Endoscopic Treatment of Cholesteatoma with Antral Extension
14.1 Introduction
Open tympanoplasty with traditional microscopic approach is widely considered a radical treatment for attical mastoid cholesteatoma; however, it is associated with several negative aspects concerning postoperative quality of life.1
It is common experience that an open cavity will mean inconvenience or discomfort for the patient: a patient who has undergone an open tympanoplasty has to avoid allowing wind or water to enter the external auditory canal, which prevents participation in water sports and other activities; there are often chronic secretions in the new cavity due to its poor aeration, unless a meatoplasty is carried out 1–3; in addition, periodic cleaning of the open cavity is required to avoid infection.
This situation arises because in open tympanoplasty the surgeon has to create a wide mastoid cavity merging the attic and tympanic cavity (▶ Fig. 14.1).2–5
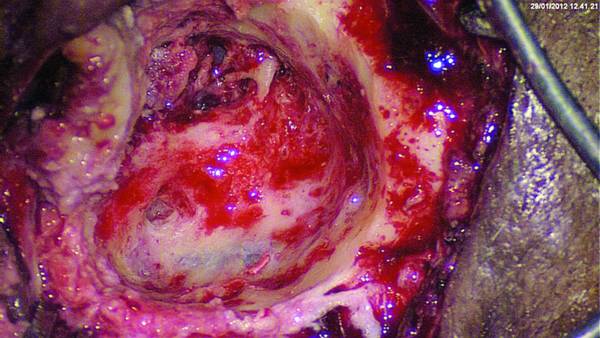
Fig. 14.1 Left ear. Open cavity after canal wall down technique; a wide cavity is created, the attic is confluent with the mastoid. This approach requires a wide meatoplasty in order to achieve optimal cleaning of the new external auditory canal.
14.2 Transcanal Endoscopic “Open” Technique
With this technique the surgeon aims to eradicate the cholesteatoma through a transcanal approach, following the cholesteatoma disease centrifugally, starting from the tympanic cavity toward the antral region.6
This is made possible by drilling of the antral region and the posterior bony wall, obtaining exposure of the mastoid antrum (▶ Fig. 14.2).
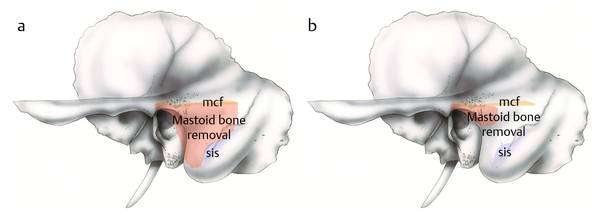
Fig. 14.2 Left temporal bone. a The orange area indicates the removal of mastoid bone during traditional microscopic mastoidectomy. b The orange area here indicates the removal of mastoid bone during the transcanal endoscopic open approach. sis, sigmoid sinus; mcf, middle cranial fossa.
14.3 Indications
Epitympanic cholesteatoma with posterior extension toward the antrum and/or the periantral cells in a sclerotic mastoid (lacking air cells) with or without low middle cranial fossa dura (▶ Fig. 14.3, ▶ Fig. 14.4).6
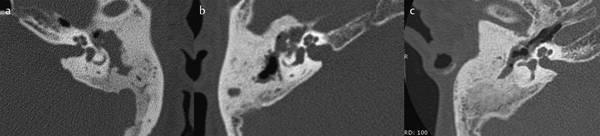
Fig. 14.3 a–c CT, axial views of the temporal bone in patients affected by attic cholesteatoma with antrum involvement without mastoid air cells.
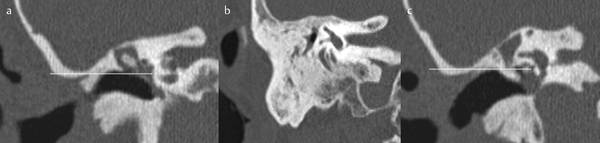
Fig. 14.4 CT, coronal views of the temporal bone showing attic-mesotympanic cholesteatoma with antral involvement. The dura of the middle cranial fossa is low (white line; a, c); this anatomical condition does not allow a microscopic closed technique. Mastoid air cells are absent (b).
