Primary acquired cholesteatoma
Secondary acquired cholesteatoma
Congenital cholesteatoma.
According to several studies on the histology of cholesteatoma, we know that congenital, primary, and secondary acquired cholesteatoma have similar histology. Cholesteatoma is a cystlike structure composed of keratinizing squamous epithelium (matrix) that contains epithelial keratin debris and a subepithelial connective tissue. The pathogenesis of cholesteatoma remains incompletely understood. From recent studies with endoscopic techniques new theories about the genesis of the primary acquired cholesteatoma in the attic region can be postulated.
10.1.1 Primary Acquired Cholesteatoma
Primary acquired cholesteatoma is subcharacterized into two classes:
Attic cholesteatoma (which represents the most frequent form). This originates from progressive pars flaccida retraction within the epitympanic sectors due to selective dysventilation of the attic that is characterized by a normal pars tensa of the eardrum with normal ventilation of the mesotympanum (▶ Fig. 10.1).1–4

Fig. 10.1 Right ear. Attic cholesteatoma; endoscopic view.
Mesotympanic cholesteatoma. This originates from retraction of the pars tensa mesotympanic sectors and is often associated with eustachian tube dysfunction (in which case, total retraction of the pars tensa is evident and pars flaccida retraction may be associated) (▶ Fig. 10.2, ▶ Fig. 10.3). It may also be caused by scar tissue (which creates a mucosal fold) secondary to previous middle ear otitis; these folds exclude the mesotympanic spaces from the normal ventilation pathways. This clinical scenario is characterized by a selective pars tensa retraction, specifically in the retrotympanic and the hypotympanic areas (▶ Fig. 10.4, ▶ Fig. 10.5).5–7

Fig. 10.2 Primary acquired cholesteatoma of the left ear. Mesotympanic cholesteatoma in a patient with eustachian tube failure.
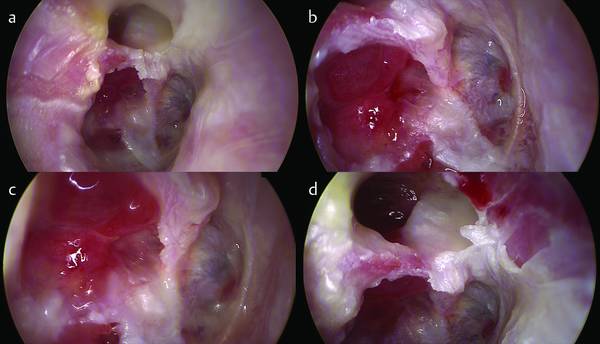
Fig. 10.3 Primary acquired cholesteatoma of the right ear. Overall view (a). Mesotympanic cholesteatoma in a patient with eustachian tube failure with retrotympanic (b) and epitympanic involvement (d). A closer view of retrotympanic involvement (c).
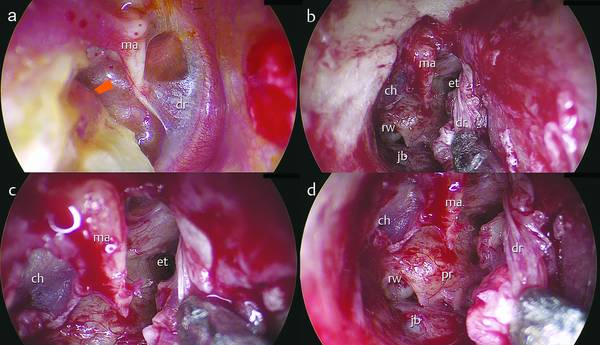
Fig. 10.4 Right ear. a Mesotympanic cholesteatoma in a patient with a selective pars tensa retraction of the retrotympanum (orange arrow). b Transcanal endoscopic approach: a tympanomeatal flap is made, entering the tympanic cavity. c The eustachian tube is detected, the protympanic mucosa is well ventilated. d The cholesteatoma retraction has involved the oval window and the retrotympanum. ma, malleus; ch, cholesteatoma; rw, round window; jb, jugular bulb; et, eustachian tube; dr, eardrum; pr, promontory.
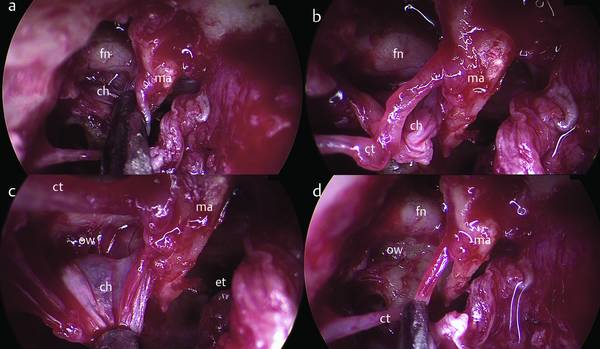
Fig. 10.5 Right ear. Mesotympanic cholesteatoma. a, b The superior limit of the cholesteatoma sac is removed from the facial nerve endoscopically, using a suction instrument. c, d The endoscopic magnification of the sac allows the removal of the pathological tissue from the retrotympanum. ma, malleus; ch, cholesteatoma; ow, oval window; et, eustachian tube; ct, chorda tympani; fn, facial nerve.
