Essentials of Diagnosis
General Considerations
The frontal sinus begins as an outgrowth of the nasal chamber in utero but does not begin to invade the vertical portion of the frontal bone until the 4th year of life. The sinus attains adult configuration at age 15 and typically reaches adult size by age 20. A variable structure, the frontal sinuses are typically asymmetric and may be unilateral (10%) or absent altogether (5%).
The anterior wall of the fully developed frontal sinus is a thick bony arch that can withstand between 800 and 2200 pounds of force. The force required to fracture this robust structure often leads to multiple injuries; therefore, a full trauma workup of all patients with frontal sinus fractures is paramount. As with all trauma patients, the airway, circulatory system, and other organ systems must be evaluated upon arrival. All patients require ophthalmologic and neurologic examination as well as radiographic and clinical examination of the cervical spine. Intracranial injury (40–50%) and other facial fractures (75–95%) are among the most commonly associated injuries in patients with frontal sinus fractures.
Pathogenesis
Motor vehicle accidents are the most common mechanism of injury for patients with frontal sinus fractures, accounting for 60–70% of all frontal sinus fractures. Assault typically requires the use of a blunt object to fracture the frontal sinus; fists alone rarely generate sufficient force. Other mechanisms of injury include industrial accidents, recreational accidents, and gunshot wounds. Young men in their third decade of life are most at risk for frontal sinus fracture. In one study, 30% of patients with frontal sinus fractures had blood alcohol levels over the legal limit or positive urine toxicology screens.
Prevention
The use of seatbelts and airbags for passengers and drivers can decrease the incidence of severe head trauma and frontal sinus fractures. Patients in automobile accidents in which airbags are deployed have a significant decrease in the number of facial fractures. Estimates are that only 15% of young patients with frontal sinus fractures resulting from automobile accidents were wearing a seatbelt; less than 10% of patients with frontal sinus fractures from motorcycle accidents were wearing a helmet. The use of helmets with motorcycles, with bicycles, at appropriate sporting events, and in industrial situations also can protect the frontal sinuses.
Clinical Findings
Most patients lose consciousness with the force required to sustain a frontal sinus fracture; estimates are that 25% of patients remain conscious throughout the injury, 50% regain consciousness within the first 4 hours after injury, and the final fourth develop prolonged unconsciousness.
Patients who are conscious at the time of the evaluation typically report frontal pain. Forehead lacerations occur in approximately 80% of frontal sinus fractures. Other less common signs on physical examination include the following: frontal numbness; palpable step-offs or crepitus; cerebrospinal fluid (CSF) leak; exposed bone; exposed brain; and ocular abnormalities, including diplopia, ophthalmoplegia, and decreased visual acuity. Between 5% and 10% of patients have no significant physical findings on examination.
Associated injuries are the rule with frontal sinus fractures. Other facial fractures occur in up to 95% of patients; bones of the orbit and paranasal sinuses are the most commonly involved. Intracranial injuries are seen in approximately 50% of patients; of these types of injuries, frontal contusions are the most common.
CT scanning is the imaging examination of choice for the evaluation of frontal sinus fractures. Clinicians looking for intracranial pathology after head trauma order CT scans of the head and often discover fractures.
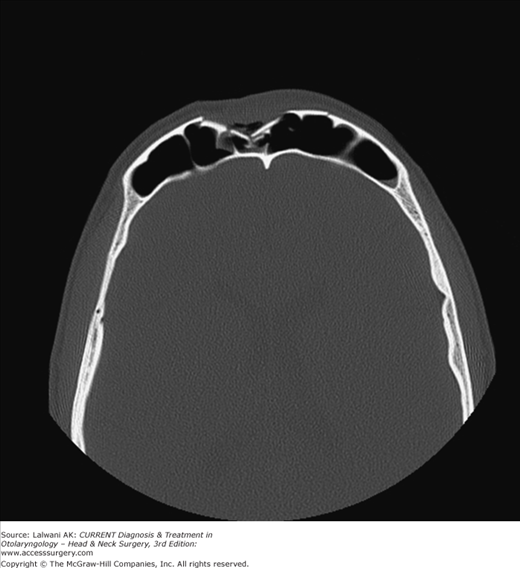
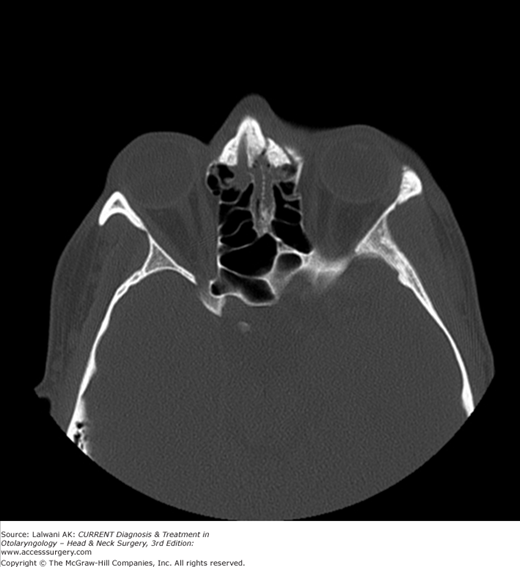
When evaluating the extent of injury and determining the operative plan for frontal sinus fractures, thin-cut axial and coronal facial CT scans are preferable to thicker-cut 5–10 mm head CT scans. Presently, fine-cut axial CT scans with coronal and saggital reconstruction are typically used for the evaluation of frontal sinus fractures. Slice thickness of 0.625 mm is ideal, although a thickness of up to 2 mm is typically adequate. Direct coronal views are less amenable to axial and saggital reconstruction and are often contraindicated in patients with frontal sinus fracture related to possible cervical spine injury and issues related to other associated injuries. Soft tissue windows should be used to evaluate intracranial and orbital injuries, which are often seen in patients with frontal sinus trauma. Many patients with associated injuries do not tolerate direct coronal images. Figures 16–1 and 16–2 are axial images of a patient with a depressed anterior table frontal sinus fracture and frontonasal recess injury, respectively.
The role of plain X-ray films in the evaluation of frontal sinus fractures is limited. In patients with nonoperative fractures and fluid in their frontal sinuses, serial Caldwell views may be used to monitor resolution of the fluid, insuring patency of the frontonasal recess.
Differential Diagnosis
Frontal sinus fractures should be distinguished from both simple forehead contusions and lacerations. Frontal bone fractures without the involvement of the frontal sinus may be mistaken for frontal sinus fractures. CT scans distinguish between these possibilities with ease.
Determining the extent of a fracture is more difficult than determining whether a frontal sinus fracture is present. Involvement of both the posterior table of the frontal sinus and the frontonasal recess is critical in determining the treatment of the fracture. Anterior table fractures are often easily identified on axial CT scans; however, because of the thin nature of the posterior table, nondisplaced posterior table fractures can be less obvious. A high index of suspicion for posterior table fractures is necessary in all patients. Pneumocephalus on the CT scan may provide a clue that the posterior table has been violated, but pneumocephalus also may come from fractures of the ethmoid bones or other aerated regions of the skull.