14.4 Contraindications
Cholesteatoma with extension to mastoid cells in a well-pneumatized mastoid.6
The advantage of the transcanal approach is to remove only as much bone as is necessary to obtain the space to eradicate the cholesteatoma, producing an antrum-attic tympanic cavity of limited dimensions that can be self-cleaning, thus avoiding meatoplasty (▶ Fig. 14.5).
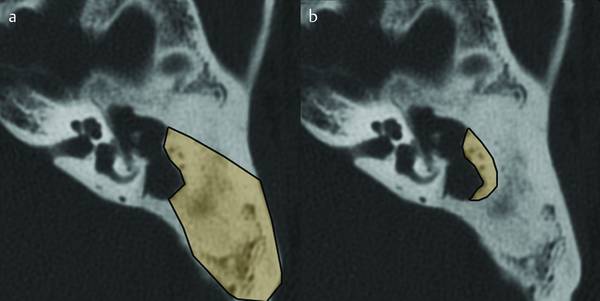
Fig. 14.5 CT, axial view. a The yellow area indicates the removal of mastoid bone during traditional microscopic mastoidectomy. b The yellow area here indicates the removal of mastoid bone during the transcanal endoscopic open approach.
When reconstruction of the posterior wall is attempted, drilling should remove just the lateral bony wall of the antrum and periantral regions, preserving the mucosa of the medial wall of the antrum. Otherwise, the mucosa will be removed to avoid conflict between the skin of the external auditory canal and the mucosa.
14.5 Surgical Steps
We recommend a 0°, 3-mm-diameter optic; with a wide external auditory canal (EAC), a 4-mm-diameter optic offers a brighter surgical field.
Pledgets soaked with epinephrine solution are placed over the eardrum and in the EAC for 5 minutes. Anesthetic–epinephrine solution is injected in the posterior-superior area of the EAC.
Using a round knife or a molecular resonance knife (Vesalius) or a laser, an incision is made in the EAC (from the 2 o’clock to the 7 o’clock position), keeping about 2 cm away from the fibrous anulus.
A tympanomeatal flap is created and reversed inferiorly and dissected from the malleus (the flap creation phases are the same as described in Chapter ▶ 12). The pledgets are placed between the cutaneous flap and beneath the bony EAC, keeping the surgical field clear of blood and helping in the maneuvers of EAC skin detachment.
The fibrous anulus is identified in its posterior portion and, using a microhook, all adhesions between the anulus and eardrum mucosa are cut to allow entry into the tympanic cavity.
The posterior malleolar ligament is parted and the flap is prepared posteroanteriorly and superoinferiorly until it can be released from the short process and handle of the malleus.
The flap is released in this way from the ossicular structures and from the anterior malleolar ligament and is laid down inferiorly over the EAC (▶ Fig. 14.6). This maneuver provides a wide exposure of the protympanic area, eustachian tube, attic region, and tensor fold region.
Once the tympanomeatal flap has been created, the integrity of the ossicular chain must be assessed carefully as well as the actual extension of cholesteatoma toward the hidden recesses and the ossicular chain itself.
If cholesteatoma involves the lateral attic, moving further inward posteriorly in the antral region, preservation of the ossicular chain will be attempted. In cases of medial extension relative to the ossicular chain with involvement of the medial face of the incudomalleolar joint, removal of the ossicular chain is necessary to allow complete eradication of the cholesteatoma matrix.
With ossicular chain erosion, removal of the incus is appropriate. This allows a wide endoscopic access to the principal anatomical landmarks (the second tract of the facial nerve and the lateral semicircular canal) that aid the surgeon in performing an open transcanal endoscopic approach (▶ Fig. 14.6, ▶ Fig. 14.7, ▶ Fig. 14.8, ▶ Fig. 14.9, see also Clinical case 1 [▶ Fig. 14.10, ▶ Fig. 14.11, ▶ Fig. 14.12, ▶ Fig. 14.13, ▶ Fig. 14.14, ▶ Fig. 14.15]).
After removal of the incus, the head of the malleus is resected, permitting access to the entire medial epitympanum.
After removal of the ossicular chain, the surgeon must continue to pay attention to the stapes superstructure; using a curved dissector, the cholesteatoma over the facial region has to be removed as far as exposure of the second tract of the facial nerve, the cochleariform process anteriorly, and the lateral semicircular canal posteriorly (▶ Fig. 14.16).