10.1.2 Secondary Acquired Cholesteatoma
The etiology of this cholesteatoma is based on previous eardrum perforation subsequent to middle ear otitis. The eardrum perforation is located marginally and may or may not involve the annulus.8 This condition predisposes to the skin migration in the middle ear that progressively creates the matrix of the cholesteatoma (▶ Fig. 10.6, ▶ Fig. 10.7).
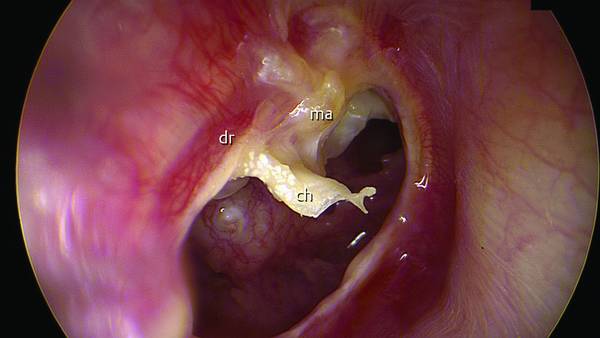
Fig. 10.6 Right ear. Secondary acquired cholesteatoma. ch, cholesteatoma; dr, eardrum; ma, malleus.
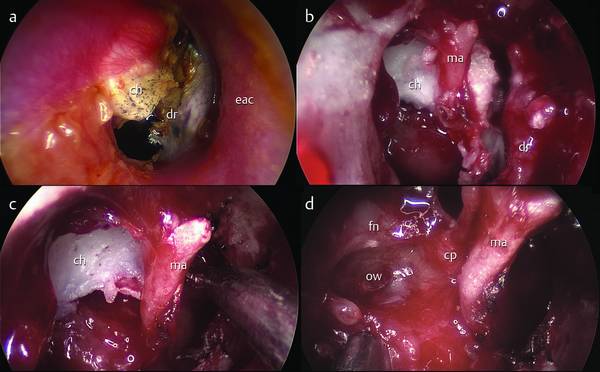
Fig. 10.7 Right ear. Secondary acquired cholesteatoma. A transcanal endoscopic approach was performed. a Aspect of the eardrum before surgery. b, c After performing the tympanomeatal flap, the infiltrative matrix of the cholesteatoma is endoscopically detected. d The oval window after removal of cholesteatoma from the tympanic cavity. ma, malleus; ch, cholesteatoma; ow, oval window; fn, facial nerve; cp, cochleariform process; dr, eardrum, eac, external auditory canal.
10.1.3 Congenital Cholesteatoma
The etiology of this remains controversial but the epithelial rest theory is most commonly accepted. This is a congenital pearly white mass medial to an intact tympanic membrane, a normal pars tensa and flaccida, and no history of otorrhea, tympanic membrane perforation, or previous otological procedures.9–11
10.2 General Indications
10.2.1 Indications and Contraindications
Indications for Transcanal Exclusively Endoscopic Approach Surgery12–15 (▶ Fig. 10.8)
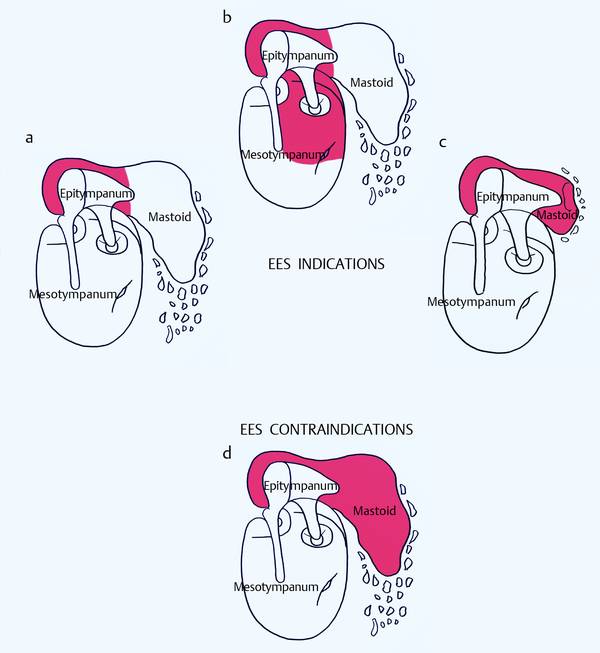
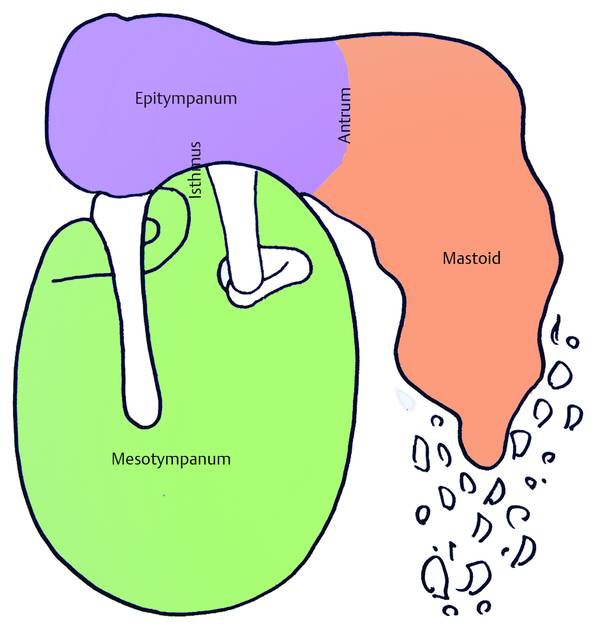
Fig. 10.8 Schematic drawings showing possible indications for endoscopic ear surgery (EES) on the basis of the location of the pathology. Areas in red represent the extension of the disease into the tympanic cavity. a Limited attic cholesteatoma. b Cholesteatoma involving the tympanic cavity with no mastoid cell involvement. c Attic cholesteatoma with extension to the antrum and periantral cells in a patient with a small mastoid with a poor air cell system (in this case a transcanal endoscopic open approach is indicated). d Contraindication: cholesteatoma with involvement of the mastoid air cells (in this case a microscopic approach is required).
