was graduated from the Philipps University Medical School in Marburg in 2010 and received his doctoral degree from the Philipps University in the same year. Since 2011 he is an ophthalmic resident at the University Eye Hospital in Bochum. His research interests are focused on laser-assisted cataract surgery, refractive surgery, and new intraocular lens technologies.

is an ophthalmologist and historian. He is working for a medical publisher in Germany and is a regular contributor to a number of journals. He has written about a dozen books on his favorite subject (besides ophthalmology), American History.

12.1 Precise and Safe: Capsulotomy and Lens Fragmentation
When, 260 years ago, Jacques Daviel stated his aim “…to entirely loosen the cataract and facilitate its issue,” he probably had a technique in mind that enabled the surgeon to operate fast, with short, precise cuts and with a high degree of safety and postoperative vision for his patients. Modern cataract surgery—which is almost always refractive surgery as well—has come closer to perfection than this pioneer in our field (who lived from 1696 until 1762) could have ever imagined. In fact, cataract surgeons in this day and age are in a position envied by colleagues in most other medical disciplines: not only will the organ in the cataract surgeon’s crosshairs enjoy a better function than preoperatively—in some cases (one might think of an almost lifelong myopia that is corrected by an IOL) it might work better than ever before in the patient’s life, without refractive error, astigmatism, and, of course, lens opacity.
The introduction of the femtosecond laser into cataract surgery, after its successful debut in refractive surgery, is part of this success story—and gives reason to expect further progress and unequaled patient satisfaction, particularly in patients with premium IOL implantation. A variety of femtosecond laser platforms have been introduced into cataract surgery, among those approved by the FDA are LensAR (LensAR Inc, Winter Park, FL), LenSx (Alcon LenSx Inc, Fort Worth, TX), Catalys (Abbott Medical Optics, Abbott Paark, Illinois, USA) and Victus (Bauch & Lomb/Technolas Perfect Vision GmbH, Munich, Germany) [1].
Our research in the field of femtosecond laser-assisted cataract surgery is based on our clinical experience with the Catalys system. Unique to that platform is a liquid optics interface docking system that includes a fluid-filled suction ring and a non-applanating disposable lens (Fig. 12.1). This docking system is engaged by the surgeon while he or she controls the patient’s chair using video imaging for alignment. Once suction is confirmed, the system automatically measures the dimensions of the anterior chamber and the lens with an integrated three-dimensional spectral-domain optical coherence tomography device. This SD-OCT identifies the ocular surfaces and creates laser exclusion zones (Fig. 12.2). The results are displayed to the surgeon for verification. At this point, the surgeon has the option of using the videographic user interface to reposition and/or redesign the corneal incisions, the capsulotomy, and lens fragmentation procedures. The advantages of the non-applanating Liquid Optic interface are a relatively mild rise in intraocular pressure (see below), a better optical quality for the surgeon, almost no corneal folds (Fig. 12.3), and fewer cosmetically challenging complications like subconjunctival hemorrhages—there is hardly any sign of ocular discomfort like redness in most eyes even on the day of surgery.
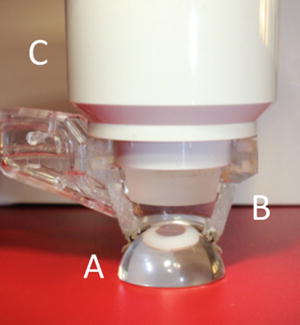
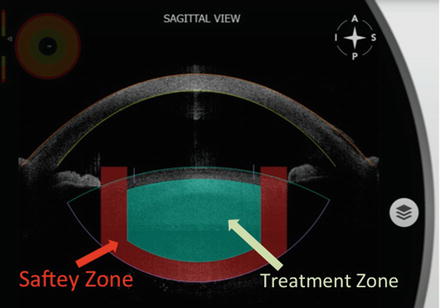
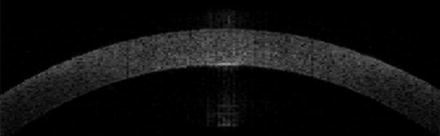
Fig. 12.1
Non-applanating and fluid-filled patient interface. (a) Eye. (b) Cut by half fluid-filled suction ring. (c) Non-applanating disposable lens
Fig. 12.2
Automatic 3D spectral-domain optical coherence tomography with automatic ocular surface identification and laser exclusion zones
Fig. 12.3
3D spectral-domain optical coherence tomography of the cornea without folds using a non-applanating fluid-filled patient interface
The attempted capsulotomy diameter usually is 5.0 mm (4 μJ pulse energy). The lens-softening pattern applied by the femtosecond laser is standardized; the grid size is normally either 350 or 500 μm (Fig. 12.4). The femtosecond laser pulses are focused starting at the predefined distance from the posterior capsule (posterior safety margin) and moved in the anterior direction through the crystalline lens (Table 12.1 and Fig. 12.2). The laser does not create planes across the lens in the coronal plane. The gas released from cavitation bubbles creates a pneumodissection effect that further separates the crystalline lens along the natural lamellar structure, reducing the need for hydrodissection and most often creating cubes of softened lens. However, the laser itself does not cut cubes but rather slices the lens.