Key point: For this step we recommend the use of curved bevel dissectors, avoiding sharp instruments because there could be facial nerve canal dehiscence under the cholesteatoma tissue with the possibility of damaging it.
Detachment of cholesteatoma over the facial nerve region may be helped by use of physiological saline-soaked pledgets placed over the facial nerve and pulled gently to remove the cholesteatoma from the nerve below.
After clear identification of the second tract of the facial nerve and the lateral semicircular canal, wide drilling of the attic and the posterior wall can be undertaken (▶ Fig. 14.17).
The drilling is done using a sharp cutting bur moving anteroposteriorly and inferosuperiorly; this step should occur in a continuously watered field.
The surgeon holds the endoscope with the left hand and the drill with the right hand; the anatomical landmarks to note are the tegmen tympani, considered the superior limit, and the mastoid antrum.
This area is located just posteriorly and superiorly to the lateral semicircular canal and can also be evaluated at the beginning of the drilling, using a 45° endoscope (▶ Fig. 14.18, see also Clinical case 2, all figures). During the drilling, the tympanic facial nerve and the lateral semicircular canal prominence are in front of the surgeon and under endoscopic control, permitting safe drilling (see Clinical case 2 [▶ Fig. 14.20, ▶ Fig. 14.21, ▶ Fig. 14.22]).
The lateral semicircular canal prominence is exposed under direct endoscopic control and the scutum and the posterosuperior EAC bony wall are pulled down, creating a confluence of the antrum and tympanic cavity (see Clinical case 3).
At the end of this step, the cholesteatoma sac is removed from the antral region with curved instruments and under 45° endoscope control to achieve a radical removal (▶ Fig. 14.32, ▶ Fig. 14.33, ▶ Fig. 14.34).
After removal of the cholesteatoma, the cavity is checked again to avoid leaving residual disease and to evaluate the cavity created (see Clinical case 2 and Clinical case 3).
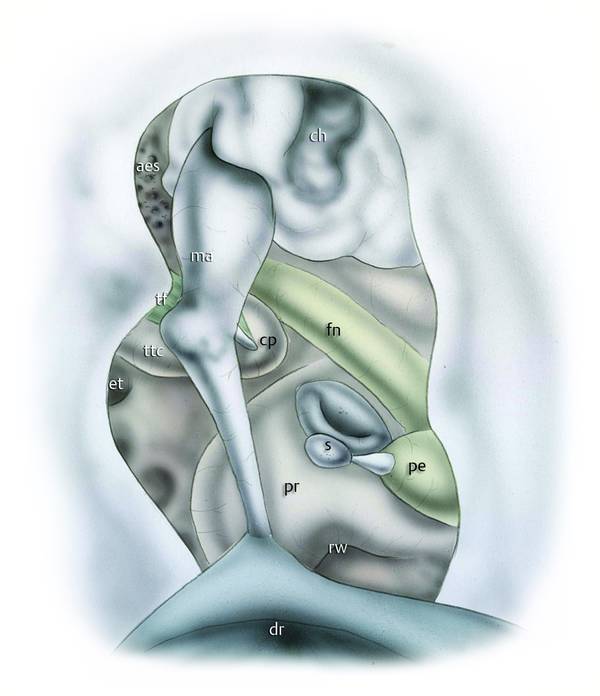
Fig. 14.6 Left ear. Transcanal endoscopic open approach. The tympanomeatal flap has been created; after atticotomy the incus has been removed, exposing the cholesteatoma sac. ma, malleus; cp, cochleariform process; s, stapes; pe, pyramidal eminence; fn, facial nerve; pr, promontory; dr, eardrum; rw, round window; ttc, tensor tympani canal; tf, tensor fold; et, eustachian tube; aes, anterior epitympanic space; ch, cholesteatoma.