Primary or secondary acquired cholesteatoma involving the tympanic cavity (mesotympanic and epitympanic region) with no antral/mastoid cell involvement (▶ Fig. 10.9, ▶ Fig. 10.10, ▶ Fig. 10.11, ▶ Fig. 10.12, ▶ Fig. 10.13, ▶ Fig. 10.14, ▶ Fig. 10.15, ▶ Fig. 10.16)
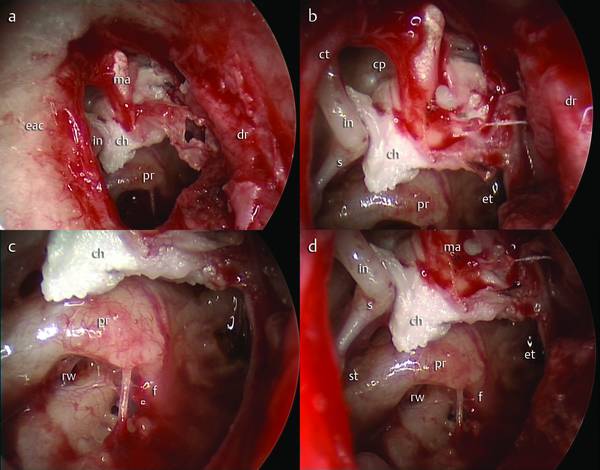
Fig. 10.9 Secondary acquired cholesteatoma involving the tympanic cavity with no mastoid cell involvement. Transcanal endoscopic approach. Right ear. a A tympanomeatal flap is made. b–d The extension of the cholesteatoma into the tympanic cavity is endoscopically detected with respect to the eustachian tube, round window, and isthmus. ma, malleus; ch, cholesteatoma; rw, round window; cp, cochleariform process; dr, eardrum; eac, external auditory canal; in, incus; et, eustachian tube; pr, promontory; st, sinus tympani; ct, chorda tympani; s, stapes; f, finiculus.
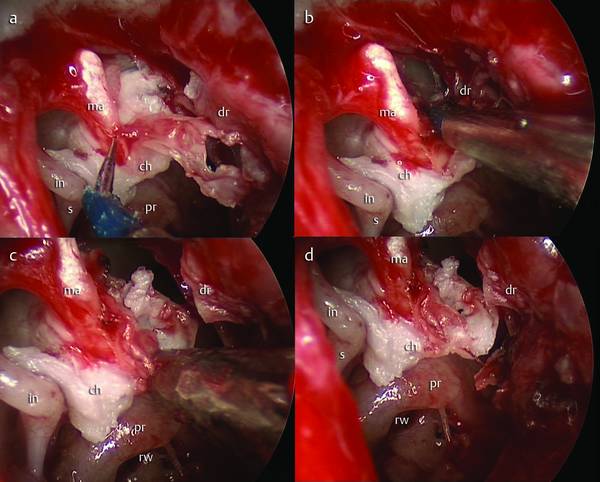
Fig. 10.10 Secondary acquired cholesteatoma involving the tympanic cavity with no mastoid cell involvement. Transcanal endoscopic approach. Right ear. Using the molecular resonance knife (Vesalius), the cholesteatoma is detached from the medial surface of the malleus under endoscopic vision (a–d). ma, malleus; ch, cholesteatoma; rw, round window; dr, eardrum, in, incus; pr, promontory; s, stapes.
