Recent significant advances in the development of flexible and rigid endoscopes offer advantages over the traditional otomicroscopes.1,2 The first medical use of microscopy in ear surgery was in 1953 and it has played a central role in ear surgery ever since. The merits of otomicroscopy are that it permits binocular vision and two-handed control. The demerits are that blind corners cannot be avoided and that bone scraping is necessary to access the surgical field.3
Based on the findings from otoscopy, many efforts have been made to try to differentiate tympanic membrane conditions such as retractions, retraction pockets (RPs), precholesteatomas, and cholesteatomas.1,4 Tos and Poulsen clinically divided Shrapnell’s membrane retractions into types 0 to IV (▶ Fig. 8.1).5 Attic cholesteatoma was defined by them as a deep RP, the bottom of which could not be seen in otoscopy. Tos also defined precholesteatoma as a deep RP filled with debris, which, as long as the bottom of the retraction is visible in otomicroscopy and the debris can be cleaned by suction, is not a cholesteatoma. These definitions were made by otomicroscopic assessment.
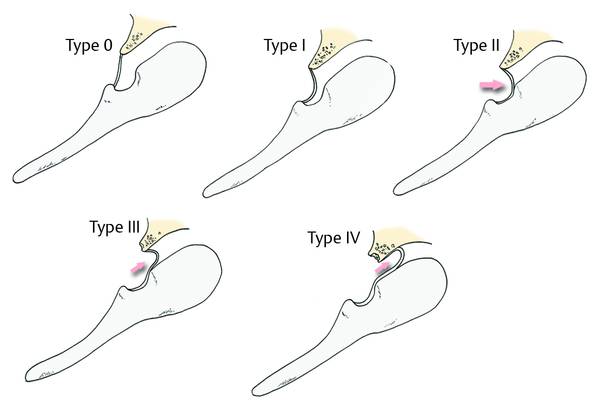
Fig. 8.1 Retraction pocket classification in accordance with Tos and Poulsen.
The visibility of an attic RP with an otomicroscope is limited by the optical characteristics (▶ Fig. 8.2).
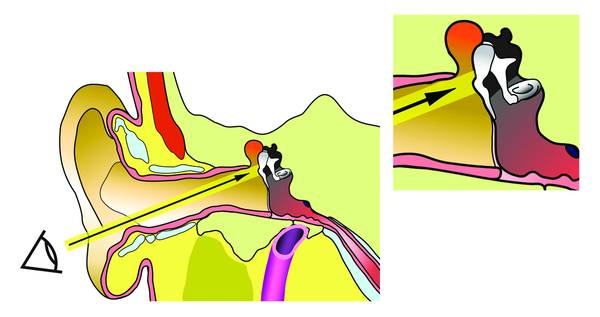
Fig. 8.2 These illustrations show the visibility of the attic RP with an otomicroscope. The range of visibility is limited due to the optical characteristics.
The growth routes of cholesteatomas follow the characteristic pathways of the local anatomical structures.6 Surrounding mucosal folds, ossicular suspensory ligaments, and the ossicles compartmentalize the middle ear into various spaces and pouches. The tympanic diaphragm, a series of mucosal folds and ossicular suspensory ligaments, is believed to resist the spread of the cholesteatoma to the adjacent space.7–9
To inspect retractions of the tympanic membrane we use a fine high-resolution rigid microendoscope, a fine rigid otoendoscope, and/or a digital videoscope. Visibility with endoscopes differs depending on the angle of the endoscope. The visibility of the RP with a 30° endoscope is wider than that with an otomicroscope (▶ Fig. 8.3).
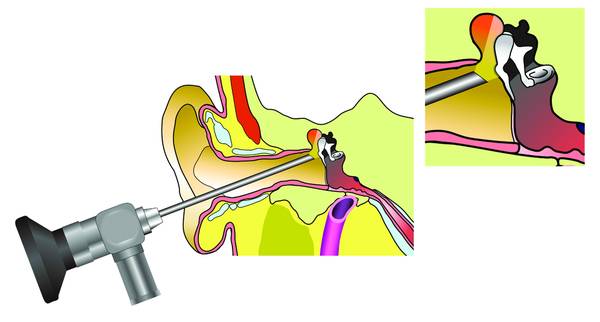
Fig. 8.3 A 30° endoscope is used to provide a wide view of the RP into the attic.