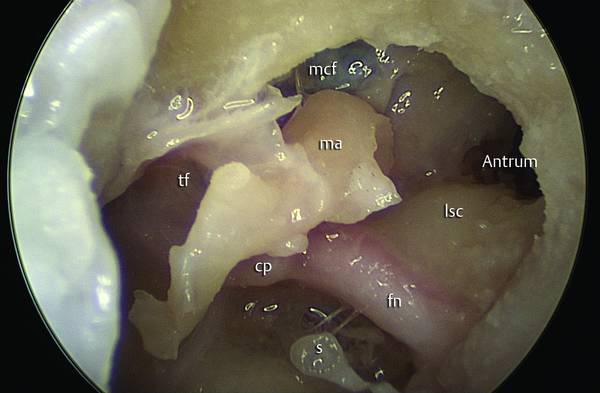
Fig. 14.7 Endoscopic dissection. Left ear. After removal of the incus, a 45° endoscope is used to view the anatomical relationship between the facial nerve, the lateral semicircular canal; and the antrum. ma, malleus; s, stapes; lsc, lateral semicircular canal; mcf, middle cranial fossa dura; cp, cochleariform process; tf, tensor fold; fn, facial nerve.
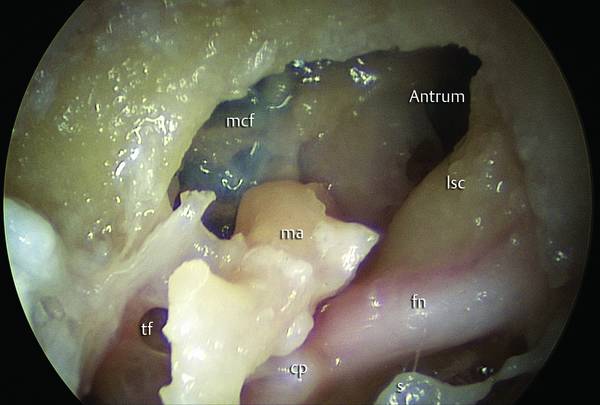
Fig. 14.8 Endoscopic dissection. Left ear. Transcanal endoscopic magnification of the antrum. The antrum is located superiorly and posteriorly with respect to the lateral semicircular canal. ma, malleus; s, stapes; lsc, lateral semicircular canal; mcf, middle cranial fossa dura; cp, cochleariform process; tf, tensor fold; fn, facial nerve.
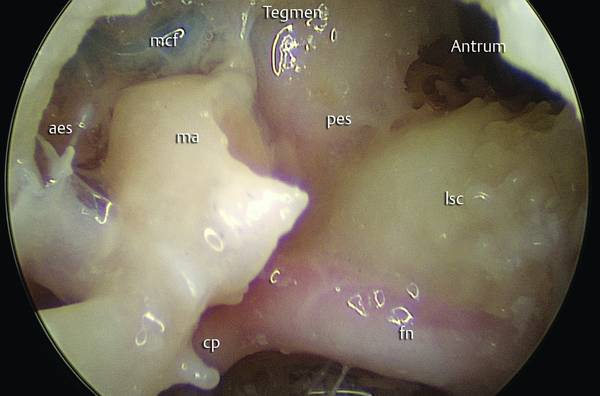
Fig. 14.9 Endoscopic dissection. Left ear. Further advancement of the endoscope into the mastoid antrum. ma, malleus; lsc, lateral semicircular canal; mcf, middle cranial fossa dura; cp, cochleariform process; fn, facial nerve; aes, anterior epitympanic space; pes, posterior epitympanic space.

Fig. 14.10 Clinical case 1. Right ear. Extensive cholesteatoma involving the attic and the mesotympanic spaces, associated with failure of eustachian tube function.
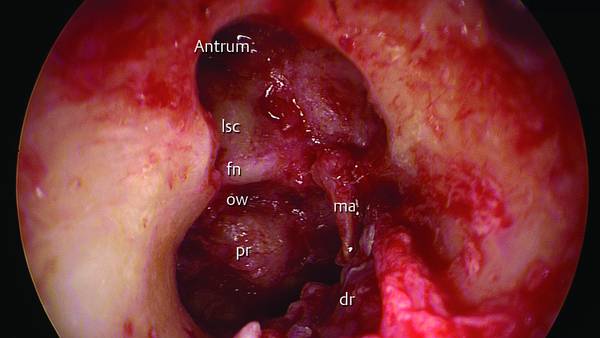
Fig. 14.11 Clinical case 1. Right ear. A transcanal endoscopic open cavity operation is performed. The incus and the superstructure of the stapes were eroded and have been removed; the cholesteatoma has been removed and epidermization of the malleus is present. fn, facial nerve; lsc, lateral semicircular canal; ow, oval window; dr, eardrum; ma, malleus; pr, promontory.