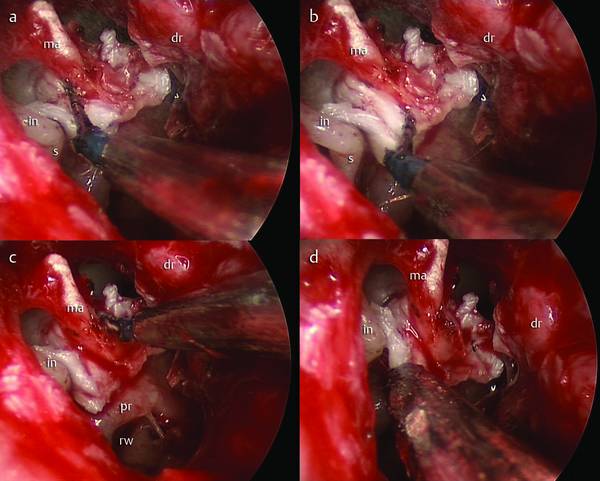
Fig. 10.11 Secondary acquired cholesteatoma involving the tympanic cavity with no mastoid cell involvement. Transcanal endoscopic approach. Right ear. a, b Dissection of the matrix of the cholesteatoma by molecular resonance knife. c, d The cholesteatoma is progressively detached from the ossicles and transposed inferiorly with the use of a suction instrument. ma, malleus; rw, round window; dr, eardrum; in, incus; pr, promontory; s, stapes.
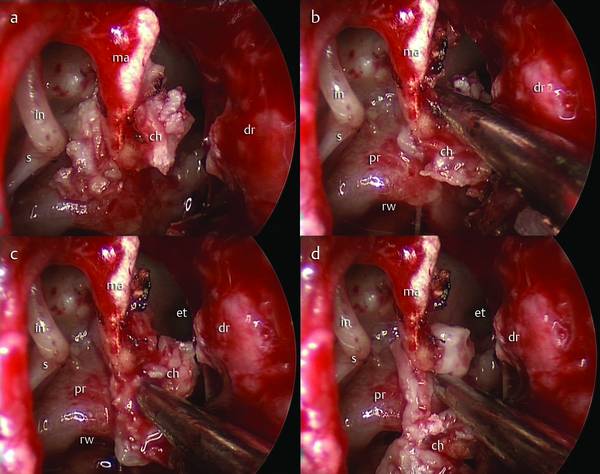
Fig. 10.12 Secondary acquired cholesteatoma involving the tympanic cavity with no mastoid cell involvement. Transcanal endoscopic approach. Right ear. a All the borders of the cholesteatoma are dissected. b–d Using a suction instrument, the cholesteatoma sac is pulled inferiorly. ma, malleus; rw, round window; dr, eardrum; in, incus; pr, promontory; s, stapes; et, eustachian tube; ch, cholesteatoma.
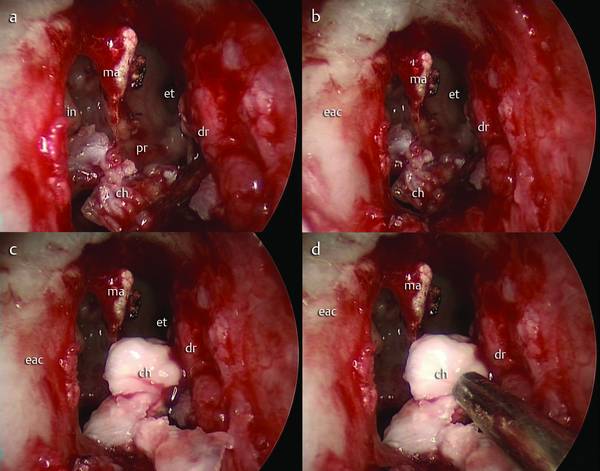
Fig. 10.13 Secondary acquired cholesteatoma involving the tympanic cavity with no mastoid cell involvement. Transcanal endoscopic approach. Right ear. a–c The cholesteatoma sac has been detached en bloc and pulled inferiorly into the external auditory canal. d A suction instrument is used in order to remove the pathological tissue. ma, malleus; dr, eardrum; in, incus; pr, promontory; et, eustachian tube; ch, cholesteatoma; eac, external auditory canal.
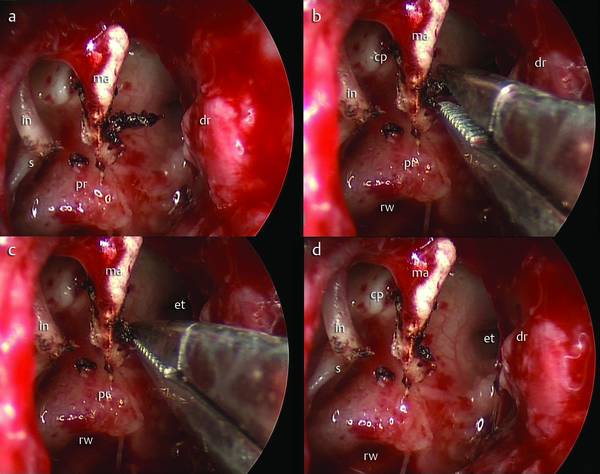
Fig. 10.14 Secondary acquired cholesteatoma involving the tympanic cavity with no mastoid cell involvement. Transcanal endoscopic approach. Right ear. a granulation attached to the handle of the malleus. b, c Removal of granulation using microscissors. d Clean ossicle. ma, malleus; dr, eardrum; in, incus; pr, promontory; et, eustachian tube; cp, cochleariform process; s, stapes; rw, round window.
