![]() 3
3 ![]()
Glaucoma Suspects
Kimberly S. Warren and Manijeh Contractor
Definition
How Are Glaucoma Suspects Defined?
Glaucoma suspects (or ocular hypertensives) may be defined as individuals with intraocular pressure (IOP) repeatedly above 21 mm Hg and/or appearance of the optic disc and/or nerve fiber layer that is indicative of glaucomatous optic nerve damage, but with normal visual fields. Appearance of the optic nerve head, which may lead to a suspicion for glaucoma, includes a large cup-disc ratio, narrowed disc rim, asymmetry of disc cupping between the two eyes, optic disc notching or hemorrhage, and peripapillary atrophy. These findings may be seen in conjunction with normal visual fields, adult onset, and normal gonioscopic examination. Known secondary causes of increased IOP or nerve damage, such as pigment dispersion, ocular trauma, and pseudoexfoliation, are excluded from the definition.
What Additional Factors Are Considered in the Definition of Ocular Hypertension?
There are some known risk factors that may make a patient “high risk” for developing glaucoma. These risk factors include advanced age, positive family history of glaucoma, myopia, black race, elevated IOP, and systemic diseases such as diabetes, cardiovascular disease, and hypertension.1–3 As the number of risk factors increases, the likelihood that an individual may develop glaucoma over a certain period of time also increases. Patients who are considered glaucoma suspects and demonstrate multiple risk factors must be carefully watched.
How Important Is IOP in Glaucoma Suspects?
The majority of patients with elevated IOPs do not develop glaucoma during their lifetimes. The higher the initial IOP, the more likely the individual may develop visual field loss. Armaly4 found that 6 to 12% of eyes with IOP in the range of 20 to 30 mm Hg on initial examination would develop visual field loss. This increased to 30% when the IOP was more than 30 mm Hg. Older patients also have a greater incidence of visual field loss.
There is still a lot of controversy regarding the use of term glaucoma suspect. Some ophthalmologists have strongly preferred the terms ocular hypertension, and incipient glaucoma. Approximately 5% of the general population have IOPs higher than 22 mm Hg and are known as ocular hypertensives. Although Armaly1 found in a 10-year follow-up study that 1.1% of ocular hypertensives individuals developed glaucoma, Lundburg et al5 found in a 20-year follow-up study that 34% of their subjects develop glaucoma. There is a definite and strong association between elevated IOP and glaucoma. Approximately 30% of the glaucoma patients have IOPs greater than 22 mm Hg.6–9 Therefore, patients with ocular hypertension are theoretically a heterogeneous group composed of preglaucoma and healthy subjects with IOP in the upper 5% of the normal range.
Epidemiology and Importance
Why Is Understanding of IOP Important in Studying Glaucoma Suspects?
As IOP is intimately related to glaucoma, it is essential to know its distribution and the factors that affect it. One of the first major population studies regarding the distribution of the IOP was undertaken by Leydhecker and Krieglstein10 in Germany. They measured IOP using Schiøtz tonometry on approximately 20,000 individuals, none of whom was known to have glaucoma at the time of examination. The authors found that the distribution of IOP in this population resembled a bell-shaped curve, but with skewing toward the higher levels. They calculated that the population’s average IOP was approximately 16 mm Hg, with a standard deviation of about 2.5 mm Hg.
IOPs over 21 mm Hg fell beyond two standard deviations from the mean, and therefore was considered abnormal. One should recognize that this abnormal level was reached solely by statistical methods. Eyes are different in their susceptibility to the effects of pressure. Some individuals develop glaucomatous damage at IOPs near the population mean, whereas others maintain normal optic nerve and visual functions for many years despite IOPs of 30 or even 40 mm Hg. Glaucoma is diagnosed only when there is detectable damage to the optic disc and/or visual fields.