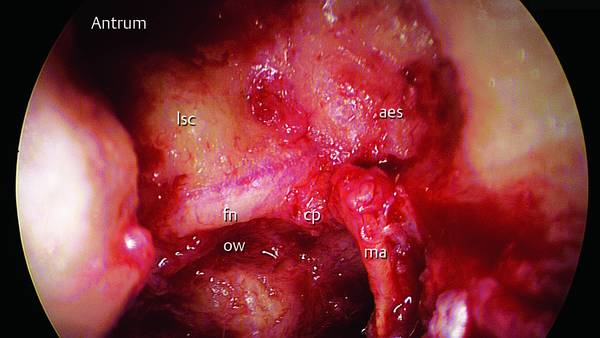
Fig. 14.12 Clinical case 1. Right ear. Magnification of the tympanic facial nerve. The nerve runs just over the cochleariform process, maintaining a close relationship with the lateral semicircular canal superiorly and posteriorly. fn, facial nerve; lsc, lateral semicircular canal; cp, cochleariform process; ma, malleus; aes, anterior epitympanic space; ow, oval window.
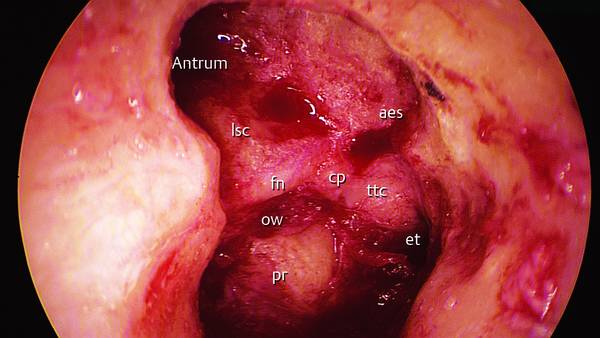
Fig. 14.13 Clinical case 1. Right ear. The handle of the malleus was epidermized and has been removed; the entire anatomical structure lying in the medial wall of the tympanic cavity is endoscopically observable. fn, facial nerve; lsc, lateral semicircular canal; cp, cochleariform process; aes, anterior epitympanic space; et, eustachian tube; ow, oval window; pr, promontory; ttc, tensor tympani canal.
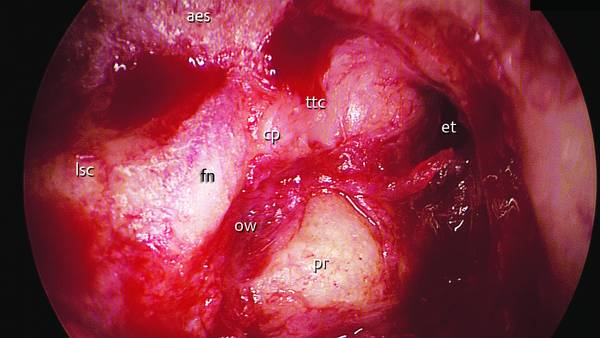
Fig. 14.14 Clinical case 1. Right ear. Endoscopic magnification of the facial nerve. fn, facial nerve; lsc, lateral semicircular canal; cp, cochleariform process; aes. anterior epitympanic space; et, eustachian tube; ow, oval window; pr, promontory; ttc, tensor tympani canal.
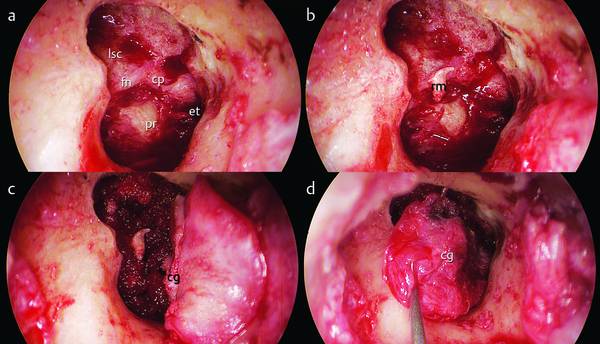
Fig. 14.15 Clinical case 1. Right ear. a, b
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