In conclusion, we have found the microendoscope, fine rigid endoscopes, and the videoscope to be useful tools for preoperative assessment of both pars flaccida and pars tensa retraction pockets.10–12
8.2 Methods
For endoscopy, fine rigid endoscopes with 0°, 30°, or 70° views (1.9 mm in outer diameter; Storz, Tuttlingen, Germany) (▶ Fig. 8.4) or 0°, 30°, or 90° view (1.7 mm in outer diameter; Olympus, Tokyo, Japan) were used. Images were delivered to a monitor through an HD CCD camera (Storz, Tuttlingen, Germany or Striker, Santa Clara, CA, USA) attached to the endoscope lens, and recorded.

Fig. 8.4 Rigid endoscopes with (from the top down) 0°, 30°, or 70° views.
The videoscope, equipped with distal sensor video chips, offers better optical resolution, contrast, and color differentiation (▶ Fig. 8.5). The high quality of the digital image is maintained. The wide 90° angle view and narrow width of 3.9 mm enables easy assessment of the whole tympanic membrane.
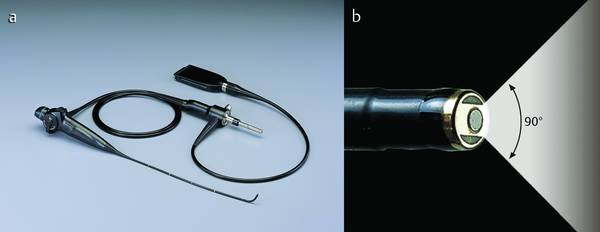
Fig. 8.5 a, b The flexible videoscope, equipped with distal sensor video chips (a). The tip of the instrument (b).
The outer diameter of the microendoscope is 0.9 mm and it has a 45° angled tip.
The resolution is 6000 pixels (▶ Fig. 8.6). A microfiberoptic endoscope with an outer diameter of 1.0 mm (Polydiagnost, Pfaffenhofen, Germany) was used to inspect the bottoms of retractions of the pars flaccida. It incorporates a thin 600-mm microfiberoptic with 6000 pixels and is enveloped with a working channel by a rigid cannula. The length of the endoscope is 50 mm and it has a 45° angled tip 5 mm in length.
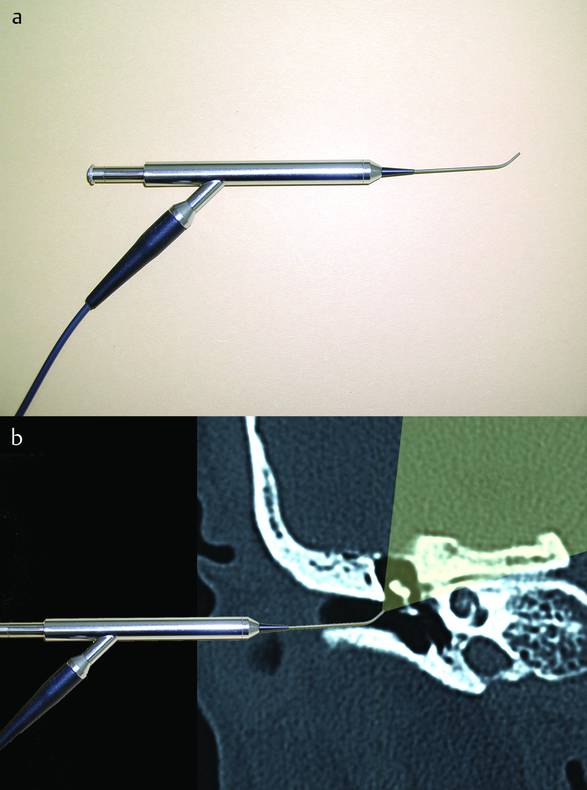
Fig. 8.6 a, b A microfiberoptic endoscope; the angle of the tip allows inspection of the depths of retractions of the pars flaccida.
8.2.1 Endoscopy of Retraction Pockets
Fine Rigid Endoscope
Endoscopy is used in the office setting for inspection of areas of the ear and for evaluation of the condition of RPs. Determination of the depth and existence of cholesteatoma provides benefits for patient consultation as well as for the surgery.
In a case of an RP with a small orifice, the inside of the RP could not be observed with an otomicroscope. With the 30° fine rigid endoscope, the head of the malleus and anterior malleolar ligament were clearly seen. In addition, a close-up view revealed that it extended to the medial attic through an anterior route (▶ Fig. 8.7
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