Most studies have found that average IOP increases with age.11 Measurements of IOP at different times of the day often yield different readings, being higher in the morning than in the afternoon or later in the day. Pressures in some individuals may be somewhat higher in the winter than in the summer.12,13 There is also evidence that the IOP is slightly higher in women than in men after the age of 40.14 Patients with a family history of glaucoma,11,14 of African-American descent,1 and those with diabetes show a strong tendency toward higher mean pressures than the general population.
How Common Are Glaucoma Suspects Compared to Patients with Primary Open-Angle Glaucoma?
It is estimated that 2.25 million people in the United States over the age of 40 years have primary open-angle glaucoma (POAG),14 and approximately half are unaware of their disease despite demonstrable visual field loss.2 Another 10 million Americans are believed to have IOPs greater than 21 mm Hg; approximately 10% of these eyes may convert to POAG over the course of a decade.3
The concept of ocular hypertension is very important because although most glaucoma patients have elevated IOP, not all subjects with elevated IOP have glaucoma. Moreover, a majority of people with ocular hypertension may not develop glaucoma during their lifetimes. Ocular hypertension is present in up to 18% of people over 40 years of age of African-American descent compared with 13.6% of mixed race and only 4.6% of whites in the same age group.15
Who Is at Risk for Being a Glaucoma Suspect?
For many years, ophthalmologists have placed varying degrees of importance on the role of IOP in glaucoma. There is good evidence that IOP is a major risk factor for glaucomatous optic nerve head damage.16 Elevated IOP is present in a majority of glaucoma cases at initial screening.17,18 Population-based studies indicate only one-tenth or less of those with elevated IOP have glaucomatous visual field loss.18 Also, IOP varies in both glaucomatous and normal individuals over time. The proportion of glaucomatous subjects with elevated IOPs increases with time: 50% at screening, 75% at screening plus one follow-up, and 85% with screening and multiple follow-up checks.18 The hypothesis that elevated IOP is a major factor in chronic glaucomatous optic atrophy and that control of IOP usually has a favorable influence on its progression is widely accepted. One study noted that none of the study patients with IOP equal to or less than 16 mm Hg progressed, whereas all of the patients with pressure equal to or greater than 22 mm Hg worsened over a 4 to 11-year follow-up.19 Of patients with an IOP between 17 and 21 mm Hg, 50% progressed. Another study found that the number of subjects experiencing visual loss annually was twice as great when mean IOP was greater than 18 mm Hg, compared to IOP less than 18 mm Hg.20 The rate was four times greater when IOP measured more than 22 mm Hg. David and associates8 highlighted various differences between black and white individuals with ocular hypertension. They showed that 65.9% of black patients presented with IOPs higher than 26 mm Hg as compared to 26% of white patients. In both groups, the risk of glaucoma was directly related to the initial IOP. Black patients with ocular hypertension have a higher risk of developing glaucoma than white patients. Black patients with ocular hypertension were also 12.6 years younger than their white counterparts.
Higher rates for glaucoma have also been reported among some Caribbean populations. In the Barbados Eye Study (BES), a high prevalence of POAG was detected with increasing age.21 One in 11 persons older than 50 years had POAG. This estimate increased to one in nine at ages over 60 years and to one in six in those over 70 years. Although IOP may contribute to the high prevalence of POAG, genetic-environmental interactions also play an important role in its pathogenesis. This study also highlights the differences between ocular hypertension and POAG.22 Ocular hypertension in the black population of the BES was linked to the high prevalence of systemic hypertension and diabetes. Patients with large body sizes, measured by body mass index, demonstrated higher IOPs. Although obesity is related to hypertension and diabetes, the association between larger body size and IOP was found independently of these two variables. An association between obesity and IOP was also found in the Japanese population.23,24 Increased pigmentation was correlated with an elevated IOP in the BES. Gender association with open-angle glaucoma has also been shown in the Framingham Study.25 Men were more than twice as likely as women to have open angle glaucoma (2.5 % vs. 1.4 %). However, the results of a Swedish study were the opposite.26
A Greek study evaluated risk factors for conversion from ocular hypertension to POAG in 345 untreated glaucoma suspects.27 Twenty percent of the patients developed confirmed glaucoma. Family history, age greater than or equal to 60 years, axial myopia, and arterial hypertension were reported to be significant risk factors for visual field loss.
