Eye Movements and Positions
Joseph L. Demer
Support: Supported by U.S. Public Health Service, National Eye Institute: grant EY-08313 and core grant EY-00331. J. Demer is Leonard Apt Professor of Ophthalmology.
Introduction
Any mobile object has six degrees of freedom: linear motion, also called translation, of its center in three orthogonal directions, and rotation about three orthogonal axes. For the eye, the translational movements may be conveniently described as anteroposterior, corresponding to proptosis versus enophthalmos; superior to inferior, corresponding to the vertical direction of hypoglobus; and mediolateral, corresponding to the horizontal direction of hypertelorism (Fig. 2.1). Ocular rotations may be conveniently described as horizontal rotations about a vertical axis corresponding to medial and lateral gaze; vertical rotations about a horizontal axis corresponding to upward and downward gaze; and torsional rotations about the line of sight. Although these designations of the translational and rotational motions of the eye seem natural and intuitive, nothing is actually unique about the designations. The foregoing coordinate systems are arbitrary conveniences of nomenclature. Other choices of coordinate systems are equally valid in the kinematic sense. It is worth briefly considering some kinematic issues that can influence the clinical description of eye movements and positions.
 Figure 2.1. A common coordinate system for translation and rotation of the eye. |
Translations of any object are commutative in the mathematical sense.1 Commutativity implies that the outcome of an operation is independent of the sequence of steps. For example, the mathematical operation of addition is commutative. The sum of 2 plus 3 is equal to 3 plus 2, for example. In the same sense, horizontal, vertical, and anteroposterior translations of the eye can be combined in any sequence with identical result. Ocular rotations are a different matter. The final orientation of the eye depends on the sequence of otherwise identical rotations of the eye in the three degrees of rotational freedom, in whatever coordinate system they are defined. Consider the following example. A 90 degree horizontal rotation to the right followed by a 90 degree vertical rotation upward results in an upward gaze direction; conversely, a 90 degree vertical rotation upward followed by a 90 degree horizontal rotation to the right results in a rightward gaze direction. The effect of noncommutativity of the rotational sequence is not limited to large eye rotations. Noncommutativity results is smaller differences for smaller angles, but differences that would nevertheless prohibit coordinated binocular alignment if the two eyes followed different sequences of otherwise equal rotations.
The problem of noncommutativity of sequential rotations is not prohibitive for either the physiology of eye movements or for those who measure eye movements. Discussed below is how the ocular motor system avoids the problem. When eye rotations are accurately measured, however, the rotational sequence must be specified. It is critical to note that for each sequence, each rotation shifts the entire coordinate system for the eye, so that the orientations of subsequent rotational axes are rotated by preceding rotations in the manner of a gimbal.2 Probably the most common sequence of rotations is the Fick sequence: first, horizontal rotation about a vertical axis; second, vertical rotation about a horizontal axis; and third, rotation about the line of sight. Another common rotational sequence, named for Helmholtz, is particularly useful for study of horizontal vergence: first, vertical rotation about a horizontal axis; second, horizontal rotation about a vertical axis; and third, torsional rotation about the line of sight. Other rotational sequences are possible, but are not typically used because as a practical matter it is very complicated to introduce torsion as one of the first or second rotations. There is no avoiding the issue that the numerical values (horizontal, vertical, torsional) of the angles describing the same final eye orientation depend on the sequence of rotations chosen.
The foregoing discussion of rotational commutativity would seemingly make ocular motility overwhelmingly complicated. Both the brain and the clinician are able to exploit simplifications that facilitate the neural command and measurement of eye rotations. In both cases, eye rotations having small to moderate angles may be reasonably approximated as consisting of independent horizontal and vertical components that do not interact. For clinical measurement purposes, this approximation works reasonably well as long as large horizontal and vertical eye rotations, or binocular misalignments, do not occur simultaneously. The clinician should always bear in mind, however, that it is only an approximation to regard horizontal and vertical angle measurements as mutually independent.
Clinical Nosology of Ocular Kinematics
Duction
The term duction refers to the rotation of one eye considered independently of its fellow. A prefix is attached to this word to indicate the direction in which the eye is rotated (Fig. 2.2). The muscle actions described below are as observed in a clinical coordinate reference, with horizontal movements described for rotations about a vertical axis in the head; vertical eye movements described for rotations about a horizontal axis in the head; and torsional movements described for torsional movements around the line of sight. The reader should be aware that, whereas this coordinate system is adequate for clinical purposes, it is only an approximation of precise ocular kinematics for reasons that include neglect of the issue of noncommutativity.
