FIGURE 13.1 OR setup. Operating room organization. Ergonomic setup of the equipment is essential as endoscopic procedures require nondirect tools for visualization (i.e., viewing screens and neuronavigation). The patient’s head is positioned in the center of the operating room, angled slightly away from anesthesia. We use two projection screens to allow direct visualization by both the main operator and the assistant who stand on either side of the bed from each other. This is essential for extended endoscopic cases to avoid the need for either operator to continuously turn their head to see the projection screen. For a right-handed surgeon, the primary surgeon usually stands on the patient’s right side. The navigation system is placed at the head of the bed so both surgeons can view the screen simultaneously.

FIGURE 13.2 OR setup. Photograph of the actual operating room setup taken from the foot of the bed. Note the patient’s head is tilted slightly so the vertex is pointed away from the operating surgeon on the patient’s right side.
Under 0-degree endoscopic view, the inferior, middle, and superior turbinates as well as the sphenoid ostia are identified bilaterally. The middle and superior turbinates are most often retracted laterally; however, in some patients, the middle turbinate is removed to optimize the exposure. A nasoseptal flap is elevated before the posterior septectomy is performed and covers an area extending from the floor of the nasal cavity under the middle turbinate superiorly to the septum adjacent to the nasal roof (Fig. 13.3). The flap is pedicled on the posterior nasal septal artery and is placed out of the way in the nasopharynx until it is needed for the closure.
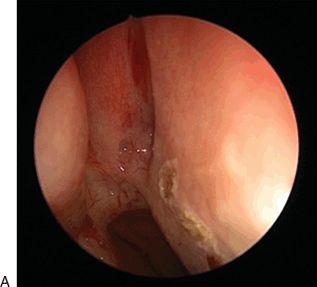
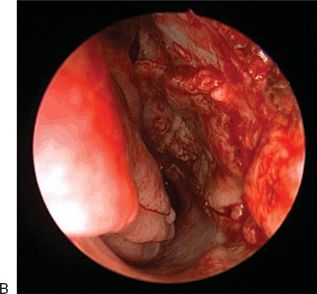

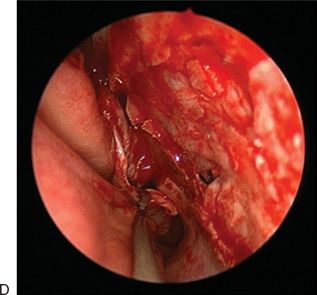
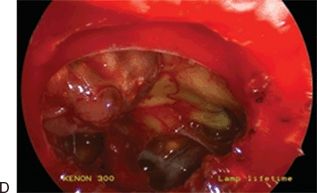
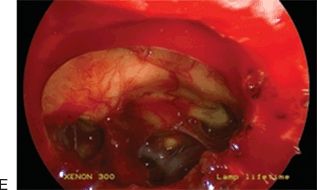
FIGURE 13.3 Harvesting the nasoseptal flap. A. The first incision is made from the choana reaching anteriorly just above the palate along the septum. B. A second incision is made superiorly a few millimeters below the cribriform plate and connected with the inferior incision. C. The flap is mobilized, the pedicle is preserved, and the flap is (D) stored in the nasopharynx until needed.
The ostium of the sphenoid sinus is then enlarged to expose the sphenoid sinus, and the posterior third of the nasal septum adjacent to the vomer and maxillary crest is resected with a tissue shaver. The sphenoid sinus rostrum is fully exposed, and the floor and lateral wall of the sphenoid sinus are drilled down to facilitate placement of the nasoseptal flap at the end of the operation. The keel of the sphenoid is completely removed. All sphenoid septa are removed with a drill, and the mucosa of the sphenoid sinus is completely removed. Bleeding is stopped with either warm saline irrigation or Gelfoam. At this point, a 0-degree, 30-cm rigid 4-mm endoscope is introduced through the left nostril and held in place with a flexible scope holder. The carotid protuberance, optic protuberance, and medial and lateral opticocarotid recesses (LOCRs) are identified. The anterior and lateral extent of the sphenoidotomy are verified using intraoperative neuronavigation ensuring that optimal exposure is obtained in all dimensions before proceeding with progressively deeper exposure. Bilateral posterior ethmoidectomies are performed to adequately visualize the most anterior portion of the PS.