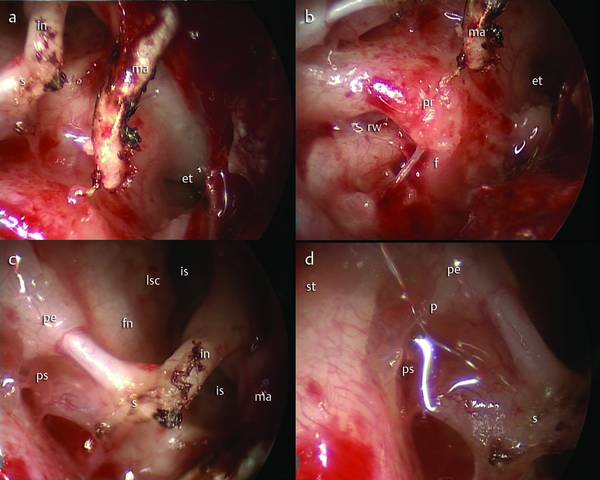
Fig. 10.15 Secondary acquired cholesteatoma involving the tympanic cavity with no mastoid cell involvement. Transcanal endoscopic approach. Right ear. A 45° endoscope is used to check the tympanic cavity, looking for residual disease. a Endoscopic view of the protympanic space. b Endoscopic view of the round window niche. c, d Endoscopic views of the retrotympanum and the isthmus. ma, malleus, in, incus; pr, promontory; et, eustachian tube s, stapes; rw, round window; f, finiculus; st, sinus tympani, ps, posterior sinus; p, ponticulus; pe, pyramidal eminence, fn, facial nerve; lsc, lateral semicircular canal; is, isthmus.
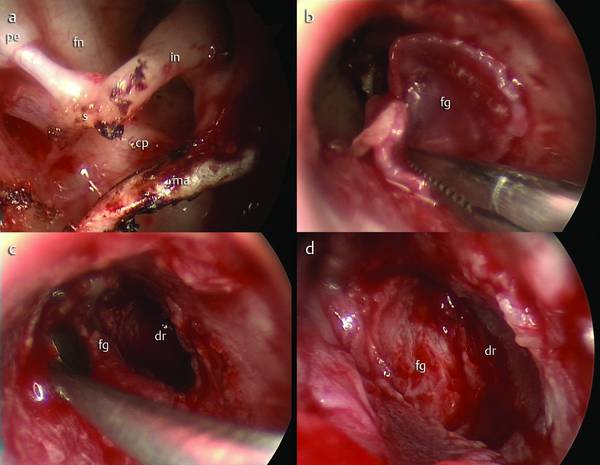
Fig. 10.16 Secondary acquired cholesteatoma involving the tympanic cavity with no mastoid cell involvement. Transcanal endoscopic approach. Right ear. a Final view of the tympanic cavity. b–d The eardrum is constructed with a temporal fascia graft in underlay. dr, eardrum; fg, temporal fascia graft; ma, malleus; in, incus; cp, cochleariform process; fn, facial nerve; pe, pyramidal eminence.
Attic cholesteatoma with no antral/mastoid cell involvement
Retrotympanic cholesteatoma and/or protympanic cholesteatoma and/or hypotympanic cholesteatoma with no antral/mastoid cell involvement
Selective and progressive eardrum attic retraction
Selective pars tensa retraction
Congenital cholesteatoma involving the attic or mesotympanic compartments with no antral/mastoid cell involvement (▶ Fig. 10.17, ▶ Fig. 10.18, ▶ Fig. 10.19, ▶ Fig. 10.20, ▶ Fig. 10.21, ▶ Fig. 10.22, ▶ Fig. 10.23, ▶ Fig. 10.24).
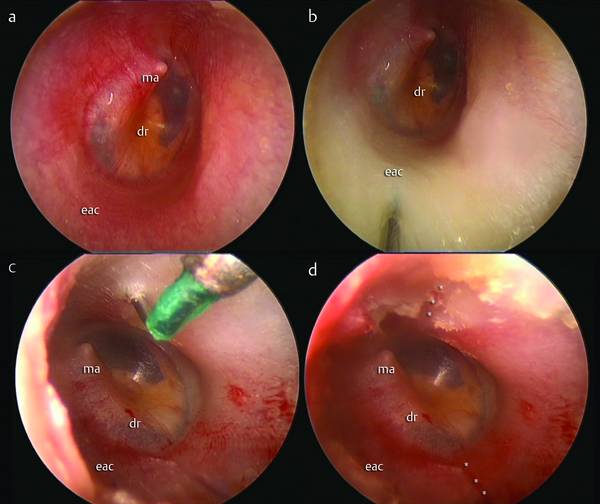
Fig. 10.17 Congenital cholesteatoma. Right ear. Transcanal endoscopic approach. a Aspect of the eardrum before surgery. b Injection of epinephrine solution into the external auditory canal. c, d Two incisions (asterisks) of the external auditory canal are made, at the 7 o’clock and 2 o’clock positions. dr, eardrum; ma, malleus; eac, external auditory canal.
