The pathogenesis of acquired attic cholesteatoma remains unclear. Of many theories that have been described so far the most important are the retraction theory, the proliferation theory, the migration theory, and the metaplasia theory. There are many articles in the international literature describing these theories and trying to substantiate them.
In 2000, Sudhoff and Tos1 promoted a combination of retraction and proliferation theories in explaining the pathogenesis of attic cholesteatoma. They first described four types of attic retraction (▶ Fig. 12.1: type 0 representing no retraction):
Type 1: slight retraction with air between Shrapnell’s membrane and the neck of the malleus
Type 2: retraction down to the malleus neck with possibility of adhesion
Type 3: retraction behind the scutum with some bone resorption
Type 4: retraction behind the scutum with considerable bone resorption, making the malleus head and incus body visible.
They also proposed a possible pathogenesis of attic cholesteatoma based on clinical and immunohistochemical findings. They divided cholesteatoma pathogenesis into four stages:
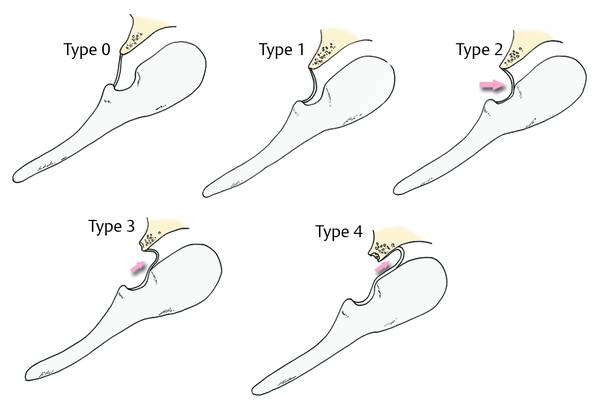
Fig. 12.1 The attic retraction classification of Sudhoff and Tos.
Retraction pocket stage
Proliferation stage of the retraction pocket, subdivided into cone formation and cone fusion
Expansion stage of attic cholesteatoma
Bone resorption.
Retraction theory is certainly based on middle ear chronic dysventilation and inflammation. Ventilation of the middle ear is a combination of anatomical structures and physiological processes. Although the eustachian tube is a crucial structure in influencing gas exchange and pressure homeostasis, some other factors also appear to play important roles. As Sadé and Ar2 state, mastoid air volumes may possibly act as an air “reservoir” or “buffer.” The larger the air content of the mastoid bone, the greater is its ability to compensate middle ear pressure variations. Moreover, it is well documented that the mastoid mucosa contributes to middle ear gas exchange and that mucosal gas exchange is related to the degree of mastoid pneumatization. It is clear that this physiological gas exchange is interrupted by traditional microscopic approaches that include mastoidectomy.
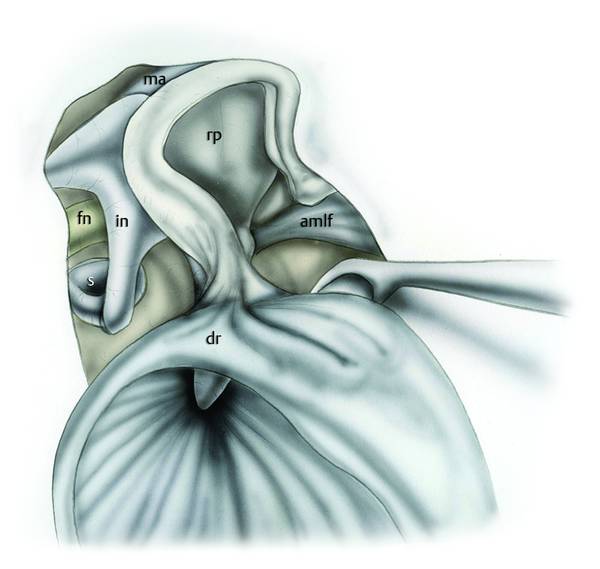
Epitympanic ventilation routes have a fundamental role in the context of attic retraction pockets. Epitympanic compartments receive their aeration via the large tympanic isthmus between the medial part of the posterior incudal ligament and the tensor tendon. Palva et al3 observed that the aeration pathway from the eustachian tube leads directly to the mesotympanic and hypotympanic spaces, whereas the epitympanum is out of the direct air stream and is only aerated through the tympanic isthmus (▶ Fig. 12.2).
