Chapter 139 Epidemiology of Posterior Uveal Melanoma
Introduction
The underlying causes of uveal melanoma are not clearly established. Because we do not have a means to prevent this disease, epidemiologic research is key to determine associated factors and to better understand the mechanisms of disease development. This chapter will focus on posterior uveal melanoma (choroidal and ciliary body melanoma) and will not include a discussion of iris melanoma, which can be reviewed elsewhere.1
Posterior uveal melanoma is an uncommon disease with an incidence of 5–6 cases per 1 million population per year. It is usually diagnosed in the sixth decade of life, and its incidence rises steeply with age. It is the most common primary intraocular malignancy, and the leading primary intraocular disease which can be fatal in adults. Although posterior uveal tract melanoma is the most common noncutaneous form of melanoma, the incidence rate is one eighth that of cutaneous melanoma in the USA.2
Incidence
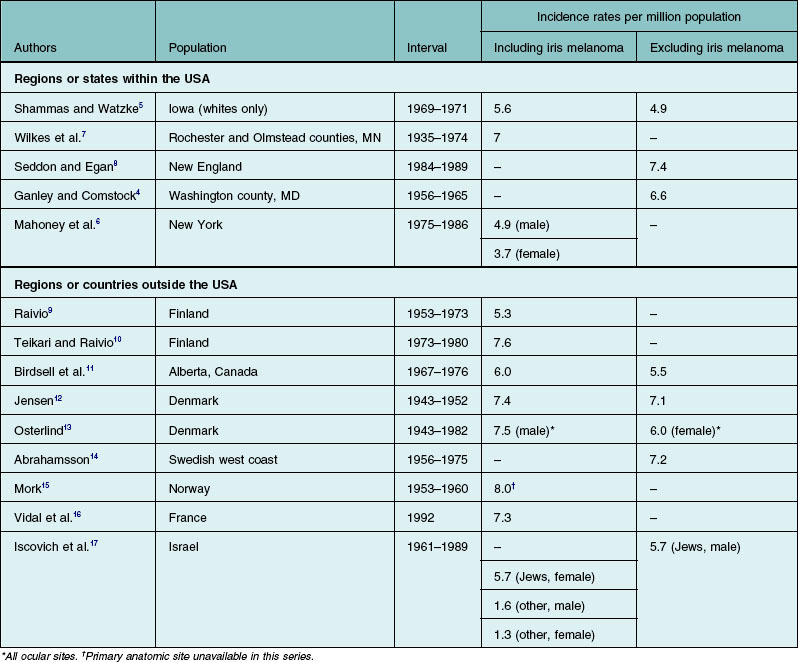
According to the most recent report of data obtained from the Surveillance, Epidemiology, and End Results (SEER) program database in the USA (1973–2008), the mean age-adjusted incidence estimate for ocular melanoma in the USA is 5.1 cases per 1 million population.3 Similar estimates for uveal melanomas of the choroid and ciliary body4,5 or the choroid, ciliary body, and iris5–7 have been reported for individual states or regions within the USA. Other surveys of primarily white populations have found incidence rates similar to those of the USA (Table 139.1).8–17 The incidence rate in black Africans is unknown but thought to be extremely low.18–21 In the USA, the rate of the disease in African Americans is less than one-eighth of the rate for whites.2 Although small fluctuations in several populations have been observed,22,23 the incidence and mortality rates of uveal melanoma have been shown to be fairly stable over the past several decades.24,25 It is important to note that comparative incidence rates across populations must be interpreted with caution – differences in case definition, methods of case ascertainment, and methods of age-adjustment could affect the relative incidence rates.
Host factors
Age and sex
Uveal melanoma is rare in children.26–28 In most series, the median age at diagnosis is 55 years.9,12 In Jensen’s series,12 rates of disease decreased in males after age 69 years. An evaluation of uveal melanoma cases reported to the Finnish Cancer Registry between 1953 and 1982,9,10 found that rates of disease in females leveled off beginning in the mid-60s, but in males of the same age, rates continued to increase. Data from Norway show rates dropping in both sexes after age 70 years.15 This is in contrast to the majority of adult cancers in which incidence increases exponentially with age.
In many large surveys of uveal melanoma patients, there is a slight predominance of males.2,6,12,16,29 Higher rates in males have been reported in many studies that presented gender-specific rates of ocular melanoma. Higher rates in males have also been found in studies that used all eye cancers in persons aged 15 years or older as a surrogate for ocular melanomas.22,23,25 It has been shown in white populations that over 90% of these eye cancers are ocular melanomas22 with the majority involving the uveal tract.3 In New England, however, the overall rate during a 6-year period was similar in males and females.8 Age-specific incidence rates were 2.3 per million for persons aged 15–44 years, 15 per million for persons aged 45–64 years, and 25.3 per million for persons aged 65 years and older.
Race and ancestral origin
Uveal melanoma is rare in nonwhite races. Data from the Third National Cancer Survey indicate that in the USA, whites have more than eight times the risk of developing the disease than blacks.3 The New England incidence survey data for a 6-year period suggest that the rate among whites is 9.4 times that of African Americans.8 A recent analysis of population-based registry data in the Surveillance Epidemiology and End Results (SEER) program30 found a relative risk of ocular melanoma for white males compared with African American males of 7.4; the risk for white women in comparison with African American women was 53. Surveys of eye disease in African populations reveal the same low risk in black Africans.18–21 The risk of uveal melanoma is also low among Chinese, Japanese, and Thais.31–33 In the USA, the disease is rare among Americans of Asian extraction.3 A series of three posterior uveal melanomas in Vietnamese Asians with clinical and cytogenetic characteristics was reported recently by McCannel et al.34 The small number of cases reported among Native Americans and Hispanics in the USA suggests that this diagnosis is also rare in these groups. Two cases of ocular melanoma among south-western Native Americans were found in a review of the New Mexico tumor and melanoma registries,35 and one report described four Native Americans with choroidal melanoma evaluated for the Collaborative Ocular Melanoma Study.36 A series of 20 choroidal melanoma patients of Hispanic origin was described by Hudson et al.37
Among whites with uveal melanoma, ancestral origin from more northern latitudes was the strongest risk factor found in a large case–control study.38 Northern European ancestry was associated with more than a sixfold increased risk, and British ancestry was associated with more than a twofold increased risk, as compared with southern European and Mediterranean heritage. The roles of ancestry and race were examined in an evaluation of the incidence of uveal melanoma using data from the Israeli Cancer Registry.17 Jews immigrating to Israel from Europe or North America and Israeli-born Jews had a threefold to fourfold increased incidence compared with Jews from Asia or Africa; non-Jews had the lowest risk.
Cancer genetics
A number of clusters of uveal melanoma occurring among blood relatives have been reported. Familial clusters of uveal melanoma cases have been identified in several large series of patients. Among 1600 patients with uveal melanoma treated by proton beam irradiation over a 10-year period, only 11 families were found to have more than one verified case of the disease.39 In a series of 4500 cases diagnosed between 1976 and 1993, 27 families having at least two blood relatives with an uveal melanoma diagnosis were identified.40 Although the overall incidence among familial cases in that study was small, it was significantly higher than the expected incidence of sporadic cases. Therefore, it was presumed that the familial clustering was associated with inherited genetic or common environmental factors. Nevertheless, most cases are sporadic with no known family history of the disease.
Although family history of uveal melanoma is rare, some cases may have a heritable component. Mutations in G-α proteins, which are believed to be responsible for tumor development have been recently identified in uveal melanoma and may be present in at least 84% of tumors. Among the most common of these somatic G-α protein mutations are GNAQ41 and GNA11,42 which are mutually exclusive. Cutaneous melanoma is now recognized as an inherited disease in as many as 10% of all cases.43 Recent evidence suggests that family members of persons with cutaneous melanoma who have large numbers of dysplastic nevi have several hundred times the risk of developing cutaneous melanoma compared with the general population.43 Reports of cutaneous melanoma and uveal melanoma occurring as double primary malignancies, some in the presence of dysplastic nevi,44–46 and melanomas of both sites occurring among family members,43,46–49 have led to speculation that cutaneous and uveal melanoma may have a common heritable variant. Persons with cutaneous melanoma have been found to be more likely to possess iris nevi50 or have a larger number of iris nevi51 compared with controls. These studies reported similar, although not statistically significant, patterns for choroidal nevi. A potential bias is that the examiners were not masked with respect to the diagnosis of skin melanoma, and nevi may have been more likely to be identified in patients with skin melanoma. There have been no reports of a higher frequency of ocular melanoma among persons with cutaneous melanoma.
The occurrence of bilateral tumors has been suggested as indicative of genetic predisposition to cancer.52 However, few cases of bilateral primary uveal melanoma have been reported,46,52,53 and most reported cases did not exhibit other characteristics associated with genetically inherited cancer predisposition, such as early age of onset or familial clustering of uveal melanoma.52
Although heredity may not play a role in most cases of uveal melanoma, cytogenetic analyses of uveal melanoma tissue have revealed that alterations in chromosomes 3 and 8 may be associated with increased metastasis-related mortality.54–56 Jay and McCartney57 documented an unusual family with eight presumed cases of malignant ocular melanoma spanning four generations; mutations in the p53 tumor-suppressor gene were detected in the two tumors for which preserved material was available. Application of molecular genetic research to uveal melanoma may lead to new insights into the pathogenesis and prognosis of this malignancy.
Ocular and cutaneous nevi and melanocytosis
Nevi on the skin have been shown to increase the risk of cutaneous melanoma.58,59 Similarly, the majority of uveal melanomas are thought by some to arise from pre-existing choroidal nevi.60 However, the available literature suggests that the risk of choroidal and ciliary body melanomas associated with nevi of the uveal tract is low. Ganley and Comstock4 estimated that 3% of the population over the age of 30 years have choroidal nevi posterior to the equator of the eye. Because nevi may also occur anterior to the equator,61 the prevalence of choroidal nevi may be as much as twice that reported. Each year, only 1 in 5000 persons with such nevi develop a melanoma (assuming all melanomas arise from pre-existing nevi).4 Because of the low risks associated with these conditions, current guidelines and recommendations for management and follow-up may not be cost-effective.
Other melanocytic conditions that have been linked to uveal melanoma include ocular (melanosis oculi) and oculodermal (nevus of Ota) melanocytosis. These are typically congenital, unilateral conditions involving hyperpigmentation of the episclera and uveal tract in ocular melanocytosis and of the periorbital skin in oculodermal melanocytosis. Both conditions are more common in females, and the highest prevalence has been reported in Asians.62 Gonder et al.63 found that the prevalence of both forms of melanocytosis was higher in persons with uveal melanoma compared with a clinic population. Singh et al.64 estimated the lifetime prevalence of uveal melanoma in white patients with ocular or oculodermal melanocytosis to be 2.6 cases per 1000 population, as compared with an estimated prevalence of uveal melanoma of 7.5 cases per 10 000 in the general population.
Case–control studies suggest that presence of cutaneous nevi may be a risk factor for uveal melanoma.38,65,66 A significant trend for an increase in the risk of uveal melanoma with more cutaneous nevi was found by Seddon et al.38 Dysplastic nevus syndrome (DNS)41 and atypical mole syndrome65,67 also have been associated with uveal melanoma. In one study, persons with dysplastic nevi were more likely to possess conjunctival, iris, and choroidal nevi.68 Results of a case–control study comparing the presence of DNS in Hungarian patients with uveal melanoma or with cutaneous melanoma and in volunteer controls indicated that DNS was significantly more common in both groups of melanoma patients than in the control group (the odds ratio for uveal melanoma as compared with controls was 4.36).69 Van Hees et al.67 reported a dose–response relationship between number of atypical nevi and uveal melanoma. After adjustment for age and sex, the presence of one or two atypical nevi was associated with nearly a threefold increased risk, and the presence of three or more atypical nevi with a fivefold increased risk of melanoma in comparison with absence of atypical nevi. Similarly, Bataille et al.65 found a trend of increasing odds ratios for greater numbers of atypical nevi. Although DNS and ocular nevi have been linked to risk of uveal melanoma, DNS was not found to be associated with the prevalence of iris or choroidal nevi in a case–control study from Sweden,70 nor was a higher-than-expected rate of dysplastic nevi demonstrated in a group of patients with ocular melanoma evaluated by Taylor et al.71 The association between DNS and uveal melanoma remains controversial.
Hormones and reproductive factors
Hormonal influences are suspected to be a factor in cutaneous melanoma based on reports of an increased risk for women in their childbearing years72,73 and the seemingly adverse influence of pregnancy on prognosis.74–76 Pregnancy may also pose an added risk for uveal melanoma, although reports of presentation77–81 and tumor growth79 during pregnancy are rare. Increases in mortality resulting from tumors of the eye73 and in the incidence of ocular melanomas2 during the childbearing years have been reported. On the other hand, the hormonal environment had no appreciable influence on risk of metastases in younger women with uveal melanoma in one series.82 Potential mechanisms are speculative and include a hormonal effect from estrogens or melanocyte-stimulating hormone. However, one study showed an absence of estrogen receptors in melanoma and surrounding choroidal tissue.79
Epidemiologic studies comparing uveal melanoma cases to controls without melanoma have evaluated hormonal and reproductive factors.83,84 Findings suggest a weak or no association and are not consistent between the two reports. For example, one found an increased risk83 and the other a decreased risk84 for ever having been pregnant. Similarly, increased risk83 and no change in risk84 for use of postmenopausal estrogens were reported. Further studies are needed to evaluate these relationships.
Eye and skin color
Some studies suggest that persons with light irides are at increased risk of developing uveal melanoma.33,66,85 In one of these studies,86 persons with blue or gray eyes were found to have three times the risk of disease (unadjusted for other host factors) compared with persons with brown eyes. In a larger study of over 400 cases that combined melanoma of the iris with other uveal melanomas, the risk for blue-eyed persons was 1.7 times that of persons with brown eyes. Hair and skin color were not found to be independent risk factors after adjusting for eye color.85 Similarly, Holly et al.66 found a twofold risk for lighter eye color. However, in a case–control study with sibling and population-based controls, Seddon et al. found that skin color was significantly associated with uveal melanoma after adjusting for ancestral origin, with a relative risk of 3.8 comparing light to darker skin color among whites with uveal melanoma, but lighter eye color was only weakly related and was not significant in multivariate analyses.38
The iris is the only part of the uveal tract positioned in front of the lens, an effective ultraviolet filter. One study found a higher prevalence of blue and gray eyes among patients with iris melanoma compared with controls with ciliary body and choroidal melanoma.87 Kliman et al.88 also found that light irides were more common in persons with melanocytic lesions of the iris but suggested that such lesions may simply be more noticeable in lighter irides. However, the well-documented tendency for iris melanomas to occur in the inferior sector of the eye,9,12,89–91 where exposure to sunlight is presumably greatest, supports the view that the origin of these iris tumors may be environmentally related.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