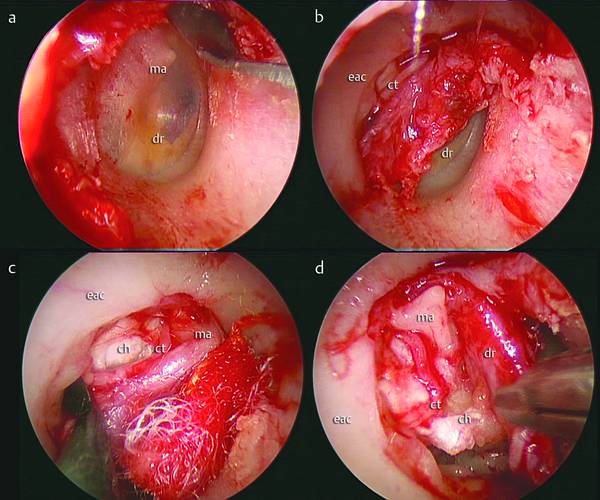
Fig. 10.18 Congenital cholesteatoma. Right ear. Transcanal endoscopic approach. a A circular incision is made with a round knife. b The tympanomeatal flap is elevated; on elevating the anulus, the chorda tympani is visible. c, d The eardrum is transposed anteriorly and inferiorly, detaching the cholesteatoma sac from its medial surface. dr, eardrum; ma, malleus; eac, external auditory canal; ch, cholesteatoma; ct, chorda tympani.
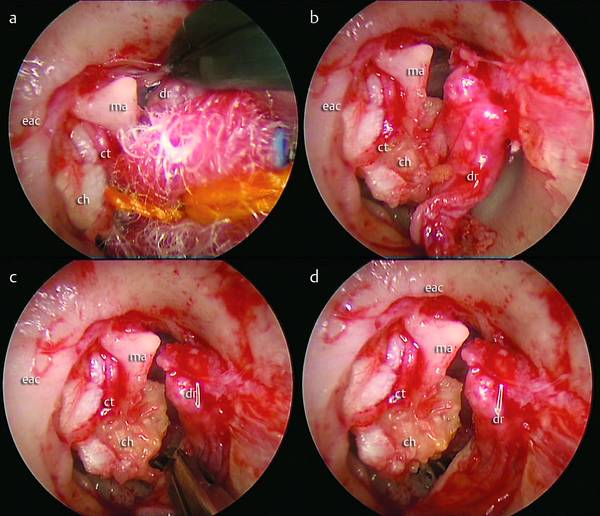
Fig. 10.19 a–d Congenital cholesteatoma. Right ear. Transcanal endoscopic approach. The eardrum is detached from the malleus and transposed anteriorly in order to have wide access to the tympanic cavity. The cholesteatoma sac is completely exposed, the matrix is located medially with respect to the ossicles, involving the oval window. dr, eardrum; ma, malleus; eac, external auditory canal; ch, cholesteatoma; ct, chorda tympani.
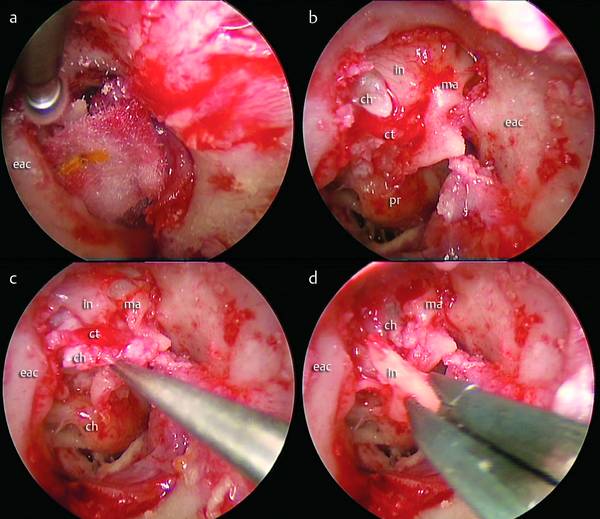
Fig. 10.20 Congenital cholesteatoma. Right ear. Transcanal endoscopic approach. a A drill is used to partially remove the scutum. b Erosion of the incus is visible; the cholesteatoma sac is located medially to the ossicular chain, involving the epitympanum superiorly. c, d The incus is removed to provide a direct view of the cholesteatoma sac. ma, malleus; eac, external auditory canal; ch, cholesteatoma; ct, chorda tympani; in, incus; pr, promontory.
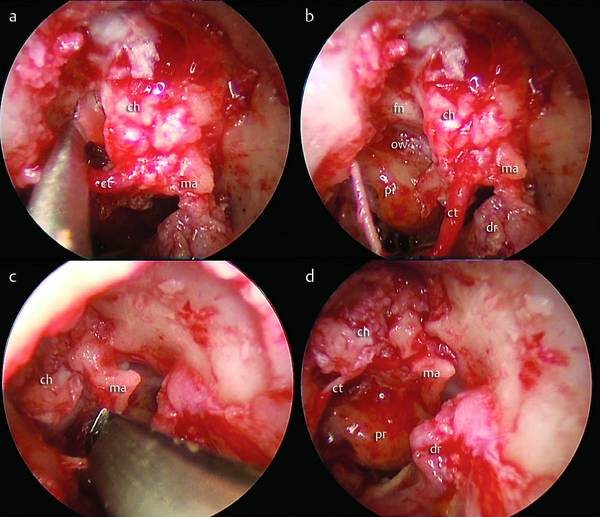
Fig. 10.21 Congenital cholesteatoma. Right ear. Transcanal endoscopic approach. a, b The posterior limit of the cholesteatoma is detected and dissected; the sac is pulled anteriorly, dissecting the cholesteatoma matrix from the tympanic facial nerve and from the oval window. c, d The head of the malleus is cut and removed. ma, malleus; ch, cholesteatoma; ct, chorda tympani; pr, promontory, dr, eardrum; fn, facial nerve; ow, oval window.