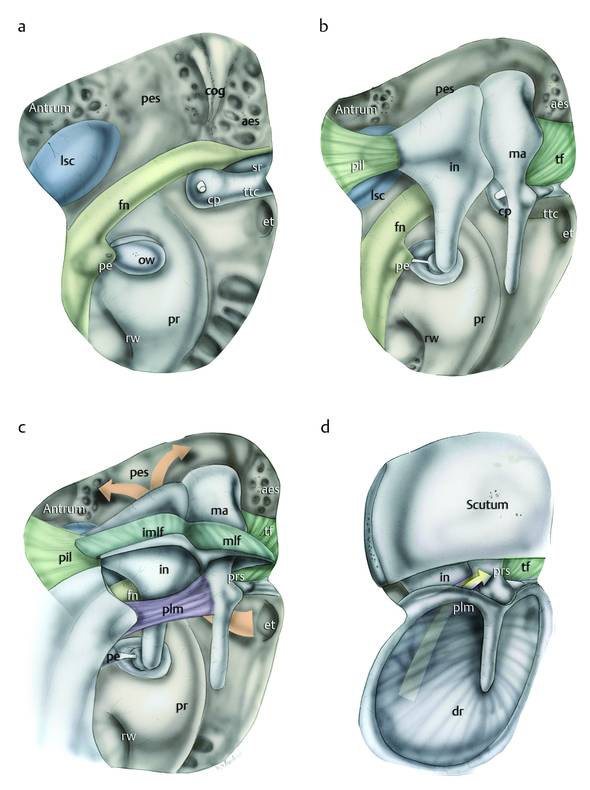
Fig. 12.2 Drawing to clarify middle ear anatomy related to the ventilation pathway of the epitympanum. a Right ear. The ossicular chain and related ligamental folds, the eardrum, and the scutum have been removed; the medial wall of the tympanic cavity is observable. Note the position of the eustachian tube with respect to the epitympanic compartment. Anatomically the tympanic facial nerve represents the floor of the posterior epitympanic space; in contrast, the semicanal of the tensor tendon represents the floor of the anterior epitympanic space. b The ossicular chain with the tensor fold and the posterior ligamental fold of the incus are repositioned on the tympanic cavity; the incudomalleolar joint occupies the epitympanic space, and the surrounding space between this joint and the medial wall of the epitympanum is narrow. c The lateral ligamental folds of the incus and malleus with the posterior and anterior ligamental folds of the malleus are inserted in the correct position and the epitympanic diaphragm is complete; the orange arrow indicates the aeration pathway from the eustachian tube to the epitympanum. d The scutum and the eardrum have been repositioned, the space between the posterior ligamental fold of the malleus and the eardrum represents the posterior pouch. This anatomical area is the main ventilation route from the mesotympanum to the Prussak space (“lower unit”) and is independent of the ventilation route of the epitympanum (“upper unit”). ma, malleus; in, incus; dr, eardrum; fn, facial nerve; tf, tensor fold; cp, cochleariform process; et, eustachian tube; ttc, tensor tympani canal; lsc, lateral semicircular canal; pr, promontory; rw, round window; pe, pyramidal eminence; aes, anterior epitympanic space; pes, posterior epitympanic space; ow, oval window; pil, posterior ligamental fold of the malleus; prs, Prussak space; plm, posterior ligamental fold of the malleus; imlf, incudomalleolar lateral fold; mlf, malleolar lateral fold; sr, supratubal recess.
The lower unit of the epitympanum is a reduced compartment represented by the Prussak space (▶ Fig. 12.2). It is separated anatomically and physiologically from the upper unit by its vault, which is represented by the lateral malleal ligament fold. This inferior epitympanic portion is ventilated in the majority of cases from the posterior pocket through the mesotympanum. For this reason the two ventilatory trajectories of the epitympanic units are separated from each other. Restoration of ventilation pathways with unification of the upper and the lower units through the creation of a large tympanic isthmus and an accessory route through the tensor fold is the basis of this surgery, which is intended to ensure ventilation to all parts of epitympanum (▶ Fig. 12.3, ▶ Fig. 12.4, ▶ Fig. 12.5).
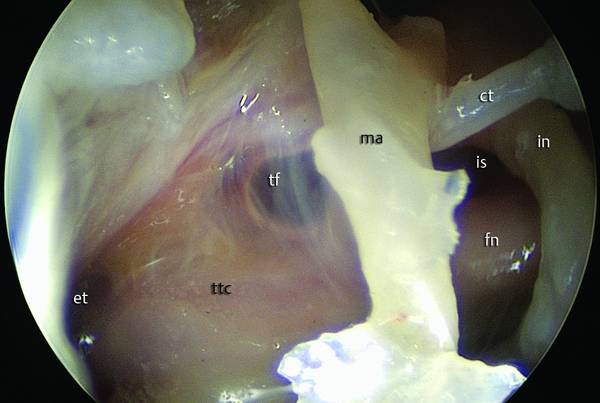
Fig. 12.3 Left ear. Endoscopic view (45° endoscope) of the tympanic isthmus and tensor fold. The tensor fold is a complete fold dividing the anterior epitympanic space from the protympanum; the anterior isthmus is located between the cochleariform process and the incudostapedial joint. ma, malleus; ttc, tensor tympani canal; et, eustachian tube; fn, facial nerve; is, isthmus; ct, chorda tympani; in, incus; tf, tensor fold.
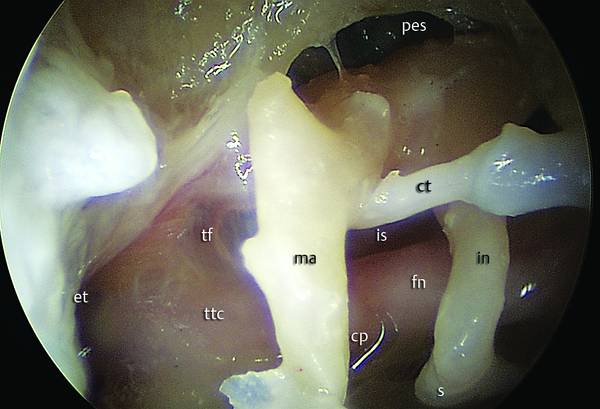
Fig. 12.4 Left ear. Endoscopic view of the epitympanic diaphragm, after removal of incudomalleolar lateral ligamental folds. The isthmus is endoscopically observable with a 45° endoscope. This anatomical area represents the main ventilation route from the mesotympanum to the epitympanic compartments; anteriorly the attic is divided by the tensor fold. ma, malleus; ttc, tensor tympani canal; et, eustachian tube; fn, facial nerve; is, isthmus; ct, chorda tympani; in, incus; cp, cochleariform process; tf, tensor fold; s, stapes; pes, posterior epitympanic space.
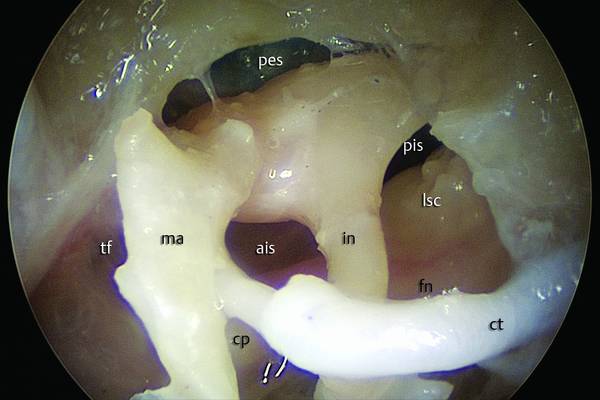
Fig. 12.5 Left ear. Endoscopic view of the epitympanic diaphragm: using a 45° endoscope the entire isthmus is endoscopically visible. The anterior isthmus is located between the cochleariform process and the incudostapedial joint; the posterior isthmus is located between the incudostapedial joint and the posterior incudal ligamental fold. ma, malleus; fn, facial nerve; ais, anterior isthmus; pis, posterior isthmus; ct, chorda tympani; in, incus; cp, cochleariform process; tf, tensor fold; pes, posterior epitympanic space; lsc, lateral semicircular canal.
The tensor fold has a strategic position because it prevents communication between the supratubal recess, the region belonging to the mesotympanum, and the overlying anterior epitympanum (▶ Fig. 12.6, ▶ Fig. 12.7). When the tensor fold is complete, the only ventilation pathway to the anterior epitympanic space is through the isthmus. The tensor fold has a very variable anatomy: in most patients it shows a superior concavity, extending laterally from the semicanal of the tensor tympani muscle to the lateral aspect of the protympanum, adhering posteriorly to the cochleariform process and to the tensor tympani tendon, and extends anteriorly to the root of zygomatic bone that becomes the epitympanic floor. When it inserts on the transverse crest its direction is almost vertical, whereas if it inserts on the tubaric tegmen its direction is rather horizontal (▶ Fig. 12.8).4
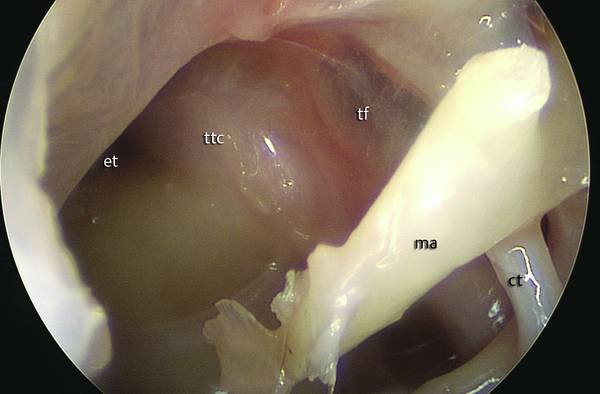
Fig. 12.6 Left ear. Endoscopic view of the protympanum and inferior edge of the tensor fold (0° endoscope). In this patient the tensor fold has a horizontal orientation; this fold is complete, separating the semicanal of the tensor tendon from the anterior epitympanic space. When the tensor fold has this conformation, no supratubal recess is present. ma, malleus; tf, tensor fold; ttc, tensor tympani canal; et, eustachian tube.
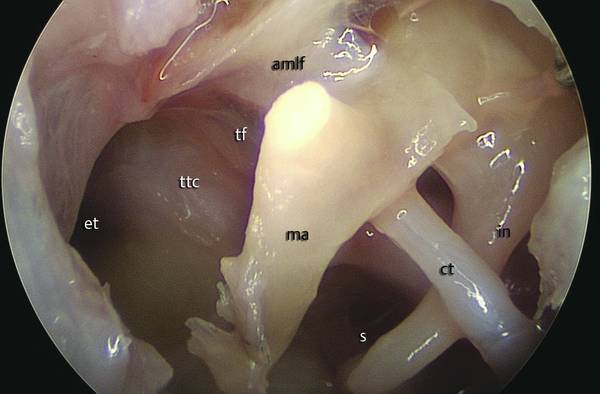
Fig. 12.7 Left ear. Endoscopic view of the entire protympanum with a 0° endoscope. ma, malleus; ct, chorda tympani; in, incus; tf, tensor fold; ttc, tensor tympani canal; et, eustachian tube; s, stapes; amlf, anterior malleolar ligamental fold.