Are There Any Geographical Differences in the Distribution of Glaucoma Suspects?
Glaucoma is the second leading cause of blindness worldwide.9,28 In the year 2000, it is estimated that there may be approximately 66.8 million people globally with glaucoma and 6.7 million of these individuals may have bilateral blindness.28 As a result, glaucoma has been the subject of many population-based studies among major ethnic groups in the world.28–30
In the United States, POAG has been reported to affect between 1.5 and 2.1% of the population.6,18,25,31 Ocular hypertension occurs in 4 to 10% of the population over the age of 40.31 It is important to evaluate the ocular hypertensive group, as it is estimated that 10% of these individuals may eventually develop POAG.32
Mitchell and coworkers33 investigated the prevalence of open-angle glaucoma and ocular hypertension in an older Australian population. Open-angle glaucoma had a prevalence of 3.0%, whereas ocular hypertension was present in 3.7% of patients. The highest prevalence of 4.1% was found in the age group of 60 to 69 years and in individuals older than 80 years. The prevalence of glaucoma was higher in women after adjusting for age. But there was no sex difference in the age-adjusted prevalence of ocular hypertension.
Nearly half of the world’s estimated 5.1 million people who are blind because of glaucoma reside in East Asia.29 In an urban, South Indian population, prevalence of POAG was 4.1% and ocular hypertension was 30.8%.34 Interestingly, angle-closure glaucoma was reported to be 43.2% higher than both POAG and ocular hypertension combined.
A population-based, collaborative glaucoma survey was conducted in seven regions throughout Japan, during the years of 1988 and 1989. The findings at the time of screening included angle-closure glaucoma (34%), POAG (0.58%), low tension glaucoma (2.04%), and ocular hypertension (1.37%). The very high prevalence of low tension glaucoma and extremely low prevalence of ocular hypertension in the Japanese might reflect a racial peculiarity and the age-specific trend of the reduced IOP with advancing age. The prevalence of primary angle-closure glaucoma was found to be much higher in Japanese than in Caucasians, with a predilection for women. The Japanese also showed a progressive decrease in myopia with age.35
Diagnosis and Differential Diagnosis
How Is the Glaucoma Suspect Identified?
A careful history and examination are important in the diagnosis of ocular hypertension or glaucoma suspect (Fig. 3–1). A thorough history should be obtained. There are generally no reported symptoms, and an elevated IOP or a suspicious disc is found on routine eye examination. The patient’s age, race, and family history of glaucoma should be identified. The practitioner must inquire about past medical and ocular problems including congenital abnormalities, myopia, and systemic vascular diseases.
What Conditions Can Mimic Glaucomatous Nerves?
There are some individuals born with anomalous optic discs, which may mimic glaucoma type changes. These include a physiologically large cup-disc ratio, optic nerve asymmetry, and peripapillary atrophy. Patients with myopia often have tilted anomalous discs that can appear to have nerve loss. Systemic vascular diseases such as hypertension, cardiovascular disease, and atherosclerosis can also lead to loss of the nerve fiber layer and cause disc hemorrhage that can signify glaucomatous changes.36
What Findings in the Exam Lead to the Diagnosis of Glaucoma Suspect?
During ocular examination an IOP above 21 mm Hg, abnormal or suspicious optic disc findings, and multiple risk factors should make a clinician suspect glaucoma. As defined earlier in this chapter, suspicious optic nerve appearance includes an increased cup-to-disc ratio, asymmetry of the cups, notching, disc hemorrhage, and peripapillary atrophy. The diagnosis of a glaucoma suspect is made if gonioscopy and visual field analysis are within normal limits.
