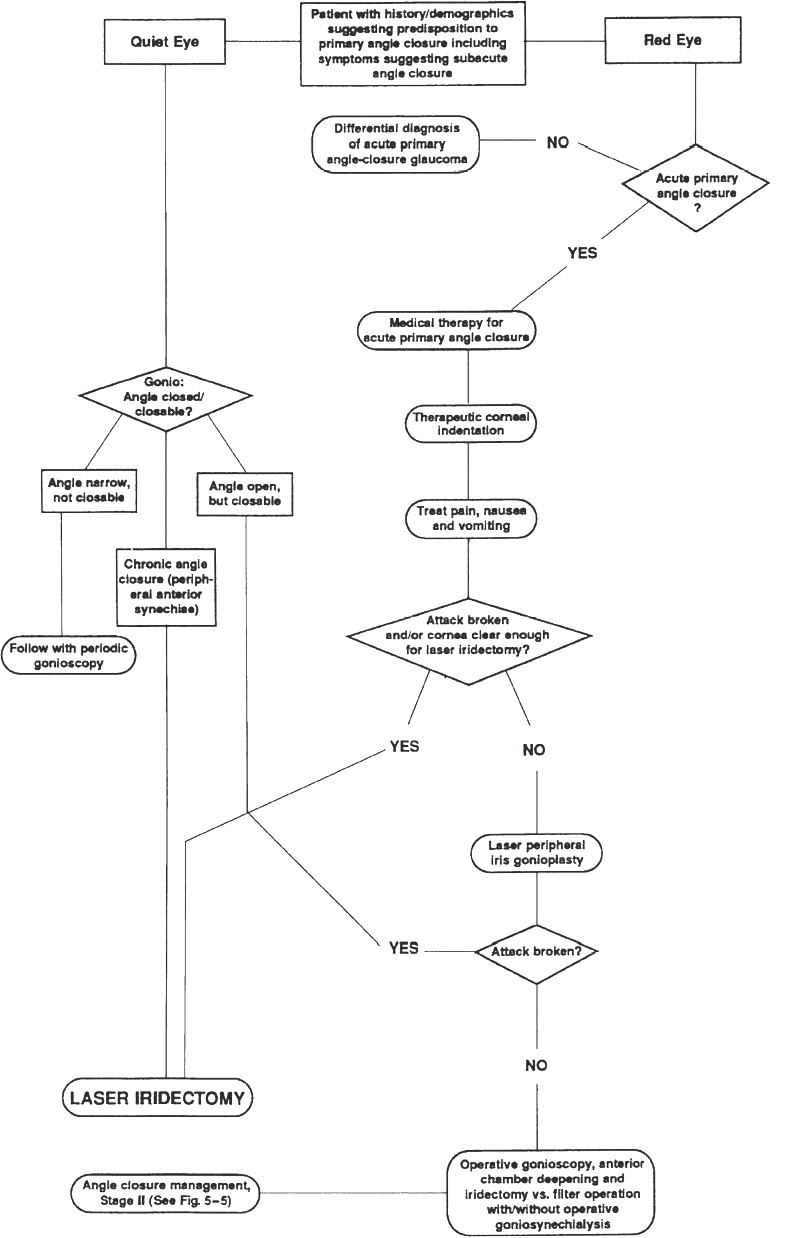
Figure 5–4. Strategy for medical and other initial therapy for primary angle-closure glaucoma, culminating in laser iridectomy.
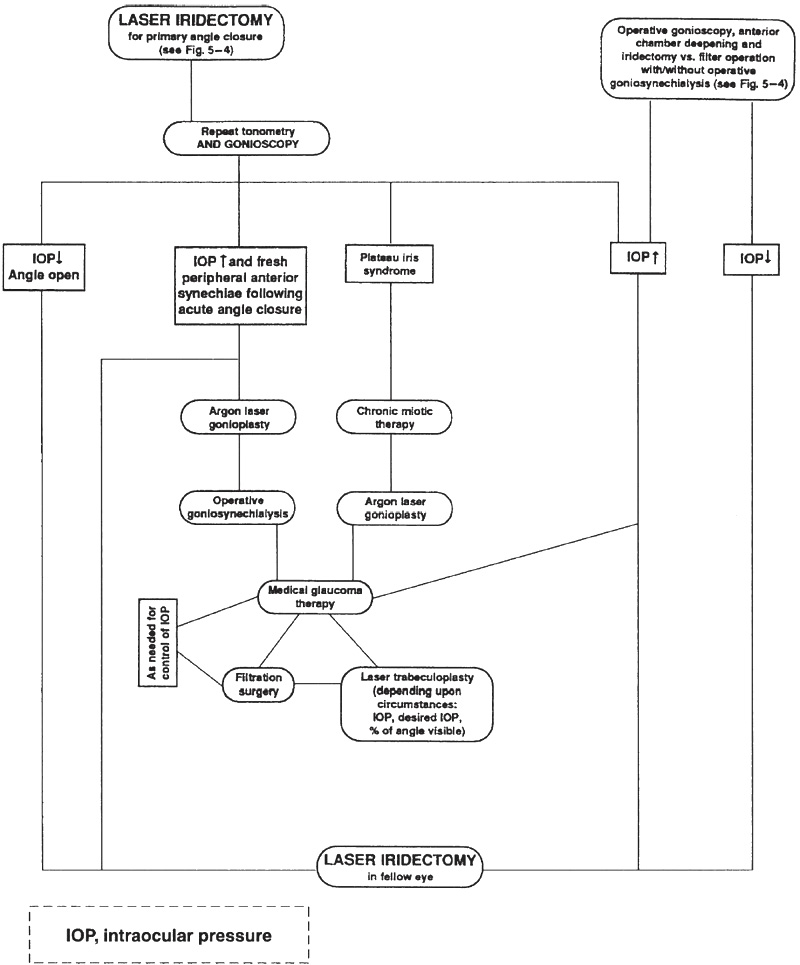
Figure 5–5. Decision tree: strategy for therapy of primary angle-closure glaucoma after iridectomy has eliminated relative pupillary block.
Other Medications
Miotics29,30,31,32, beta-blockers, carbonic anhydrase inhibitors, and alpha agonists are described in Table 5–5.
THERAPEUTIC CORNEAL INDENTATION
Indentation of the anesthetized central cornea with a sterile cotton-tipped applicator, indentation goniolens (Zeiss, Posner, or Sussman), or applanation prism (on 20 seconds, off 10, on 20, etc.) can be invaluable in breaking an acute attack of primary angle-closure glaucoma.33 Therapeutic corneal indentation works by the same principle as diagnostic indentation gonioscopy. The pressure applied to the central cornea pushes aqueous from the central anterior chamber into the peripheral anterior chamber, which opens the angle and allows aqueous to reach the trabecular meshwork. A variation on this theme was described by Kimbrough et al,34 who reported the successful relief of acute angle closure with adjunctive retrobulbar anesthesia followed by intermittent application of the “super pinkie” ocular compression device.
A. Hyperosmotics
|
B. Miotics
|
C. Topical beta blockers
|
D. Carbonic anhydrase inhibitors (CAIs)
|
E. Alpha agonists
|
PAIN, NAUSEA, AND VOMITING
Medical therapy should be provided.
LASER PERIPHERAL IRIS GONIOPLASTY
Argon laser photocoagulation can be used to shrink and flatten the peripheral iris to open the angle in attacks of acute angle-closure glaucoma that fail to respond to medications and corneal indentation.35,36 Often, the cornea is not sufficiently transparent to perform definitive laser iridectomy, but is clear enough to permit the application of laser energy to shrink the peripheral iris. In this situation, gonioplasty can be employed to open some or all of the angle to lower the IOP and clear the cornea, making subsequent laser iridectomy possible. The effect of gonioplasty is often transient and therefore is not a substitute for definitive relief of relative pupillary block with iridectomy. Similarly, attempted argon laser iridectomy, even in the absence of patency, can inadvertently “peak” the pupil in the meridian toward the laser iridectomy site, transiently relieving relative pupillary block, and breaking the acute angle-closure attack. For this reason, care must be taken to be certain that the iridectomy is patent. If it is not, the iridectomy must be completed because the transient pupilloplasty effect will usually lessen with time and eventually predispose the eye to recurrence of angle closure. In addition to its value in treating an acute attack of angle closure, argon laser gonioplasty has several other valuable uses in the management of primary angle closure as listed in Table 5–6.
What Should Be Done If the Acute Attack of Angle Closure Is Unresponsive to Medical Therapy and Laser Gonioplasty, and the Cornea Is Not Sufficiently Clear to Allow Laser Iridectomy?
In this situation, surgical iridectomy is required. The question is, Will iridectomy alone resolve the problem or should a filtration operation be performed? Before the availability of laser iridectomy, this was a common dilemma for the ophthalmologist confronted with acute angle closure. It is unpleasant for both the patient and the surgeon to have to follow one intraocular surgical procedure with another. When surgical peripheral iridectomy becomes necessary, operative anterior chamber deepening and gonioscopy allows quantification of permanent synechial angle closure in the operating room, where the decision between iridectomy and filtration surgery can be weighed.37,38 Also, at that time, operative goniosynechialysis can be used to break fresh peripheral anterior synechias to restore angle anatomy and aqueous outflow.21,22 Although operative goniosynechialysis has been successfully employed up to 1 year following acute angle closure, the earlier one can open and restore the functional anatomy of the angle, the better. Depending on how much of the angle is not yet closed with synechias, a decision must be made whether to perform iridectomy alone or as part of a filtration operation. Chandler and Simmons37 have recommended filtration surgery if more than 6 clock hours of angle are closed with synechias; surgical peripheral iridectomy alone if 4 or less clock hours are closed; and that the surgeon use his own judgment for eyes with 4 to 6 clock hours of synechial angle closure. These recommendations, although very helpful, are not foolproof. Mixed mechanism glaucoma may be present with very poor facility of outflow and high pressure, even with an entirely open angle. If, following surgical iridectomy, the IOP remains uncontrolled; glaucoma medications, laser trabeculoplasty, and glaucoma filtration surgery must be employed, as needed, to control any residual glaucoma at an acceptable level of IOP.
| Indications |
During an acute attack of primary angle-closure glaucoma, when the cornea is not sufficiently clear to allow laser iridectomy, gonioplasty can occasionally be used to open segments of the angle to help lower the pressure and clear the cornea permit definitive treatment (laser iridectomy) |
What Should Be Done After Breaking the Attack of Acute Angle Closure?
When the acute attack is broken or the cornea is sufficiently clear, proceed with laser iridectomy to eliminate pupillary block and prevent its recurrence and angle closure.39–41 Remember that after iridectomy, there is yet much work to do, even if the pressure has improved. Figure 5–5 diagrams the important, but often neglected, management of primary angle closure following iridectomy.
What Are Some Useful Guidelines for Laser Iridectomy Technique?
PRETREATMENT
- If the pupil is not already miotic from medications used to break an acute attack, constrict the pupil for a taut iris and easy penetration, for example, with pilocarpine 2 to 4% every 5 minutes for three doses until the pupil is nonreactive.
- An alpha agonist such as brimonidine 0.2% (Alphagan) or apraclonidine 0.5 or 1.0% (Iopidine), and/or other glaucoma medications are helpful in minimizing the risk of a postlaser pressure spike.42
TECHNIQUE
- The Abraham or Wise iridectomy lenses greatly facilitate iris penetration.
- Argon laser: Iridectomy with the argon laser is an art form.43–47 Unlike the neodymium:yttrium-aluminum-garnet (Nd:YAG) photodisruptive iridectomy, this photocoagulative technique must be varied depending on differences in iris color and its relative tendencies to absorb or reflect laser energy For example, “chipping away” with many high power/short exposure burns is very effective for dark brown irises. On the other hand, the “gas bubble” technique described by Hoskins and Migliazzo46 is wonderful for light blue irises. For iris coloration in between these two extremes, a variety of techniques can be used such as the Simmons-Deppermann “drumhead” technique.47 These methods are listed in Table 5–7; however, numerous techniques have been used successfully. This list may serve as a starting point from which surgeons can refine their own techniques.
- Nd:YAG laser: The action of Nd:YAG photodisruptors, unlike argon laser photocoagulators, is independent of the propensity of the iris to absorb or reflect laser energy.48,49 With the Nd:YAG laser, the same iridectomy technique can be used regardless of iris color. However, thin, light blue irises are more easily penetrated with Nd:YAG laser than thick, dark brown ones.
- Site of iridectomy:
- Base of iris crypt or thin spot
- Iris freckle, if argon laser used
- Avoid visible blood vessels, especially with Nd:YAG
- Peripheral site, especially if Nd:YAG used, to avoid damage to the underlying crystalline lens.
- Use the 2 or 10 o’clock position, so that the iridectomy is under the upper lid, but not the 12 o’clock position, where gas bubbles formed during the procedure can obscure visualization and interfere with completion of the laser procedure. Also, avoid creation of an iridectomy in the interpalpebral fissure (3 or 9 o’clock position) where postlaser visual symptoms and inadvertent laser damage to the macula are more likely.50
- If the procedure is going well and a second iridectomy can be made easily, some surgeons elect to perform a second iridectomy in case the first one becomes occluded later. This delayed closure is an unusual occurrence following Nd:YAG iridectomy for primary angle closure. Delayed closure is a more common problem following argon laser iridectomy, but can even occur after Nd:YAG iridectomy, especially for certain secondary angle closures such as neovascular glaucoma, uveitic glaucoma, or aphakic/ pseudophakic pupillary block.
- Use the 2 or 10 o’clock position, so that the iridectomy is under the upper lid, but not the 12 o’clock position, where gas bubbles formed during the procedure can obscure visualization and interfere with completion of the laser procedure. Also, avoid creation of an iridectomy in the interpalpebral fissure (3 or 9 o’clock position) where postlaser visual symptoms and inadvertent laser damage to the macula are more likely.50
What General Guidelines Are Useful in Nd:YAG Laser Iridectomy?
The Nd:YAG laser is useful for initial laser iridectomy and particularly for completion of unsuccessful attempts at argon laser iridectomy. One should choose a site of thin iris as far in the periphery as clear visibility permits. In the periphery of the iris, damage to the underlying crystalline lens is least likely. Precise focusing is crucial to successful Nd:YAG iridectomy, so areas of arcus senilis should be avoided, as well as visible iris blood vessels to minimize hyphema during and after the procedure. Usually, one to five single shots of 4 to 7 mJ each are required. Some surgeons prefer to use the Nd:YAG burst mode for iridectomy. However, because with most instruments the procedure can be completed with single shots, many avoid the use of the burst mode, just in case it might increase the chance of damaging the underlying crystalline lens.
| “Gas bubble” technique for light blue irises (Hoskins and Migliazzo46) |
1. Create a 1.5-mm gas bubble on the surface of the iris with 1500 mW, 50 µm, 0.2–0.5 second burn (hold down the foot pedal until the desired bubble forms) |
2. Immediately apply one or two additional shots, as needed, focused on the apex of the bubble; the gas bubble’s inner surface will re-reflect laser energy toward the iris; this will usually achieve penetration, as evidenced by a plume of brown iris pigment carried by aqueous from the posterior chamber into the anterior chamber |
3. Lower laser settings to 500–1000 mW, 50 µm, 0.05 seconds, and use multiple shots to enlarge and “clean up” the iridectomy |
| Modified “chipping away” technique for dark brown irises |
In these eyes the areas of laser application tend to fill in with surrounding iris tissue after each shot, much like trying to dig a hole in dry sand; use many high-power, short-exposure burns: 1500 mW, 50 µm, 0.02–0.05 seconds |
| “Drumhead” technique for intermediate iris colors (Simmons and Deppermann47) |
1. Tighten the proposed iridectomy site like a drumhead by surrounding it with four “stretch” burns: 100–200 mW, 200 µm, 0.2 seconds |
Active bleeding from the iris is common during Nd:YAG iridectomy, and may interfere with completion of the laser procedure. It can be temporarily controlled with the intermittent application of firm pressure upon the eye with the hand-held laser contact lens. Some surgeons minimize iris bleeding by prehearing the iridectomy site with argon laser photocoagulation.51,52 A typical method used for such pretreatment is to tighten the desired site in similar fashion to the “drumhead” iridectomy technique, by surrounding it with four spaced burns of approximately 200 mW, 200 µm, and 0.2 seconds and then coagulating the central area with 10 to 20 burns of 400 to 800 mW, 100 µm, and 0.1 seconds.47 The applications should be sufficient to tighten the iridectomy site without causing excessive pigment disruption. However, bleeding from the Nd:YAG iridectomy site very rarely causes significant problems.
It is not necessary to enlarge a small Nd:YAG iridectomy after penetration. Nd:YAG iridectomies tend to be smaller but “cleaner” than those made with the argon laser and are less prone to subsequent closure. Also, damage to the underlying lens capsule is more likely if additional photodisruption is used once a patent iridectomy has been achieved.
What Should Be Done After Laser Iridectomy?
The very important evaluation and management of the eye following iridectomy, as diagrammed in Figure 5–5, is seldom discussed and is often neglected. After laser iridectomy has relieved pupillary block, it is crucial to reexamine the eye and repeat the gonioscopy. The IOP may be improved following iridectomy, but there is much work yet to do. One-fourth of these eyes will require further treatment for glaucoma at some time in the future. In addition, 40 to 80% of fellow eyes of eyes with acute angle-closure glaucoma will have an acute attack within 5 to 10 years if they are not treated with prophylactic iridectomy. The pain and emotional upset resulting from an acute angle-closure attack in the first eye may increase sympathetic flow, induce pupillary mydriasis, and increase relative pupillary block, precipitating an acute attack of angle closure in the fellow eye during treatment of the first eye. Prophylaxis with 0.5 to 1% pilocarpine in the fellow eye is used by some, but it is not foolproof and, in some cases, can increase relative pupillary block and angle closure/closability. Prompt laser iridectomy in the fellow eye, if its angle is closed/closable, is necessary.53,54 If the angle closure is truly unilateral, one should consider the differential diagnosis of secondary angle closure in the first eye, as listed in Table 5–1.
What If Following Iridectomy, the IOP Is Down and the Angle Is Open and Not Closable?
Proceed with laser iridectomy to relieve relative pupillary block in the fellow eye if its angle is closable as shown in Figure 5–5.
What If, After Iridectomy, the IOP
Remains Elevated with Fresh Peripheral Anterior
Synechiae Following Medical Therapy and Laser Iridectomy for Acute Angle Closure?
Fresh peripheral anterior synechiae can occasionally be broken with laser peripheral iris gonioplasty and/or operative goniosynechialysis. Gonioplasty creates surface iris burns to shrink and flatten the iris tissue and pull it away from the trabecular meshwork.23 Operative goniosynechialysis has been reported to break fresh synechiae and improve facility of outflow up to 1 year following an acute attack of primary angle closure.21,22
What If, After Iridectomy, the Angle Remains Closed/ Closable from Plateau Iris Syndrome?
With plateau iris syndrome the angle is still appositionally closed/closable after iridectomy, which eliminates relative pupillary block but not the plateau iris mechanism. Remember that most cases of angle closure with plateau iris configuration, as seen gonioscopically prior to iridectomy, are actually due to increased relative pupillary block, which is cured by iridectomy. To resolve plateau iris syndrome, where angle closability persists after iridectomy, one must flatten the peripheral iris to remove it from the proximity of the trabecular meshwork with chronic miotic therapy or laser peripheral iris gonioplasty.
CHRONIC MIOTIC THERAPY FOR PLATEAU IRIS SYNDROME
Chronic miotics were the only available therapy for the prevention of progressive synechia formation in plateau iris syndrome prior to the introduction of argon laser gonioplasty. Chronic miotic therapy, such as pilocarpine 0.5 to 1% every 12 hours, is much less convenient, less well tolerated, and less dependable than laser gonioplasty, however. Dapiprazole (Rev Eyes), which achieves miosis by α-adrenergic blockade, may offer an alternative, but at this time it is costly and has a relatively short shelf life following its reconstitution.
LASER PERIPHERAL IRIS GONIOPLASTY FOR PLATEAU IRIS SYNDROME
Laser peripheral iris gonioplasty, as outlined in Table 5–6, is the preferred method of relieving the plateau iris mechanism.55,56 With this technique, argon laser burns are applied to the peripheral iris roll to shrink and pull it away from the angle. The effect is often transient, and retreatment is often necessary. Therefore, it is imperative that these eyes are followed indefinitely with periodic gonioscopy.
Remember that plateau iris syndrome may develop years after iridectomy, so periodic gonioscopy should be performed on all patients who have had iridectomy for primary angle closure.
What If, After Iridectomy, the IOP Remains Elevated Without Fresh Peripheral Anterior Synechiae and In the Absence of Plateau Iris Syndrome?
In this situation, one should proceed to medical therapy, laser trabeculoplasty, and filtration surgery, as needed for control of IOP of this open angle component of the patient’s “mixed mechanism” glaucoma.
Treat IOP with medical glaucoma therapy just as with chronic open angle glaucoma. If medical therapy is unsuccessful, consider laser trabeculoplasty, depending on the desired and existing IOP, the extent of optic nerve and visual field damage, and the fraction of the circumference of trabecular meshwork available for trabeculoplasty. For example, if the pressure is 26, the desired pressure is 18, and 11 clock hours of trabecular meshwork are available for trabeculoplasty, then it is a reasonable option. On the other hand, if the pressure is 45, the desired pressure is 16, and only 2 clock hours of meshwork are visible, then laser is a waste of time and may pose a hazard. In actual practice, most cases lie in between these two extremes and the surgeon must exercise his or her judgment as to the value of laser trabeculoplasty in the particular setting. As a general rule, potentially dangerous posttrabeculoplasty IOP elevation should be minimized by treating no more than half of the visible trabecular meshwork at a single laser session.
If medications and laser trabeculoplasty fail to control the IOP, filtration surgery is necessary.
What Particular Problems Does Filtration Surgery Pose in These Eyes?
Glaucoma filtration operations in eyes with primary angle closure can be exceedingly challenging and fraught with unique problems. In the characteristically small, hyperopic and deep-set eyes with primary angle closure, surgical exposure is usually far less than optimal. If the eye has recently had an acute attack of angle closure, visibility of anterior segment anatomy is often decreased by the presence of corneal edema. Also, conjunctival hyperemia predisposes to intraoperative bleeding, further compromising visibility. This is complicated by a small anterior segment in which to maneuver. In addition to these technical problems, there is an increased risk of intraoperative suprachoroidal hemorrhage and of postoperative malignant (ciliary block) glaucoma.
Future Considerations
The treatment of glaucoma in general, and therefore that of primary angle-closure glaucoma, will evolve and improve. As more glaucoma drugs have emerged, expanding the medical therapeutic options, the fraction of patients unable to use medications because of expense, inconvenience, and side effects has decreased. In particular, the continued development of aqueous suppressant medications increase the options for the ophthalmologist to lower the intraocular pressure even in the face of synechial angle closure. As the understanding of neuroprotectve medications grows, patients with primary angle closure, just like those with other forms of glaucoma, will benefit from medications that enhance the optic nerve’s ability to resist pressure-induced damage.
Through the years, instrumentation and techniques for laser iridectomy have continued to improve. Although Nd:YAG laser iridectomy is, at present, a wonderful procedure for patient and physician, iridectomy technology will doubtless become even better.
Relative pupillary block and the beneficial effect of laser iridectomy are very well understood. In contrast, plateau iris syndrome, despite recent progress, remains an enigma. A better understanding of the mechanics of plateau iris will yield a wider and more efficacious array of therapeutic options than laser gonioplasty and chronic miotics.
Finally, and perhaps most important, a better understanding and wider appreciation of the demographics of primary angle closure will increase awareness of the problem and lead to earlier detection, before permanent synechial angle closure and optic nerve damage occur.
References
4. Mapstone R: Mechanics of pupil block. Br J Ophthalmol 1968;52:19–25.
11. Drance SM: Angle closure glaucoma among Canadian Eskimos. Can J Ophthalmol Symposium 1973;8:252–254.
12. Cox JE: Angle closure glaucoma among the Alaskan Eskimos. Glaucoma 1984;6:135–137.
17. Quigley HA: Number of people with glaucoma worldwide. Br J Ophthalmol 1996;80:389–393.
23. Wand M: Argon laser gonioplasty for synechial angle closure. Arch Ophthalmol 1992;110:363–367.
24. Mapstone R: Provocative tests in closed angle glaucoma. Br J Ophthalmol 1976;60:115–119.
30. Reibaldi A: A new alpha blocking agent. Glaucoma 1984;3(6):255–257.
39. Quigley HA: Long term follow-up of laser iridotomy. Ophthalmology 1981;88:218–224.
43. Kolker AE: Techniques of argon laser iridectomy. Trans Am Ophthalmol Soc 1984;82:302–306.
44. Pollack IP: Use of argon laser energy to produce iridotomies. Ophthalmic Surg 1980;ll: 506–525.
46. Hoskins HD, Migliazzo CV: Laser iridectomy—a technique for blue irises. Ophthalmic Surg 1984;15:488–90.
48. Klapper RM: Q-switched neodymium:YAG laser iridotomy. Ophthalmology 1984;91:1017–1021.
50. Berger BB: Foveal photocoagulation from laser iridotomy. Ophthalmology 1984;91:1029–1033.
53. Mapstone R: The fellow eye. Br J Ophthalmol 1981;65:410–413.
56. Carpel EF, Brown JD: Permanent iridoplasty. Am J Ophthalmol 1983;96:113–114.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