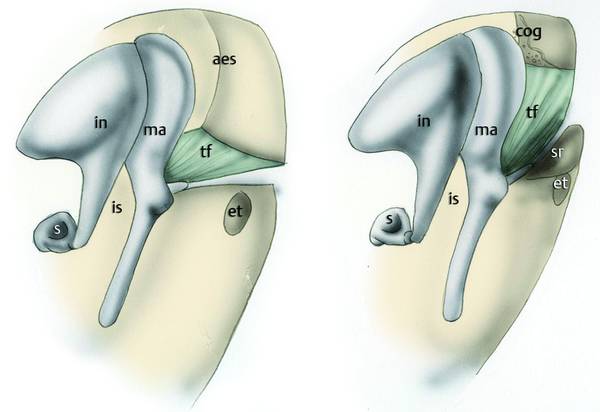
Fig. 12.8 The two major anatomical variations of the tensor fold. On the left, the tensor fold with horizontal orientation; in this case the tensor fold is attached to the semicanal of the tensor tendon of the malleus; no supratubal recess is present. On the right, the tensor fold with vertical orientation; in this case the fold is attached superiorly on the cog and a supratubal recess is present with variable depth. ma, malleus; in, incus; tf, tensor fold; et, eustachian tube; s, stapes; is, isthmus; sr, supratubal recess; aes, anterior epitympanic space.
Epitympanic ventilation may be impaired by various anatomical variations and by isthmus blockage. We have classified anatomical variations of the tensor fold and the isthmus that cause different epitympanic ventilation blockages into three types (▶ Fig. 12.9)5:
Type A: blockage of the isthmus associated with a complete tensor fold.
Type B: blockage of the isthmus associated with an attic vertical blockage, and consisting of a mucosal fold with a vertical orientation separating the anterior epitympanic space from the posterior epitympanic space with or without a complete tensor fold.
Type C: complete epidermization of the attic space causing a blockage of the isthmus, a complete antrum blockage, and epidermization of the tensor fold area isolating the mesotympanic space from the epitympanic and mastoid spaces. Different types of tympanoplasty are performed depending on the presence of pathological tissue, the tensor fold, and isthmus and ossicular conditions.
The tympanic isthmus remains the cornerstone of the epitympanic ventilation route. The tensor fold is an accessory route that may help ventilation of the upper space and it needs to be opened during endoscopic surgery, though this might be insufficient if surgery fails to restore a functioning isthmus.
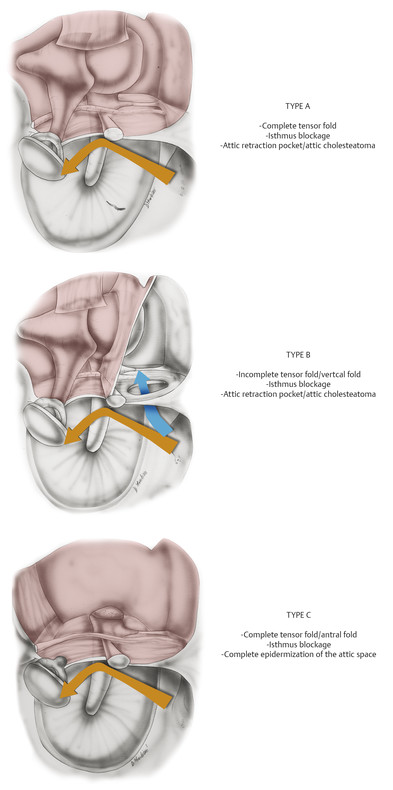
Fig. 12.9 Classification of epitympanic ventilation blockage correlated with the endoscopic findings. Left ear viewed from medially to laterally.
In relation to our previous articles6 attic retraction pockets can be classified as four anatomical-physiological types (▶ Fig. 12.10):
Isolated Prussak space retraction pocket due to an isolated obstruction of the von Tröltsch pouch, with a normal tympanic isthmus. It does not usually expand through the attic spaces and is self-limiting.
Anterior attic retraction pocket: progressive selective dysventilation of the anterior epitympanum, related to a complete tensor fold and to an anomalous isthmus-anterior attic ventilation route (e.g., the presence of a vertical fold; underdevelopment of anterior epitympanic compartments, causing reduced ventilation between the ossicular chain and epitympanic walls).
Posterior attic retraction pocket. This is rare: a selective and progressive posterior dysventilation due to isthmus blockage with presence of a vertical fold (type B ventilation blockage). The tensor fold is generally incomplete.
Complete attic retraction pocket. This is found more frequently; characterized by a progressive retraction of both anterior and posterior epitympanic compartments due to type A ventilation blockage with a complete tensor fold associated with isthmus blockage. In this scenario there is a complete exclusion of epitympanic compartments from the mesotympanic space.
This classification helps the surgeon in planning the correct surgery on the basis of the type of dysventilation.
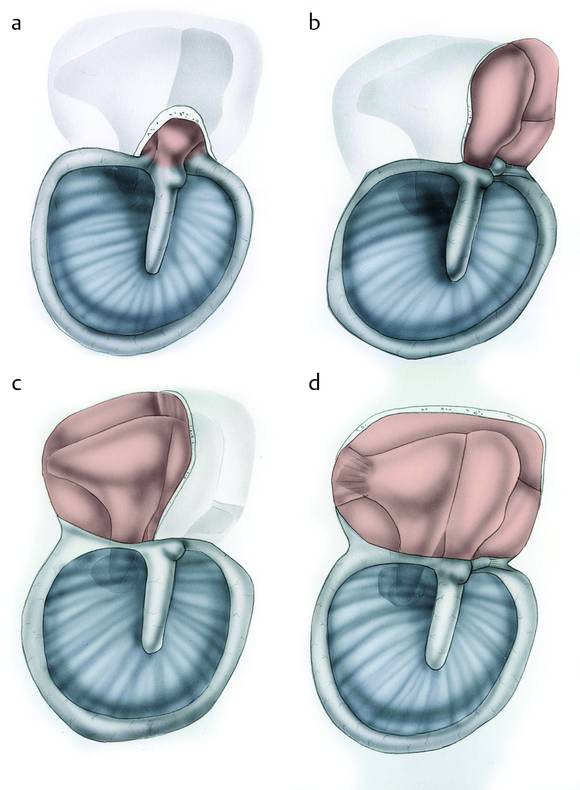
Fig. 12.10 Classification of attic retraction pockets. a Isolated Prussak space retraction pocket. b Anterior attic retraction pocket. c Posterior attic retraction pocket. d Complete attic retraction pocket.
12.2 History
The anterior epitympanic space has always been a critical point in cholesteatoma surgery. It is not easily accessible and residual pathology may be hidden from the surgeon’s view. Canal wall up technique provides a difficult view of the anterior portion of the epitympanic space and cholesteatoma retention rates can be higher. Direct exposure of the anterior epitympanic space is needed to completely remove pathology. Wullstein7 was the first to describe a technique intermediate between canal wall up and canal wall down: he proposed a lateral epitympanotomy with subsequent osteoplastic reconstruction. Several techniques of bony wall reconstruction followed Wullstein’s description.
Surgery of the epitympanic space, regardless of which technique is used, has two basic goals: removal of pathology and restoration of a route of ventilation. With this in mind, it is easily understandable why removal of the tensor fold is an important step that goes along with restoration of the tympanic isthmus. Removal of the tensor fold with a microscopic approach is difficult. A canal wall up technique does not permit the visualization of the tensor fold, because the working angle is through the ear canal and the tensor fold remains hidden behind the neck of the malleus. For this reason, Morimitsu et al8 proposed an “anterior tympanotomy.” These authors removed bone from the lateral attic to the zygoma. In this way, the working axis frontally became parallel to the axis of the ear canal. After this bone removal, it was possible to drill in front of the head of the malleus and remove the tensor fold. Palva et al9 suggested tensor fold excision to create a large new attic aeration pathway during cholesteatoma surgery by an endaural atticotomy extending to the supratubal recess. When the ossicular chain was intact, the authors suggested cutting the neck of the malleus to allow lateral lifting of the manubrium. This approach exposed the tensor tendon and allowed excision of the tensor fold.
In our experience10 the tensor fold is easily reachable with a transcanal endoscopic approach. Endoscopic examination of the tensor fold area is possible using an endoscope of 3 mm diameter and with a 45° endoscope inserted in the protympanic region; this position allows good exploration of the inferior edge of the tensor fold. The tensor fold is then removed with an angled instrument and with endoscopic monitoring. In some cases, anterior atticotomy exposed the superior face of the tensor fold seen by the endoscope inserted into the anterior epitympanic region and rotated inferiorly.
12.3 General Surgical Evaluation
12.3.1 Indications and Contraindications
Indications
Self-cleaning epitympanic retraction pocket endoscopically visible, but worsening at periodic follow-up (Tos types 2 and 3)
Non–self-cleaning epitympanic retraction pocket that is not visible with a 45° angled endoscope (Tos type 4)
Cholesteatoma involving the attic space with or without extension to the mesotympanic, hypotympanic, and retrotympanic spaces, but not involving the antrum or mastoid cavity.
Contraindications
Poor health
External ear malformations
Narrow external ear canal
Cholesteatoma involving antrum and mastoid cavity
Tegmen tympani dehiscence
Lateral semicircular canal dehiscence (relative contraindication).
12.3.2 Advantages
Better visualization of the anterior epitympanic space and possible preservation of the ossicular chain if the pathology involves the anterior epitympanum
Evaluation of the epitympanic diaphragm and tympanic isthmus
Restoration of the physiological ventilation route from the protympanic space to the epitympanum and mastoid cavity through the tympanic isthmus and an opened tensor fold
Minimally invasive approach without retroauricular incision and preserving the mastoid cavity and mucosa—important for the homeostasis of the middle ear.
12.3.3 Complications
Complications are similar to those for microscopic approaches and are related to the anatomical structures involved.
12.3.4 Preoperative Evaluations
The goals of a transcanal endoscopic approach are preservation of the mastoid bone and mastoid mucosa (important for middle ear homeostasis), removal of tympanic and epitympanic cholesteatoma, and restoration of epitympanic and mastoid ventilation by opening the tympanic isthmus and tensor fold.
Surgery has to be planned on the basis of the extension of the pathology: if a cholesteatoma involves the antrum or mastoid cavity, an exclusively endoscopic approach is contraindicated. Preoperative staging is fundamental in this kind of surgery. Middle ear CT scans are helpful in evaluating cholesteatoma extension even though sometimes cholesteatoma and inflammatory tissue in the mastoid cavity look the same. For this reason, diffusion-weighted MRI might be helpful for correct staging of cholesteatoma.
We consider that correct staging of cholesteatoma is also important for follow-up evaluation and long-term results. It should be applied to every cholesteatoma approach: endoscopic, microscopic, or combined modality.
12.4 Epitympanic Cholesteatoma Staging
For epitympanic cholesteatoma staging, see ▶ Table 12.1.
| Category | Stage |
| Site | Lateral attic (with anterior epitympanum) |
| Medial attic | |
| Subsite | Mesotympanum |
| Protympanum | |
| Hypotympanum | |
| Retrotympanum | |
| Antrum | |
| Mastoid | |
| Extension | C1: cholesteatoma with limited attic extension |
| C1a: cholesteatoma involving only the lateral attic | |
| C1b: cholesteatoma involving also the medial attic | |
| C2: cholesteatoma with extension in 1 or more subsite | |
| C2a: posterior extension to the antrum and mastoid | |
| C2b: inferior extension to the mesotympanic, protympanic and hypotympanic regions | |
| C2c: both posterior and inferior extension | |
| C3: cholesteatoma involving retrotympanic space (sinus tympani/subtympanic sinus; subpyramidal space) and/or with facial nerve involvement | |
| C4: cholesteatoma involving inner ear or petrous apex | |
| C4a: Any preview stages with middle cranial fossa dura involvement | |
| C4b: infiltration of otic capsule and/or labyrinth and/or ear vestibule and/or cochlea. | |
| C4c: infiltration of petrous apex with or without carotid involvement and/or infiltration of inner ear. | |
| Characteristics | S1: cholesteatoma in pouch shape |
| S2: cholesteatoma with infiltrative matrix | |
| Patient’s characteristics | A: adult |
| B: pediatric patient (<14 years) |
In this chapter only surgical steps for cholesteatoma staging C1a and C1b will be described. For cholesteatoma C2a and C2c an exclusively endoscopic approach is contraindicated.
12.5 Surgical Steps
12.5.1 Incision and Tympanomeatal Flap Elevation
The incision is made clockwise from the 3 o’clock to the 9 o’clock position, 1.5 to 2 cm from the anulus, using a molecular resonance microscalpel (Vesalius) (Clinical case 1 [▶ Fig. 12.11, ▶ Fig. 12.12]).
Key point: Hypotension and use of the anti-Trendelenburg position are very important aids in this kind of surgery.
Dissection is performed with cottonoids soaked in epinephrine solution. The flap is elevated using a microdissector, applying traction with the cottonoids on the bone surface of the external ear canal. The flap is elevated anteriorly until identification of the anulus is achieved. This first step is very important in the transcanal endoscopic approach because the skin of the ear canal can bleed and thus jeopardize the endoscopic procedure.
In underlay dissection of the anulus, the flap is separated from the posterior malleolar fold. Accurate dissection of the pars flaccida from the retraction pocket or cholesteatoma sac is made from top to bottom
Key point: Our recommendation is a sharp dissection with a microscalpel or a microhook.
Dissection proceeds anteriorly to the small process of the malleus; the anterior anulus is now visible and the tympanic flap is transposed inferiorly through an underlay dissection and the protympanic space is uncovered. The tympanomeatal flap is dissected from the long process of the malleus as far as the umbus. If necessary a complete inferior transposition of the flap may be made, dissecting the flap from the umbus with microscissors. The protympanic space and eustachian tube are now visible and the mesotympanic mucosa can be explored (▶ Fig. 12.13).
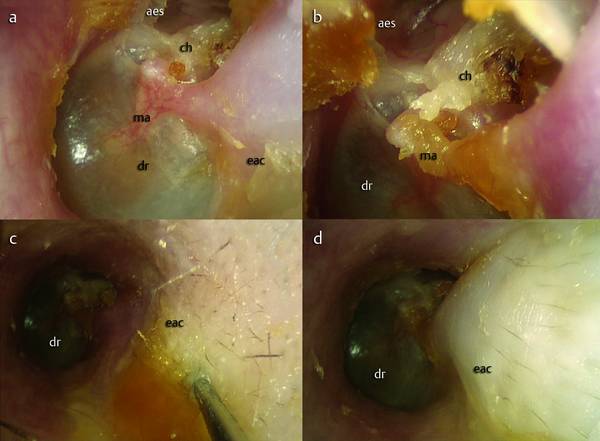
Fig. 12.11 Clinical case 1. Left ear. Transcanal endoscopic approach. An epitympanic cholesteatoma is detected endoscopically (a, b); the mesotympanum is well ventilated. An injection of epinephrine solution is made in the posterior portion of the ear canal (c, d). aes, anterior epitympanic space; ma, malleus; eac, external auditory canal; dr, eardrum; ch, cholesteatoma.
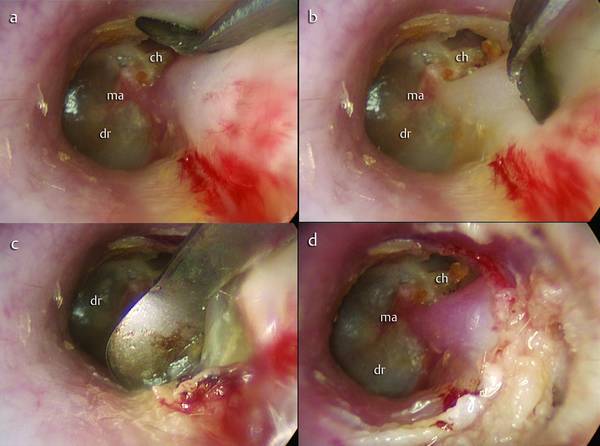
Fig. 12.12 Clinical case 1. Left ear. Transcanal endoscopic approach (a). The skin incision is made with a Vesalius dissector (b, c) in order to reduce the bleeding during the dissection of the tympanomeatal flap (d). ma, malleus; dr, eardrum; ch, cholesteatoma.
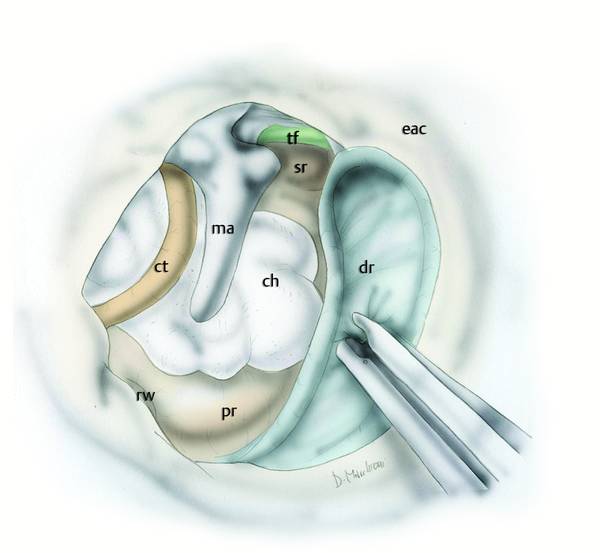
Fig. 12.13 Dissection of the tympanomeatal flap is carried out from posterior to anterior and from superior to inferior; the eardrum is detached from the handle of the malleus until the protympanum and the tensor fold area are endoscopically detectable. ma, malleus; dr, eardrum; ch, cholesteatoma; sr, supratubal recess; tf, tensor fold; pr, promontory; rw, round window; ct, chorda tympani; eac, external auditory canal.
12.5.2 Middle Ear Mucosa and Evaluation of Ventilation Routes
The tympanic isthmus and the tensor fold are now evaluated. In patients with pathology limited to the attic, the epitympanic diaphragm is easily evaluated through an endoscopic approach (▶ Fig. 12.14).
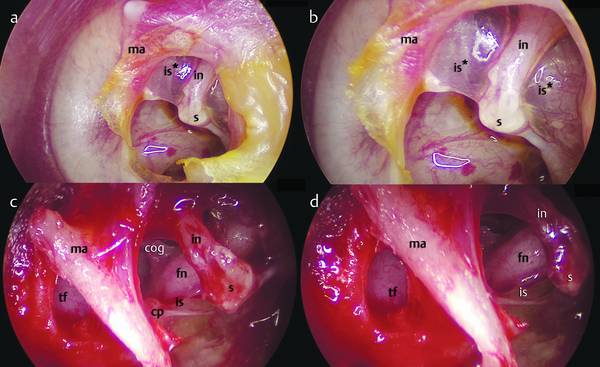
Fig. 12.14 Left ear. a, b Endoscopic views of the tympanic isthmus; in this case the isthmus is blocked by a mucosal fold involving the incudostapedial joint. c, d Endoscopic views of the isthmus (45° endoscope) after removal of the blockage and tensor fold: note a well-ventilated attic with open isthmus. ma, malleus; tf, tensor fold; in, incus; fn, facial nerve; s, stapes; is*, isthmus blockage; is, open isthmus; cp, cochleariform process.