Are There Better Ways of Detecting Glaucoma Other Than Visual Fields and Optic Nerve Changes?
Nerve fiber layer defects have been shown to precede visual field defects in patients who progressed from a glaucoma suspect to POAG. In some studies the nerve fiber demonstrated changes 5 years before visual field changes.37,38 Studies by Quigley report that 40% of optic nerve fibers may be lost before there is a change noted on visual field testing.39 There have also been reports that scanning laser polarimetry shows a reduction in the nerve fiber layer levels when ocular hypertensive patients are compared with normals.40
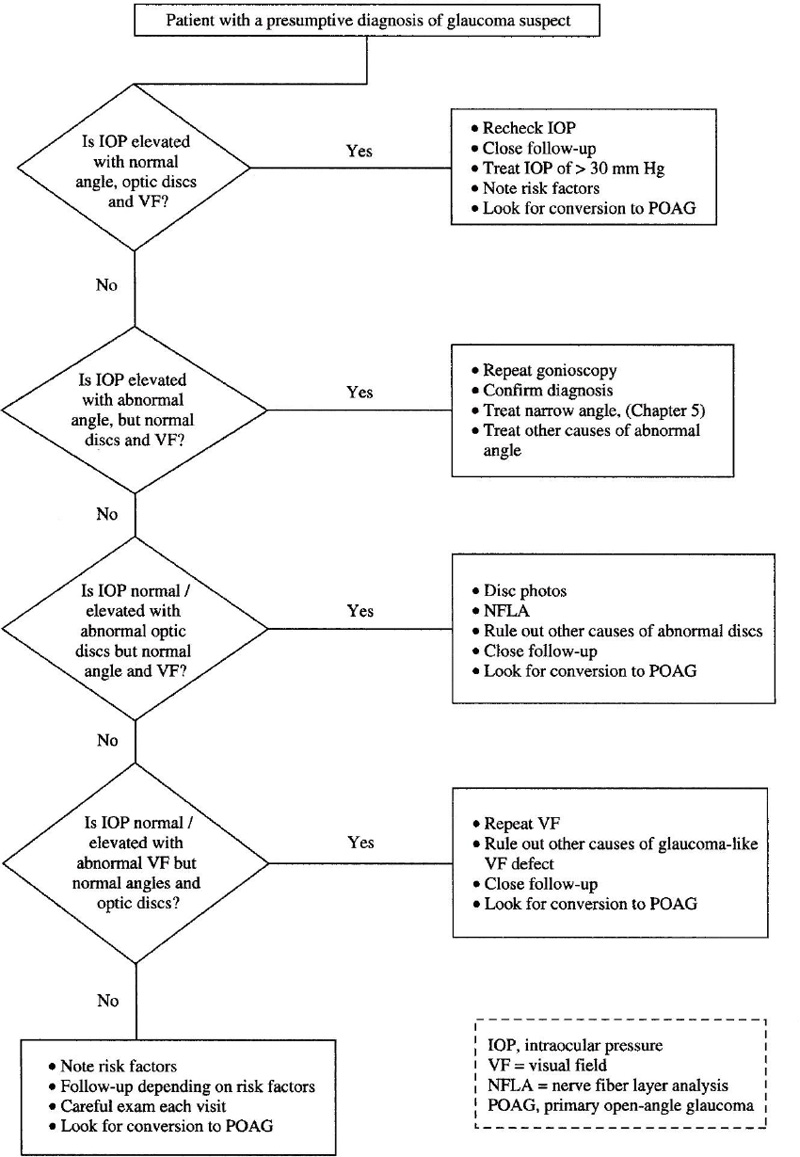
Figure 3–1. Algorithm for management of glaucoma suspects.
How Is Elevated IOP Related to Optic Nerve Damage?
Several hypotheses have been proposed in this regard. The first hypothesis (vascular theory) suggests that POAG represents a progressive anterior ischemic neuropathy, which is usually a result of elevated IOP. It is important to realize that perfusion of the optic nerve head is dependent on blood pressure at the level of the optic nerve, the capillary circulation in the optic nerve head, and the IOP itself. This explains why subjects differ in regard to the resistance of their optic nerve to increased IOP and why some individuals with microvascular diseases such as diabetes are more likely to develop glaucoma.
The second hypothesis, mechanical theory, suggests that POAG is due to a progressive optic neuropathy caused by the mechanical effect of IOP on the lamina cribrosa. Elevated IOP produces distortion and partial collapse of the lamina’s supportive structures, causing compression of the optic nerve fibers as they pass through. This will lead to the blockage of the axoplasmic flow and eventually destruction of the nerve fibers. Visual field loss would depend on the resistance of the lamina cribrosa to compression from the elevated IOP.
Experimental studies have shown that the holes and pores in the lamina cribrosa tend to be larger at the superior and inferior poles of the optic disc. Accordingly, the supporting structure of the lamina is less rigid in these areas and more likely to collapse when the IOP is elevated. This explains why progressive disc cupping usually precedes the development of visual field defects. Similarly, it may explain why young patients with less rigid laminar supporting tissue show rapid changes in the cupping when IOP is elevated, and why they show reversibility of cupping when IOP is normalized. Clinically, the initial damage is also seen at the upper or lower poles of the disc.
Is There Evidence of Abnormality in Blood Flow in Glaucoma Suspects?
In several studies, the abnormalities of the blood flow in POAG has been shown using color Doppler imaging,41,42 fluorescein angiography,43 laser Doppler flowmetry,44 and pulsatile ocular blood flow measurements 45
Other investigators have shown evidence of reduced blood flow at the level of the lamina cribrosa and temporal neuroretinal rim. Kerr and associates46 used scanning laser Doppler flowmetry images of the optic disc. Pulsatile ocular blood flow readings were performed on patients in the sitting, standing, and supine positions. The authors found significant reduction in the blood velocity, volume, and flow at the lamina cribrosa and temporal neuroretinal rim in glaucoma patients compared to patients with ocular hypertension. They found no difference between the groups when evaluating the nasal neuroretinal rim or nasal juxtapapillary retina. The ocular pulse amplitude, pulse volume, and pulsatile ocular blood flow were significantly lower in glaucoma compared to ocular hypertensives in the sitting and standing positions.
In 1973, Drance et al47 reported a “hypercoagulable state” theory in patients with normal pressure glaucoma. They showed that these patients had a greater tendency to develop thrombosis. Several other studies have also shown that patients with POAG, when compared with normal pressure glaucoma and a control group, had an elevated level of clotting cascade and fibrinolysis pathway (prothrombin fragments 1 + 2 and D-dimer).48
These findings give evidence of disturbance in ocular circulation in POAG. It is not clear if this is the primary cause of the disease or one of the complex collection of secondary changes that occur in glaucoma.
There are some published data relating to ocular blood flow in ocular hypertension. Some studies have shown no significant difference between normal and ocular hypertension, whereas others found evidence of impaired circulation in ocular hypertensives using fluorescein angiography49 The response of ocular blood flow to artificially elevated IOP in the acute situation has been studied in animal models.50 In normal human volunteers, blood flow circulation in the retina, choroid, and optic disc were studied with the use of suction cups to elevate IOP.51 The velocity of the blood flow, as measured with fluorescein angiography, was reduced at increased levels of IOP. The reduction in choroidal circulation was more marked than that in the retina. Differences in anatomic and physiologic characteristics of choroidal and retinal blood vessels appeared to account for this observation. IOP and age may alter the ocular blood flow in the absence of disease.52
Treatment and Management
How Often Should the Glaucoma Suspect Be Followed?
An ocular hypertensive or glaucoma suspect requires follow-up at regularly scheduled visits. The exams should include visual acuity, tonometry, optic nerve analysis, and periodic visual field testing. Baseline stereoscopic optic disc photos are helpful when analyzing the nerve for progressive changes characteristic of glaucoma. There has been recent advancement in the field of digital imaging that may be able to detect visual field loss prior to the conventional visual field testing. This method of nerve fiber layer analysis may help us detect patients who are destined to develop POAG at an earlier date and begin treatment.
When Should Medical Treatments Be Started in a Patient with Ocular Hypertension?
Therapy should be started if there is evidence of optic nerve or visual field changes consistent with early POAG. Some physicians may also treat based on a certain level of IOP regardless of normal appearing discs and visual fields. The level of ocular hypertension and the prevalence of optic nerve or visual field damage has been studied and correlated. A study by Strumberg53 showed that 29% of eyes with an IOP from 30 to 36 mm Hg showed some degree of measurable damage and 72% of eyes with IOP greater than 36 mm Hg showed damage. Stamper et al36 also found similar correlations with 28% of eyes with an IOP greater than 30 mm Hg showing damage. Pohjanpelto and Palva54 reported that 11% of eyes with IOP from 30 to 34 mm Hg and 27% of eyes with IOP 35 to 39 mm Hg showed changes consistent with POAG. Based on these studies, most physicians would treat ocular hypertension when the IOP reaches 30 mm Hg or greater consistently.
Do Other Factors Besides IOP Initiate Early Medical Treatment?
In addition to those with significantly elevated IOP (i.e., >30 mm Hg), patients with multiple risk factors should be considered for early treatment. For example, an African-American patient with a positive family history of glaucoma, who is also being treated for systemic hypertension, would be considered for early treatment even if the visual field tests were normal. Monocular patients should be watched very carefully, and initiating early treatment may be appropriate. A patient with unreliable visual fields or difficult follow-up exams should be considered for treatment as well. Patients who are anxious and very concerned about the possibility of progression to POAG should be counseled by the physician. Treatment and follow-up may be based on the physician and patient comfort levels. A patient with a previous vascular event in the fellow eye may also be considered for early therapy.
What Initial Medical Therapy Should Be Started?
In the treatment of ocular hypertension, it is best to begin with a monocular trial to ensure the efficacy of the drug. First-line therapy should be initiated after a thorough medical and ocular history to determine any contraindications to certain drugs. Depending on the patient, first-line therapy includes topical β-adrenergic antagonists, prostaglandin analogues, α-agonists, and topical carbonic anhydrase inhibitors. Systemic carbonic anhydrase inhibitors, miotics, argon laser trabeculoplasty, filtering, and tube-shunt procedures are routinely not indicated for the ocular hypertensive patient.
Do All Glaucoma Suspects Develop Glaucoma?
The majority of the individuals with ocular pressure greater than 21 mmHg did not develop visual field change with a follow-up of at least 5 years.55 Linner56 studied 10-year follow-ups of ocular hypertensive patients, and found that the mean value of pressure in those subjects examined at the beginning of the study and at 5- and 10-year intervals showed a statistically significant decrease. The identification of susceptible ocular hypertensive patients who may develop glaucoma is an unsolved clinical problem.
Future Considerations
What Are Some of the New Techniques Used to Analyze the Optic Nerve Head and the Nerve Fiber Layer?
There has been recent advancement in the technology used to analyze the optic nerve head and the nerve fiber layer. Some of these advancements include scanning laser tomography, scanning laser polarimetry, and optical coherence tomography (OCT). The Heidelberg retina tomograph (HRT) uses a diode laser that is projected onto the retina using a confocal system. The depth of the scanning rage is 0.5 to 4.0 mm. The instrument performs 32 consecutive scans and covers a rectangle of 10 × 10 degrees. According to a report by the American Academy of Ophthalmology (AAO),57 there are advantages and disadvantages of each of the above methods. The advantages of the HRT are that (1) images can be obtained in an undilated pupil, (2) it uses low light intensity, and (3) a real-time image can be obtained for immediate evaluation. Disadvantages of the HRT are the cost and that it requires a reference plane. The HRT targets both the optic nerve head and the nerve fiber layer for analysis.
The scanning laser polarimeter measures the nerve fiber layer by using a confocal scanning laser ophthalmoscope with an integrated polarimeter. The GDx Nerve Fiber Analyzer is an example of this technology. Scanning laser polarimetry measures the thickness of the retinal nerve fiber layer. The advantages outlined by the AAO57 include (1) quicker and more objective polarimetric reading than visual fields; (2) a greater sensitivity than the glaucoma hemifield test; (3) measurements are obtained without a reference plane and independent of magnification; and (4) it is independent of the optical resolution of the human eye. Some of the disadvantages are (1) other polarizing structures of the eye might interfere with retardation, and (2) peripapillary atrophy and chorioretinal scarring may also increase retardation. Scanning laser polarimetry targets analysis of the nerve fiber layer.
OCT is a high-resolution technique that is an optical analogue of ultrasound B-scan. It uses an 850-nm diode laser to obtain cross-sectional images of the posterior segment. The advantages of OCT include: (1) no reference plane is required, and (2) it is not affected by the refractive state of the eye. Disadvantages include: (1) cortical and posterior subcapsular cataracts may impair performance, and (2) it requires pupillary dilation. The target of this instrument in glaucoma evaluation is the nerve fiber layer. It also can be useful in diagnosing macular disorders and other retinal pathologies.
Can These New Techniques Differentiate Glaucomatous from Nonglaucomatous Eyes?
The techniques are relatively new; however, there has been some evidence to support their ability to detect glaucomatous changes. Mistlberger et al58 found that both HRT and OCT could differentiate glaucomatous from nonglaucomatous eyes. In the same study, however, the OCT showed no difference between normal and ocular hypertensive eyes. There have been other studies that claim HRT is able to demonstrate optic disc change before the development of field defects in a group of ocular hypertensives converting to early glaucoma.59 More studies and evaluations are needed to determine how best to use this new technology in the treatment of ocular hypertension.
Is There a Role for Neuroprotective Agents in Patients with Ocular Hypertension?
This is an interesting concept in the ocular hypertensive patient. Should patients be started on a neuroprotective agent to prevent the progression to POAG? If so, which patients should be started on neuroprotective agents and how should they be followed? Is nerve fiber layer analysis the best way to follow this category of patients? These are very important questions and more research needs to be done to see if certain medications can be used in the ocular hypertensive patients to protect them from future damage.
Acknowledgment
This work is supported in part by an unrestricted departmental research grant from Research to Prevent Blindness, Inc., New York, New York.
References
4. Armaly MF: Interpretation of the tonometry and ophthalmoscopy. Invest Ophthalmol 1972;11:75–79.
17. Sommer A: Intraocular pressure and glaucoma. Am J Ophthalmol 1989;107:186–188.
24. Shiose Y, Kawase Y: A new approach to stratified normal intraocular pressure in a general population. Am J Ophthalmol 1986;101:714–721.
28. Quigley HA: Number of people with glaucoma worldwide. Br J Ophthalmol 1996;80:389–393.
30. Thylefors B, Negrel AD: The global impact of glaucoma. Bull WHO 1994;72:323–326.
32. Kass M: When to treat ocular hypertension. Surv Ophthalmol 1983;28:229–232.
53. Stromberg U: Ocular hypertension. Acta Ophthalmol Scand Suppl 1962;69:7.
56. Linner E: Ocular hypertension: I. The clinical course during ten years without therapy: aqueous humor dynamics. Acta Ophthalmol 1976.54;707–720.
59. Kamal DS, Viswanathan AC, Garway-Heath DF, et al: Detection of optic disc change with the Heidelberg retinal tomograph before confirmed visual field change in ocular hypertensives converting to early glaucoma. Br J Ophthalmol 1999;83:290–294.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