The bone over the tuberculum sellae is initially thinned with a high-speed diamond drill under constant irrigation. The opening extends between the medial opticocarotid recesses (MOCRs), and the inferior extent of the exposure can extend down to the clival recess. The opening is extended anteriorly above the level of the diaphragma sellae, and the PS is removed, the anterior extent of which is determined by using image guidance (Fig. 13.4). If necessary, the bone overlying the medial opticocarotid recess is then drilled using a diamond drill and copious irrigation to thin and remove the bone overlying the optic nerve dural sheaths. The optic nerve dura is unroofed bilaterally, and the bone overlying the carotid prominences is thinned with a drill and removed with Kerrison rongeurs (Fig. 13.4). The location of the carotid arteries is verified using a Doppler ultrasound probe. The dura above and below the superior intercavernous sinus is opened, and the sinus is coagulated and cut just medial to the cavernous sinus bilaterally. The diaphragma sellae is then incised and removed with microscissors. This maneuver is performed during the approach for craniopharyngiomas and macroadenomas. For tuberculum meningiomas, the diaphragm, which is often the site of origin of the tumor, is removed at the end of the operation to ensure a complete resection.
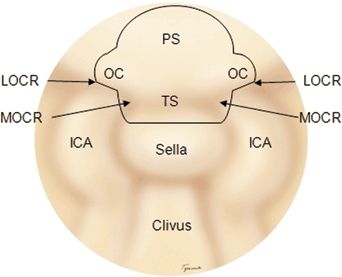
FIGURE 13.4 Bone opening. The bone at the superior aspect of the sella is opened between the MOCR. The tuberculum sellae (TS) and PS are opened with a high-speed drill and Kerrison rongeur depending on the extent of the tumor as determined by navigation and examination of the films. The OCs are opened bilaterally if there is suspicion that the tumor (usually meningiomas) invades into the canal. (ICA, internal carotid artery; LOCR, lateral opticocarotid recess; medial opticocarotid recess; OC, optic canal; PS, planum sphenoidale.)
Large pituitary tumors, meningiomas, and craniopharyngiomas are immediately visualized once the dura is opened. Internal decompression is performed either with two upwardly curved suctions or, if the tumor is firm, with an ultrasonic surgical aspirator, radiofrequency monopolar or ring cautery, or miniaturized microdebrider device as well as with microscissors. Visualization is enhanced with a 30-degree, 30-cm rigid 4-mm endoscope (Karl Storz). Once decompressed, the tumor capsule can be mobilized, and the anterior communicating artery complex and perforators are dissected sharply off of the tumor capsule. Care must be taken to preserve the recurrent artery of Heubner and the subchiasmatic perforating and hypophyseal vessels. The optic nerves and pituitary stalk are identified and dissected off the tumor capsule with preservation of the arachnoid membrane when possible. Avoidance of coagulation and “pulling” are critical to the preservation of vital neurovascular structures while the remaining capsule is removed. The resection bed is examined with a 45-degree, 18-cm rigid 4-mm endoscope to ensure the absence of any residual tumor. Curved suctions, angled micropituitary rongeurs, and dissectors can be used to reach residual pieces of tumor.
Tumor extensions behind the chiasm that extend into the third ventricle are dissected with the view provided by a 0-degree, 30-cm rigid 4-mm endoscope. The solid components are carefully dissected free from the optic chiasm and stalk. Internal decompression facilitates mobilization of the capsule for sharp dissection from the walls of the hypothalamus. It is important to visualize and preserve critical neurovascular structures such as the carotid arteries and hypothalamic and chiasmatic perforators. Once the tumor is partially removed, the location of the stalk may become apparent if it was previously obscured by tumor, and one can safely work on either side of the stalk if the gland is not mobilized. If invasion of the walls of the third ventricle is noted, it may be prudent to leave some wall of the capsule to prevent hypothalamic injury. Once the tumor and cyst wall are completely removed, the resection bed is examined with a 45-degree, 18-cm rigid 4-mm endoscope to ensure the absence of residual tumor. In most cases, the third ventricle ependyma including the foramen of Monro and aqueduct of Sylvius is clearly seen, and contents of the interpeduncular cistern are also apparent (Figs. 13.5 to 13.8).