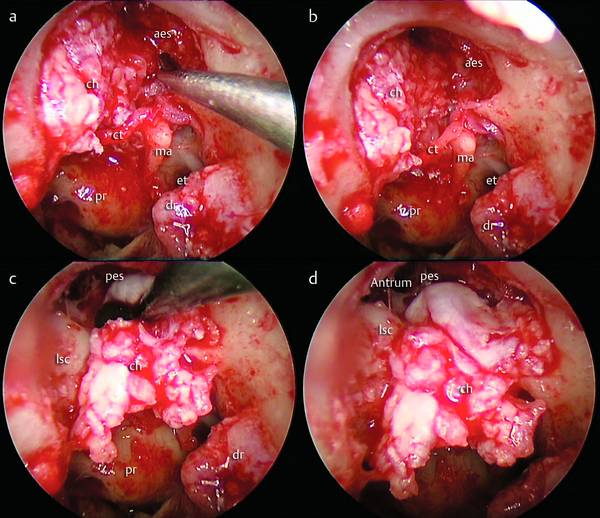
Fig. 10.22 Congenital cholesteatoma. Right ear. Transcanal endoscopic approach. a, b The anterior limit of the cholesteatoma is gently dissected from the anterior bony wall of the attic. c, d A dissector is used to dissect the cholesteatoma sac from the antrum, pulling the cholesteatoma inferiorly. ma, malleus; ch, cholesteatoma; ct, chorda tympani; pr, promontory, dr, eardrum; et, eustachian tube; lsc, lateral semicircular canal; pes, posterior epitympanic space; aes, anterior epitympanic space.
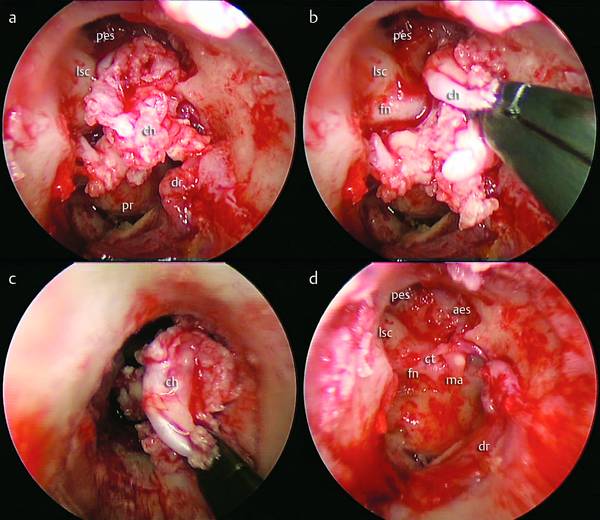
Fig. 10.23 Congenital cholesteatoma. Right ear. Transcanal endoscopic approach. a, b The entire cholesteatoma is isolated and dissected. c The cholesteatoma is removed from the tympanic cavity en bloc. d Endoscopic view of the final tympanic cavity. ma, malleus; ch, cholesteatoma; ct, chorda tympani; pr, promontory, dr, eardrum; lsc, lateral semicircular canal; pes, posterior epitympanic space; aes, anterior epitympanic space; fn, facial nerve.
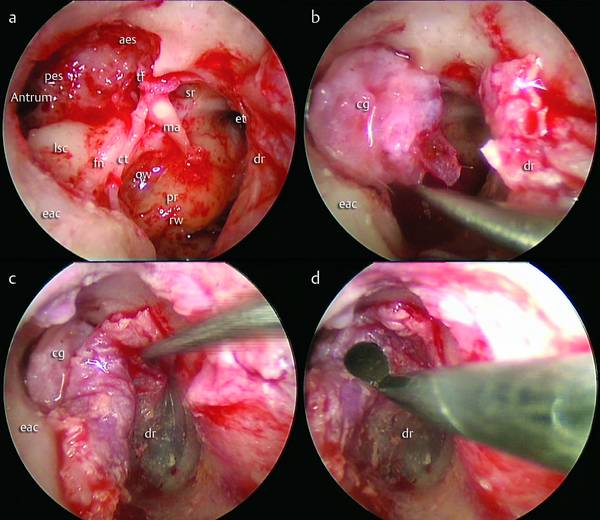
Fig. 10.24 Congenital cholesteatoma. Right ear. Transcanal endoscopic approach. a, b The reconstruction of the scutum is made with a cartilage graft. c, d The tympanomeatal flap is repositioned over the cartilage and over the external auditory canal. In this case a second look after a year is necessary for an ossiculoplasty. ma, malleus, ct, chorda tympani; pr, promontory, dr, eardrum; lsc, lateral semicircular canal; pes, posterior epitympanic space; aes, anterior epitympanic space; fn, facial nerve; rw, round window; ow, oval window; cg, cartilage graft; et, eustachian tube; tf, tensor fold; sr, supratubal recess; eac, external auditory canal.