During the surgical approach to the middle ear we have to introduce the endoscope into the middle ear cavity; a 3 mm-diameter, 15 cm-long endoscope is needed to evaluate the epitympanic diaphragm. With this we are able to examine the tympanic isthmus and the tensor fold area, appreciating the epitympanic diaphragm of the upper unit. This transcanal lateral approach permits good exposure of the tympanic isthmus. Endoscopic examination of the tympanic isthmus is possible using 0° and 45° endoscopes of 3 mm diameter. Inserting the instrument into the tympanic cavity, we can explore all of the large tympanic isthmus between the medial part of the posterior incudal ligament posteriorly and the tensor tendon anteriorly (see Clinical case 2 [▶ Fig. 12.15, ▶ Fig. 12.16]). The 0° endoscope allows us a magnified view of the space between the incudostapedial joint and cochleariform process with the tensor tendon (Proctor’s anterior isthmus); complementing this, after posterior atticotomy the 45° endoscope permits a magnified view of the space between the pyramidal process and the short process of the incus (Proctor’s posterior isthmus) (▶ Fig. 12.16). Using a 45° endoscope of 3 mm diameter, the tensor fold area can be examined endoscopically by two approaches:
Inferior approach: the endoscope is introduced into the protympanic region, identifying the eustachian tube and supratubal recess. This position allows good exploration of the inferior edge of the tensor fold.
Superior approach: for a good view of the superior edge of the tensor fold we must perform a wide anterior atticotomy, exposing the anterior epitympanic space. This procedure allows a good view of the superior edge of the tensor fold.
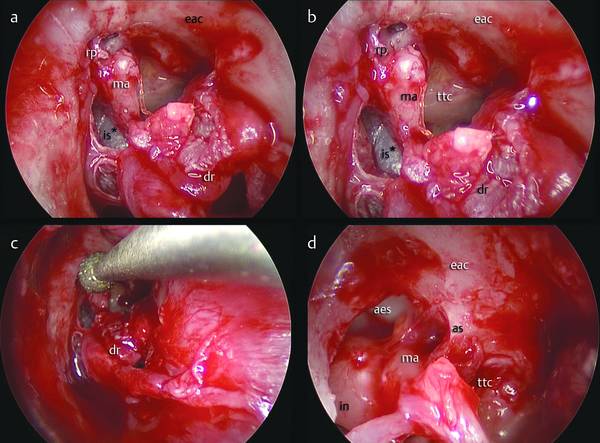
Fig. 12.15 Clinical case 2. Right ear. Transcanal endoscopic approach to retraction cholesteatoma. a, b The tympanomeatal flap has been elevated: a retraction pocket of the attic is visible with a blockage of the isthmus. c Transcanal atticotomy is performed to provide direct access to the retraction pocket. d The anterior epitympanic space after removal of the retraction (45° endoscope). ma, malleus; is*, isthmus blockage; rp, retraction pocket; dr, eardrum; ttc, tensor tympani canal; eac, external auditory canal; aes, anterior epitympanic space; as, anterior spine; in, incus.
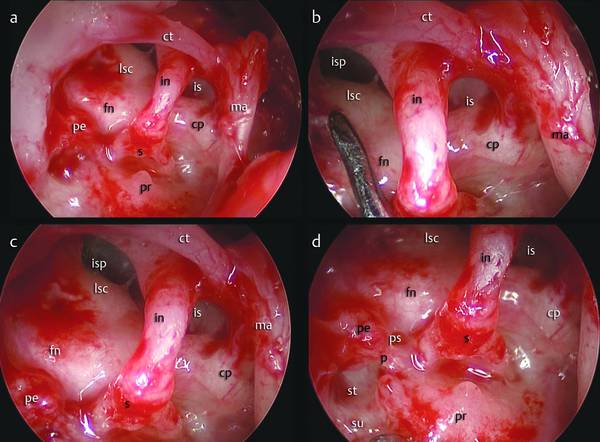
Fig. 12.16 Clinical case 2. Right ear. Transcanal endoscopic approach to retraction cholesteatoma. a–d Endoscopic views of the retrotympanum. After removal of the isthmus blockage, the isthmus is detected using a 45° endoscope. At the final check, the posterior and the anterior isthmus are open, the attic is well ventilated, and the ossicular chain is preserved. ma, malleus; is, isthmus; isp, posterior isthmus; pr, promontory; s, stapes; in, incus; pe, pyramidal eminence; lsc, lateral semicircular canal; fn, facial nerve; cp, cochleariform process; ps, posterior sinus; st, sinus tympani; p, ponticulus; su, subiculum; ct, chorda tympani.
12.5.3 Selective Epitympanic Retraction Pocket
The depth of the pocket is evaluated with a 45° endoscope. The superior margin of the pocket is dissected with a curved dissector to isolate bone of the scutum (▶ Fig. 12.17). A transcanal atticotomy is performed using a microdrill system under endoscopic vision until the epitympanic compartments are visible (▶ Fig. 12.18). Now the most cephalic and medial portions of the pocket are dissected from the bone and the pocket is dislocated inferiorly, thus exposing the ossicular chain and incudomalleolar joint (▶ Fig. 12.19). The pocket is now attached at the small process of the malleus and, whenever possible, is removed “en bloc” (▶ Fig. 12.20, ▶ Fig. 12.21, ▶ Fig. 12.22).