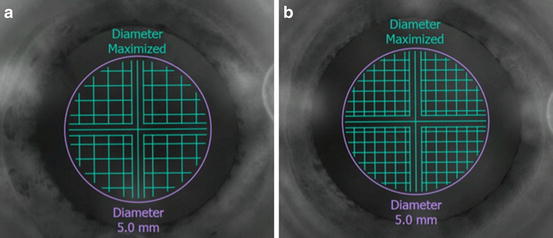
Fig. 12.4
500 (a) and 350 (b) μm grid pattern
Ultrasound phacoemulsification is performed in our clinic on the same operating chair, without moving or walking the patient through the operating room. Preparing the patient for phacoemulsification and IOL implantation with the femtosecond laser results in a considerable reduction of effective phacoemulsification time. In two groups of 80 patients each, one group receiving a 350 μm grid pattern and the other a 500 μm grid pattern, the mean absolute phacoemulsification time was 0.03 and 0.21 s, respectively. Cataract surgeons have for almost two decades evaluated ways to reduce the amount of ultrasound energy the ocular structures are exposed to. The femtosecond laser has achieved this goal most convincingly. There is a plethora of benefits for the patient: less energy delivered to the eye may be associated with an earlier improvement in postoperative visual acuity as a result of less endothelial cell loss and corneal edema and less anterior chamber cells and flare caused by alteration of the blood–aqueous barrier. The corneal swelling in the early postoperative period is less pronounced after femtosecond laser application than after conventional phacoemulsification; Takacs et al. described a significantly higher central corneal thickness after phacoemulsification alone (607 μm on average) than after pretreatment with the femtosecond laser (580 μm) in groups of 38 eyes each [2]. Less phacoemulsification energy usually means a faster and safer visual rehabilitation after cataract surgery [3].
12.2 Clinical Pearls
12.2.1 Three-Step Regimen for Femtosecond-Assisted Cataract Surgery in Eyes with Small Preoperative Pupils
There is no doubt that a large pupil is most welcome to any cataract surgeon, no matter which technique is being used. This applies to femtosecond laser cataract surgery as well. A dilated pupil enables the laser system to provide an accurate image of the anterior segment, which allows planning the treatment preoperatively. A large pupil also allows clear visualization of the anterior segment by the surgeon during the laser application. Furthermore, femtosecond lens fragmentation is more effective in eyes with large pupils, decreasing ultrasound phacoemulsification application during removal of the nucleus.
Unfortunately, it is not always this way. Among the first 850 eyes we performed surgery upon using the Catalys femtosecond laser and using an all-comers approach, there were 40 eyes (4.7 %) with a pupil dilatation less than 5.5 mm after routine preoperative dilation. The mean pupil diameter achieved after preoperative topical dilation in this group was 4.4 ± 0.42 mm (median 4.5 mm; minimum 3.2 mm, maximum 4.9 mm). The most frequent comorbidities of the non-dilating pupils were a pseudoexfoliation of the lens capsule (30.0 %) and an intraoperative floppy iris syndrome (12.5 %). Three eyes had glaucoma (10 %), two eyes (6.7 %) suffered from corneal guttae, and two eyes (6.7 %) had a history of blunt ocular trauma.
To Dilate These Pupils, a Three-Step Approach Proved Helpful
(a)
Intracameral administration of a 0.1 % epinephrine solution
(b)
Additional viscomydriasis with Healon GV(AMO, Santa Ana, California, USA)
(c)
Implantation of a Malyugin ring (7 mm, MicroSurgical Technology, Redmond, Washington) (Fig. 12.5)
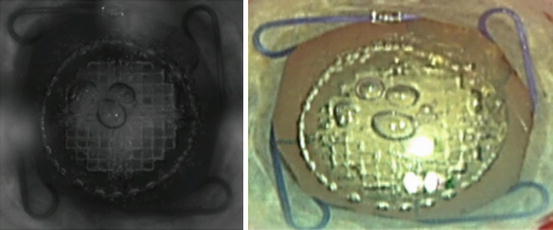
Fig. 12.5
Femtosecond laser-assisted cataract surgery with Malyugin ring in place
The application of intracameral epinephrine alone was sufficient in 7 %; in 25 % additional viscomydriasis was necessary. The implantation of a Malyugin ring was performed in 68 %. In the majority of cases with an implanted Malyugin ring, the device was removed after the implantation of the IOL using the ophthalmic viscosurgical device (OVD) to protect corneal endothelium. The trailing eyelet was disengaged first using the Frankfurt iris manipulator (Geuder, Germany). The inserter was placed slightly at the side of the eyelet, but over the ring, and then turned in a way that the hook was over the entire eyelet. Engaged with the eyelet, it was pulled back into the bimanual inserter and out of the anterior chamber. OVD removal was performed using 20 G irrigation–aspiration handpieces (Geuder, Germany).
Using this three-step approach, a mean pupil diameter of 5.8 ± 0.36 mm (median 5.8 mm; minimum 5.0 mm, maximum 6.3 mm) was achieved. The capsulotomy diameter on the Catalys instrument was set for 5.0 mm; the resulting capsulotomy diameter was a mean of 4.8 ± 0.18 mm (median 4.9 mm; minimum 4.5 mm, maximum 5.0 mm). In not a single eye did severe intraoperative complications occur. The OCT scanning was not compromised in any case and the posterior capsule had been detected correctly. Five capsulotomies showed fine tongue-like lesions. All of the capsule discs could be pulled out with the Koch microforceps (Geuder, Germany) without any further manipulation of the capsulotomy. No capsular tears were observed. One eye had a duplicate anterior capsule and it was necessary to repeat the femtosecond laser capsulotomy procedure to achieve a complete opening of both layers of the capsule. In all cases that were treated with a Malyugin ring, the anterior chamber was stable during every step of the femtosecond laser-assisted procedure. No redocking of the fixation cone on the eye had to be performed.
With the disposable liquid optics interface of the Catalys system which does not distort the cornea and raises the intraocular pressure only minimally [4], the surgeon has the means to separate surgical steps changing from laser capsulotomy and lens fragmentation to manual steps such as the insertion of a Malyugin ring and back to laser treatment easily. To create a well-sized and shaped capsulotomy in “small pupil” cases, the use of a femtosecond laser can be a great advantage [5, 6].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