Contraindications
Mastoid cholesteatoma
Lateral semicircular canal fistula
Dehiscence or fistula of the dura mater
Small external auditory canal.
The transcanal endoscopic approach enables good control of the whole tympanic cavity and of the blind areas (retrotympanum, hypotympanum, and protympanum) (▶ Fig. 10.25).16–19 This technique is limited by the anatomical condition of the external ear canal (which should be wide and without any narrow sections) (▶ Fig. 10.26). It is indicated as the first choice for congenital cholesteatoma limited to the tympanic cavity, for mesotympanic primary acquired cholesteatoma with selective pars tensa retraction, and for secondary acquired cholesteatoma limited to the middle ear.
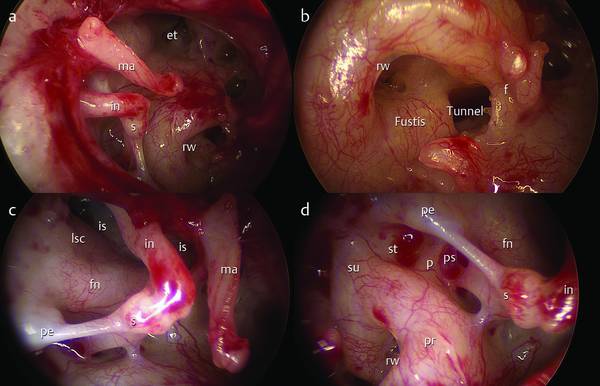
Fig. 10.25 Right ear. a General endoscopic view of the tympanic cavity after elevation of the tympanomeatal flap. b Endoscopic magnification of the round window niche; the round window membrane is exposed and the tunnel is also exposed. c Endoscopic view of the tympanic isthmus and facial nerve. d Endoscopic magnification of the retrotympanum. ma, malleus, in, incus; s, stapes; pr, promontory; lsc, lateral semicircular canal; fn, facial nerve; rw, round window; et, eustachian tube; f, finiculus; st, sinus tympani; pe, pyramidal eminence; su, subiculum; p, ponticulus; ps, posterior sinus; is, isthmus.
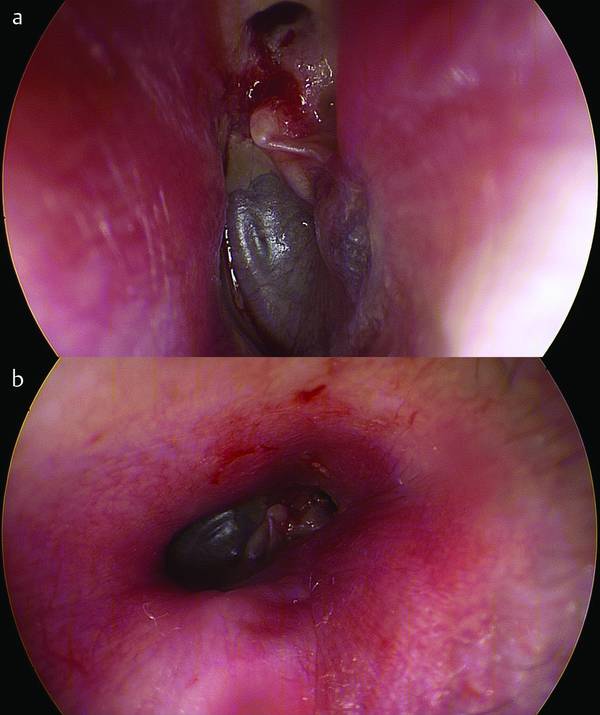
Fig. 10.26 Left ear. Endoscopic analysis of the external auditory canal before surgery in a patient affected by attic cholesteatoma (a). In this patient a narrow external auditory canal (b) can be seen. This anatomical condition represents a relative contraindication for the transcanal endoscopic approach.
These conditions can be managed by transcanal endoscopic approach leading to the complete removal of the pathology via a minimally invasive approach without requiring mastoidectomy and approaching the pathology directly.
A relative contraindications for this kind of approach is the presence of a mesotympanic primary acquired cholesteatoma due to lack of the normal ventilation function of the eustachian tube.
10.2.2 Attic Cholesteatoma
Particular attention needs to be given to this type of cholesteatoma, which is one of the most frequent (14% to 25% of cases). Attic cholesteatoma is the main indication for this type of endoscopic approach because the transcanal approach allows complete removal of the matrix of the cholesteatoma and the restoration of the physiological anatomy of the middle ear, essential to prevent recurrence of further cholesteatoma.
Anatomical and Physiological Considerations for the Transcanal Endoscopic Approach
In physiopathological terms, the middle ear must be considered as three separate compartments linked to each other (▶ Fig. 10.27)20–22: