 visceration is the removal of the contents of the globe while leaving the sclera and extra-ocular muscles intact. Evisceration is usually indicated in endophthalmitis that does not respond to medication or for cosmetic improvement of a blind eye.
visceration is the removal of the contents of the globe while leaving the sclera and extra-ocular muscles intact. Evisceration is usually indicated in endophthalmitis that does not respond to medication or for cosmetic improvement of a blind eye.
The patient is informed that it is impossible to achieve or retain any vision with this procedure and that removal of the eye is essential to resolve the inflammation or unsightliness of the eye. The patient is also counseled regarding the form of cosmetic improvement to be expected, with or without inserting an implant within the empty scleral shell, either at surgery or at some future point.
No case of sympathetic ophthalmia after evisceration has been reported. If the slightest chance of saving some useful sight in trauma cases exists, the eye should not undergo evisceration.
The primary challenge in operating on soft infected eyes is making a clean incision on a soft cornea or limbus. A secondary consideration is the possibility of spreading infection through the channels by cutting manually with a knife or scissors. Both these challenges can be overcome by making incisions with a Fugo blade.
Surgical Technique
- Use a 100-µm Fugo blade tip set at medium power and high energy to incise the cornea near the limbus. Move the activated tip along the desired incision line inside the limbus and continue to make a gutter in the cornea. Because the cornea is usually thick in these cases, it takes two or three passes to go through and reach inside the eye. Make the incision in such a way that no infected tissue is kept at the incision margin. If an infective process is invading the sclera, make the incision proximally so as to pass through healthy sclera.
The sharpest cutting knives, including diamond knives, often cannot make a clean-cut incision because they can work only in the presence of tissue resistance. They are not suitable for use in infected, soft eyes. But the Fugo blade cuts either a soft eye or a hard eye with equal facility.
- Cut the uveolenticular mass. Lift the incised corneal tissue to reveal the inflammatory mass, lens, vitreous, and uveal tissues, inextricably mixed. In the central area, pull and excise this mass with the Fugo blade.
- Pull the ciliary body away from the sclera and insert a spatula in the suprachoroidal space, thus separating the sclera from the uveal–retinal tissue. Move the spatula around in every direction and as deep into the sclera as possible. Remove the entire mass with several scrapes of the spatula (Fig. 47.1). My colleagues and I do not use evisceration spoons because they cause excessive trauma to the internal surface of the sclera. Surgical trauma should be minimized in infected cases.
- Rinse the empty scleral cavity with povidine–iodine.
- Pull the ciliary body away from the sclera and insert a spatula in the suprachoroidal space, thus separating the sclera from the uveal–retinal tissue. Move the spatula around in every direction and as deep into the sclera as possible. Remove the entire mass with several scrapes of the spatula (Fig. 47.1). My colleagues and I do not use evisceration spoons because they cause excessive trauma to the internal surface of the sclera. Surgical trauma should be minimized in infected cases.
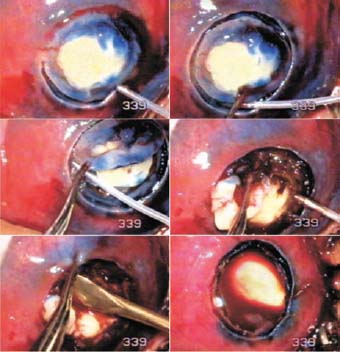
Figure 47.1. Fugo blade incisions in the limbus area cut the cornea to full depth. The uveovitreolenticular mass is excised. A spatula is introduced in the suprachoroidal space to remove the contents. The scleral cavity is cleared of tissue.
Any additional surgical steps are determined by several factors, such as the age of the patient, original cause of the loss of the eye, and any cosmetic treatment planned.
Summary
The Fugo blade’s capacity to cut successfully in situations in which no tissue resistance is present has stimulated interest in harvesting sclerocorneal buttons from cadaver eyes, which are transferred directly to preservative medium bottles.
Suggested Reading
Albert DM, Diaz-Rohena R. A historical review of sympathetic ophthalmia and its epidemiology. Surv Ophthalmol. 1989;34:1–14.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