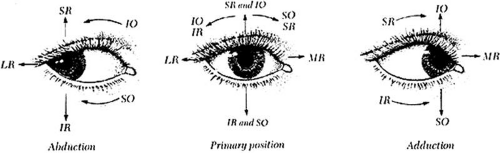 Figure 2.2. Ductions and their principal agonist extraocular muscles when pulley positions are normal. Horizontal ductions (adduction and abduction) are produced mainly by the medial rectus (MR) and lateral rectus (LR) muscles. Vertical ductions and cycloductions result mainly from combined contractions of the vertical rectus and oblique muscles, but may also result from oblique actions of horizontal rectus muscles under certain conditions. Combined contractions of the superior rectus (SR) and inferior oblique (I0) muscles produce most supraduction; combined contractions of the inferior rectus (IR) and superior oblique (SO) muscles produce most infraduction. Incycloduction is mainly caused by combined SO and SR contractions, and excycloduction is mainly caused by combined IO and IR contractions. In each case, however, abnormal muscle pulling directions caused by heterotopic pulleys may permit any rectus muscle to have horizontal, vertical, and torsional effects. |
Adduction
Adduction is a horizontal rotation about a vertical axis shifting gaze medially. It is mainly accomplished by contraction of the medial rectus muscle and relaxation of the lateral rectus muscle. The vertical rectus muscles may also produce adduction (e.g., when in central gaze their pulleys and scleral insertions are shifted nasally). For example, nasal displacement of the vertical rectus pulleys and insertions on the sclera can produce significant adducting force that can be exploited surgically to treat medial rectus paralysis.
Abduction
Abduction is a horizontal rotation about a vertical axis shifting gaze laterally. It is mainly accomplished by contraction of the lateral rectus muscle and relaxation of the medial rectus muscle. A small amount of secondary abduction is accomplished by contraction of the oblique muscles—in up gaze by the inferior oblique muscle, and in down gaze by the superior oblique muscle. The vertical rectus muscles can also produce abduction (e.g., when in central gaze their pulleys and scleral insertions are shifted temporally). For example, temporal displacement of the vertical rectus pulleys and insertions on the sclera can produce significant abducting force that can be exploited surgically to treat lateral rectus paralysis.
Supraduction
Supraduction (sursumduction) is an upward vertical rotation (elevation) about a horizontal axis. Supraduction results from combined contraction of the superior rectus and inferior oblique muscles and the combined relaxation of the inferior rectus and superior oblique muscles. The inferior oblique muscle produces greater supraduction in adduction than in abduction, so that supraduction in adduction can be regarded as a diagnostic position reflecting inferior oblique activity in some circumstances. Note, however, that other muscles, including the superior rectus and medial rectus, can produce supraduction in adduction. Consequently, this gaze position is not a specific indicator of inferior oblique muscle contractility.
Infraduction
Infraduction (deorsumduction) is a downward vertical rotation (depression) about a horizontal axis. Infraduction results from combined contraction of the inferior rectus and superior oblique muscles. The superior oblique muscle is active in downward gaze across the horizontal range, but the action of the superior oblique muscle depends on the geometry of its path from the rigid trochlea to the scleral insertion. Thus, in abduction, the superior oblique muscle is mainly an incycloducctor of the eye, and in adduction the superior oblique muscle is mainly an infraductor. The inferior rectus muscle is the main infraductor of the eye. In adduction, however, the superior oblique muscle contributes sufficient infraduction that this gaze position may be regarded as a diagnostic position reflecting superior oblique activity in some circumstances. Note, however, that other muscles, including the inferior rectus and sometimes the medial rectus, can produce infraduction in adduction. Consequently, this gaze position is not a specific indicator of superior oblique muscle contractility.
Incycloduction
Incycloduction (intorsion) is a rotation of the eye about the line of sight that displaces the superior pole of the eye medially. Incycloduction is mainly the result of the combined contraction of the superior oblique and superior rectus muscles, and the combined relaxation of the inferior oblique and inferior rectus muscles. As the eye moves into an abducted position, however, the superior oblique muscle becomes the prime incycloductor, and in adduction, the superior rectus muscle is the principal incycloductor. The rectus muscles can also produce incycloduction (e.g., when in central gaze their pulleys and scleral insertions are not both aligned anteroposteriorly). For example, superior displacement of the lateral rectus pulley, inferior displacement of the lateral rectus insertion on the sclera, or both, will result in incycloduction as the lateral rectus muscle contracts. Analogous alterations of any of the rectus pulleys or scleral insertions can similarly product incycloduction.
Excycloduction
Excycloduction (extorsion) is rotation of the eye about the line of sight that displaces the superior pole of the eye laterally. Excycloduction is mainly the result of the combined contraction of the inferior oblique and inferior rectus muscles and the combined relaxation of the superior oblique and superior rectus muscles. The rectus muscles can also produce excycloduction (e.g., when in central gaze their pulleys and scleral insertions are not both aligned anteroposteriorly). For example, inferior displacement of the lateral rectus pulley, superior displacement of the lateral rectus insertion on the sclera, or both will result in excycloduction as the lateral rectus muscle contracts. Analogous alterations of any of the rectus pulleys or scleral insertions can similarly product excycloduction.
Version
Version refers to simultaneous movement of both eyes in the same direction; a prefix indicates the direction of the conjugate movement. The muscles in each eye that are the prime movers undergo graded contractions in accord with Hering’s Law of innervation, and for each contracting muscle, there is normally a corresponding relaxation of an antagonist (Sherrington’s Law). Hering’s Law states that the gaze effort command to each eye is the same; if only one eye is able to see the target, the fellow eye will receive the same command. The complete range of versions, indicating only the contracting muscles, is shown in Figure 2.3.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


