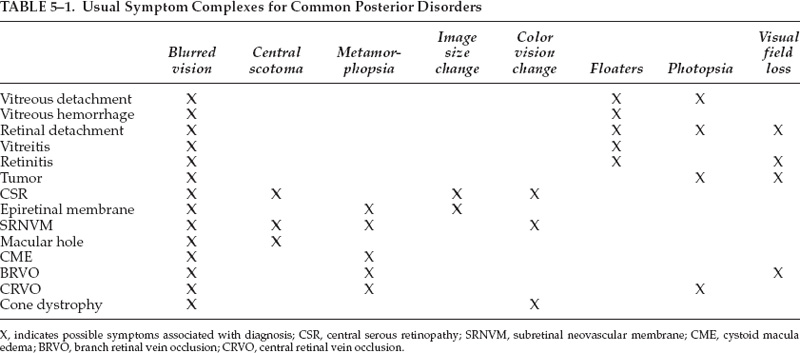
5 Almost every patient evaluation begins with a chief complaint or the patient’s statement of the predominant symptom. In some cases, a single symptom will be almost pathognomonic of a particular entity. More often, the complaint will be associated with other symptoms, and the pattern will be useful in constructing a differential diagnosis. In a large number of retinal diseases, the symptom complex and a complete ocular examination will be enough to establish the diagnosis. For the retina patient, the complete examination includes distance and near vision, refraction, external examination, pupil examination, confrontation visual fields, slit-lamp examination, intraocular pressure, biomicroscopic study of the vitreous and retina, and indirect ophthalmoscopy, usually with scleral depression. Amsler grid is often useful in localizing disease to the macula. Fluorescein angiography is commonly used to document the degree of disease, to elucidate a diagnosis, and to guide therapy. The study of the posterior segment by ultrasonography is helpful when the media are obscured either by anterior segment disease or vitreous hemorrhage or when a mass is identified in the fundus. Visual fields, color vision testing, optical coherence tomography, and the retina thickness analyzer all have their place in studying more complex problems. The vast majority of retinal diagnoses can be established from examination alone. Nevertheless, taking a history is important for a number of reasons. First, it helps to establish a differential diagnosis and therefore focus the examination to distinguish between entities. Second, it is important to understand the patient’s concerns. From the history, the physician should not only elucidate details of the symptomatology but should listen sympathetically so that he or she understands the fears and anxieties caused by the symptoms. The patient will have certain expectations of the encounter with the physician that also can be extracted from the conversation. The choice of terms in explaining the disease can give the physician clues about the patient’s level of knowledge and sophistication regarding ocular problems. The interchange between the physician and patient also may be valuable to understanding what coping mechanisms the patient may be using to deal with these new complaints. Finally, a careful history will allow the physician to predict accurately the examination findings in many cases. One of the most important questions to ask about a symptom is the relative intensity. Is the scotoma complete or only relative? Is the visual loss mild or severe? If pain is involved, for example, is it slightly annoying or is it disabling? Current Medicare guidelines mandate that pain be considered one of the key pieces of information elicited in every examination. The next pertinent question is, How long has the symptom been present? For visual symptoms, the answer to this question is often vague. When there is a definite onset to the symptom (“I was sitting at the table, and I began to notice floaters”), it is helpful in pinpointing the duration of the problem. In other cases, the symptom may seem acute to the patient, but the disease process may be well established. A classic example of this phenomenon is the patient who wakes up to look at the clock and notes that because one eye is occluded by the pillow, he or she cannot see the clock with the other eye. In this situation, the visual loss may have been present for a long time before its discovery. An additional important question is, Is the symptom stable or becoming worse? Some disorders, such as macular pucker, have an acute onset and often remain stable. Others, however, are slowly progressive over months to years. In trying to establish duration, it may be helpful to ask the patient if he or she can recall whether the symptom was present at some specific time, such as a past holiday, or if the symptom might have been present 1 year or 2 years or 5 years previously. Vitreous floaters from a posterior vitreous detachment follow another pattern; they appear suddenly and fade over time. Further, the following question is also important: Is the symptom intermittent or constant? Intermittent symptoms may suggest vascular phenomena, acute variations in intraocular pressure, or symptoms associated with increased intracranial pressure. Often, however, intermittent symptoms may be attributed to changes in ambient lighting or to difficulties with specific visual tasks. A patient may present with a single symptom, but more often there are multiple interrelated symptoms. Table 5–1 lists some common retinal diagnoses with their usual associated symptoms. Blurred vision may be a symptom of anterior or posterior segment disease. Symptoms of itching (allergy), exudate, dry eyes, tearing, and foreign-body sensation most often point toward external ocular disease. Many patients describe these along with complaints more suggestive of retinal disease. Once the posterior diagnosis is established, the patient should be reassured that the anterior symptoms do not relate to the posterior problem. Monocular diplopia and triplopia most often are encountered with a particular set of glasses or problems with the crystalline lens, such as juvenile nuclear sclerosis. Floaters are the hallmark of disease in the vitreous. Floaters are usually caused by small bits of collagen in the vitreous cavity, by inflammatory cells in the vitreous, or by vitreous hemorrhage (Table 5–2).
Expanding on the Primary Complaint to Get to the Diagnosis
Symptoms
Why Obtain an Ophthalmic History?
What General Questions Should Be Asked about Symptoms?
Symptom Complexes
Which Visual Symptoms Suggest Anterior Segment Disease?
Which Symptoms Suggest Vitreous Disease?
| Retinal breaks |
| Subretinal hemorrhage |
| Trauma |
| Neovascularization |
| Diabetic retinopathy |
| Occlusive diseases |
| Branch retinal vein occlusion (BRVO) |
| Central retinal vein occlusion (CRVO) |
| Sickle cell retinopathy |
| Inflammatory diseases |
| Sarcoidosis |
| Peripheral vasculitis |
| Blood dyscrasias |
| Abnormalities in clotting cascade (e.g., von Willebrand disease) |
| Leukemia |
Which Symptoms Suggest Macular Disease?
Central scotoma (either relative or absolute), metamorphopsia, changes in image size, and acquired color vision change all suggest the possibility of macular disorders.
Which Symptoms Suggest Peripheral Retinal Disease?
Peripheral retinal disease is suggested by loss of visual field, flashes, and nyctalopia (decreased vision at night).
Which Diagnoses Are Suggested by Halos around Lights?
It is classically taught that corneal edema caused by sudden increased intraocular pressure causes halos around lights. Lenticular opacity and debris in the vitreous also may cause similar symptoms. Most patients note these halos or sunbursts around oncoming car lights when driving at night.
What Questions Should Be Asked of a Patient Who Complains of Blurred Vision?
Almost all patients consulting a retinal specialist complain of blurred vision, but it is the least specific symptom. The patient may complain, “I can’t see good,” “I can’t see the television,” or “My eye goes all dark-like.” They may be much more specific, for example, stating, “I have a dark spot in the middle.” Numerous questions must be asked to characterize the loss and to define a symptom complex.
The first task is to discern whether the concern is bilateral or unilateral. Unilateral visual loss may be asymptomatic to the patient for a long time and may be discovered incidentally when the eye is blocked. Other patients will not notice that their vision is decreased until they try to accomplish a monocular task, such as sighting a rifle.
Of particular importance is whether the symptoms are constant or intermittent. The patient who notes a graying-out of the vision in one eye leads the examiner to consider amaurosis fugax, pressure on the optic nerve, or increased intracranial pressure. Some patients describe an intermittent blur of vision that is likened to a lace curtain or gauze that floats in front of their vision; this symptom suggests vitreous opacities, particularly if the haze is mobile and floats back and forth at a different rate than eye movement.
It is particularly important to focus on whether the visual loss is considered to be diffuse, central, or peripheral. Central visual loss strongly points to macular disease, whereas peripheral loss suggests vascular disease, peripheral retinal disease (degeneration, infection, retinal detachment), optic nerve disease including glaucoma, or neurologic changes.
Specific conditions under which the visual loss is noted are of essential importance. Greater loss of clarity at near than distance is most commonly found in presbyopia, but in the patient with possible retinal disease, this phenomenon suggests a macular origin of the problem. Diabetic maculopathy classically creates greater degrees of near visual disturbance than distance vision change.
When visual loss is bilateral, it may be important to assess it with the patient’s systemic condition. Relatively acute bilateral vision changes can occur in diabetic patients whose blood sugar rises out of control. Changes in the hydration of the lens because of the difference between the intralenticular and extralenticular concentration of sugars is thought to account for much of this blurring. A drop of one or two lines of vision in each eye of patients with rapid decompensation of glucose control sometimes is noted even in pseudophakic patients. In the patient with the crystalline lens intact, spontaneous recovery may take as long as 6 weeks after the blood sugar is stabilized. Sudden bilateral vision loss, such as in homonymous hemianopia, may suggest neurologic disease. Episodic bilateral visual loss may occur in patients whose hypertensive medications have been changed and who develop temporary postural hypotension when they stand up.
The patient may notice other problems associated with unilateral visual loss that are mentioned only when specific questions are asked. For example, loss of stereopsis may lead the patient to miss the glass when attempting to pour water or to experience difficulty parking the car accurately.
Difficulty reading is a common complaint of patients with blurred vision. Whereas some patients are completely unaware of visual loss in one eye, loss of several lines of vision for others may lead to fairly significant difficulties. Patients may note a sense of confusion when trying to read and may block off the affected eye even when the vision is as good as 20/40. This sense of confusion may be more likely to occur if the dominant eye is affected by the disease process.
If visual loss is transient, several nonretinal diseases are suggested. In a young person with visual loss of approximately 20 minute duration, migraine is the likely diagnosis, whereas the older patient probably suffers from amaurosis fugax, suggesting ipsilateral carotid disease. A patient who has bilateral fleeting visual loss, particularly when engaging in activities that cause a Valsalva maneuver, will often be found to have bilateral disc edema. A unilateral presentation of the same symptoms may be found in the patient with a congenital disc anomaly.
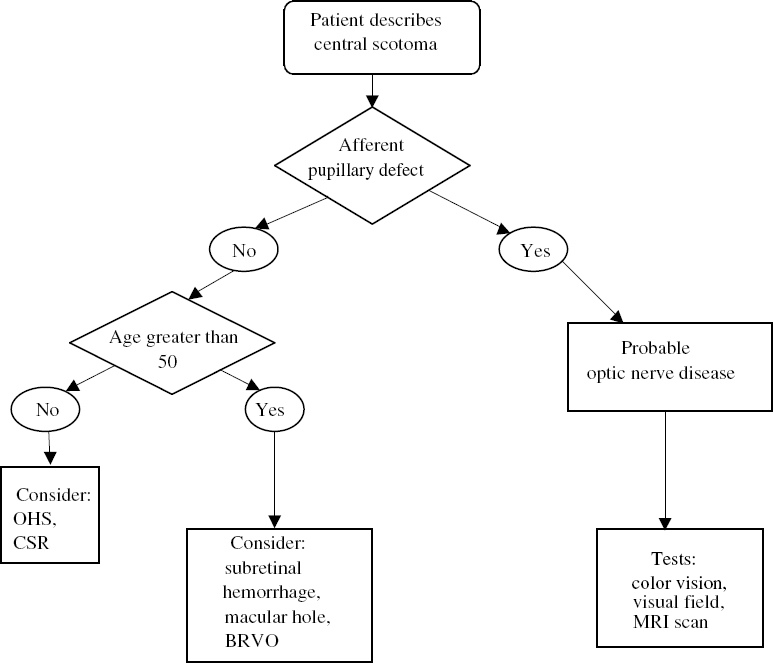
How Is the Patient with Symptoms of a Central Scotoma Evaluated?
The presence of a central scotoma indicates macular or optic nerve disease. Historically, if the patient is young, the differential diagnosis would include optic neuritis, central serous chorioretinopathy, subretinal hemorrhage, and inflammatory conditions of the macula or nerve, such as toxoplasmosis, histoplasmosis, and papillophlebitis. In older patients, optic nerve disease is a lesser possibility, and subretinal hemorrhage and macular hole assume greater importance in the differential diagnosis.
In the younger patient, associated symptoms such as pain on extraocular movement and neurologic symptoms tend to indicate optic neuritis. A pupillary examination is most helpful to establish the optic nerve as the site of abnormality. If subretinal neovascularization is suspected, ocular histoplasmosis and angioid streaks lead the list of possible diagnoses. Questions should include whether the patient has been under any undue stress (often thought to be associated with central serous chorioretinopathy) and whether the patient has spent time in the histoplasmosis geographic belt as a younger person.
The quality of the description of the abnormality gives some clue to the diagnosis. Patients with central serous retinopathy often notice a round area of defect in the vision, which they describe as being gray. Patients with a macular hole describe a smaller scotoma and may notice a loss of individual letters or words while reading. The scotoma tends to be denser in these cases. In patients with subretinal hemorrhage, the scotoma is more likely to be of irregular shape and more absolute or darker.
From a practical diagnostic viewpoint, the presence of an afferent defect is an important dividing line in pursuing the diagnosis (Fig. 5–1). In the patient with a significant afferent pupillary defect, optic neuritis should be considered; after the appropriate full ocular examination, color vision testing, and visual fields, a cranial magnetic resonance imaging (MRI) should be considered. In the patient without an afferent defect or a minimal afferent defect, the diagnosis will tend to subdivide on the basis of age.
In the younger patient, examination of the nerve for an optic pit is important if there is subretinal fluid. The most important test in the patient with subretinal fluid or suspected subretinal neovascularization in either age group is the fluorescein angiogram. Macular holes may be somewhat difficult to diagnose. The Watzke–Allen test is important in differentiating and can be performed easily. A narrow slip beam is shined on the macular hole; with a full-thickness hole, the patient may perceive a break in the line. Ocular coherence tomography and fluorescein angiography may be useful tests in establishing the correct diagnosis.
How Is the Patient with Metamorphopsia Evaluated?
When the patient complains of distorted vision, the examiner must be sure that there is actually metamorphopsia. Some patients use the word distortion to indicate general blurring. In ophthalmologic terms, metamorphopsia usually indicates that straight lines are bent or distorted. The Amsler grid may be used to demonstrate what the examiner means by metamorphopsia and to confirm its presence. This symptom points to a macular cause and most often indicates subretinal fluid or blood, epiretinal membrane, or venous occlusive disease producing cystoid macular edema. In determining whether the patient has true metamorphopsia, questions about the appearance of straight lines and the usual visual environment are sometimes helpful. Many patients will note that there is actually a distortion on a line of print so that one set of letters moves upward. Others notice a small scotoma or complain that the words tend to “jump around.” Many patients notice that straight lines, such as door frames, telephone poles, or telephone lines, are “bent.” Many patients already have been given an Amsler grid and will consult the physician because of changes on the Amsler grid itself.
Once the patient’s pupils are dilated, a thorough biomicroscopic examination of the macula is indicated. Fluorescein angiography is often useful to search for the cause of the distortion of the macula, which is almost invariably found as the cause of the distortion of vision.
How Is the Patient with the Change in Image Size Evaluated?
Patients often notice a difference in image size if a refractive error produces greater than a 2.5-diopter difference between the two eyes. More often, the alteration in image size is acquired and is accompanied by other symptoms, usually blurring of vision. The first question to ask is whether the altered image is larger or smaller. In general, patients are able to make this distinction and are able to tell which eye is involved. A larger image is almost pathognomonic of epiretinal membrane with macular distortion (Fig. 5–2). A smaller image is highly suggestive of a neurosensory detachment of the macular retina.