Sporadic or autosomal dominant with incomplete penetrance
Symptoms
 Gradually decreasing vision, typically beginning in adolescence and progressing into adult life
Gradually decreasing vision, typically beginning in adolescence and progressing into adult life
 Patients often relate a history of not being able to attain good vision despite multiple changes of glasses or soft contact lenses.
Patients often relate a history of not being able to attain good vision despite multiple changes of glasses or soft contact lenses.
 May have a history of eye rubbing
May have a history of eye rubbing
 Can develop acutely decreased vision and pain due to hydrops with advanced disease
Can develop acutely decreased vision and pain due to hydrops with advanced disease
Signs
 Early
Early
 Progressive myopia and astigmatism
Progressive myopia and astigmatism
 Scissors reflex on retinoscopy
Scissors reflex on retinoscopy
 Irregular mires on keratometry
Irregular mires on keratometry
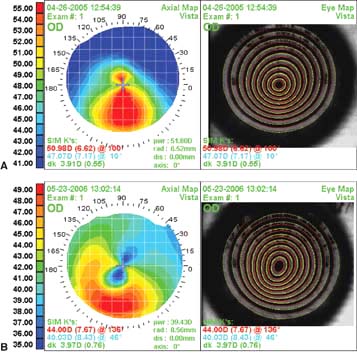
 Inferior steepening on computerized corneal topography (Fig. 4-1A) and tomography. Eyes with “low sagging cones” can demonstrate a mild crab-claw topographic pattern (Fig. 4-1B), which is similar to the pattern seen in pellucid marginal degeneration.
Inferior steepening on computerized corneal topography (Fig. 4-1A) and tomography. Eyes with “low sagging cones” can demonstrate a mild crab-claw topographic pattern (Fig. 4-1B), which is similar to the pattern seen in pellucid marginal degeneration.
 Central or paracentral stromal thinning of the cornea with protrusion at the apex of the thinning (Fig. 4-1C)
Central or paracentral stromal thinning of the cornea with protrusion at the apex of the thinning (Fig. 4-1C)
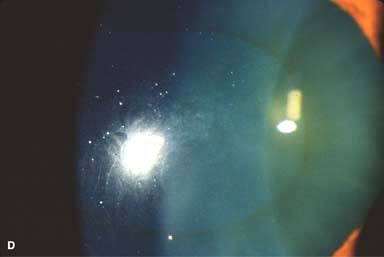
 Fleischer’s ring: epithelial iron deposits at the base of the cone (Fig. 4-1D)
Fleischer’s ring: epithelial iron deposits at the base of the cone (Fig. 4-1D)
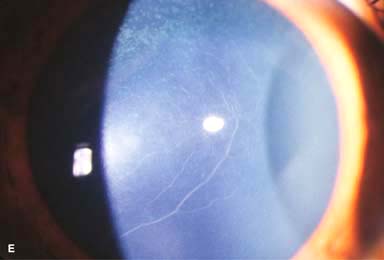
 Prominent corneal nerves (Fig. 4-1E)
Prominent corneal nerves (Fig. 4-1E)
 Late
Late
 Vogt’s striae: fine vertical deep stromal tension lines that disappear temporarily with digital pressure applied to the limbus (Fig. 4-1F)
Vogt’s striae: fine vertical deep stromal tension lines that disappear temporarily with digital pressure applied to the limbus (Fig. 4-1F)
 Abnormal “oil droplet” red reflex
Abnormal “oil droplet” red reflex
 Rizutti’s sign: conical light reflection on the nasal limbus when light is shone from the temporal side
Rizutti’s sign: conical light reflection on the nasal limbus when light is shone from the temporal side
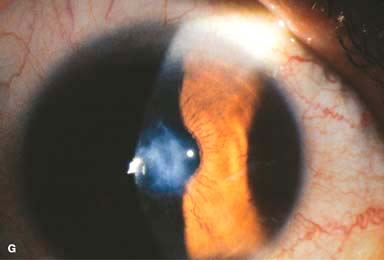
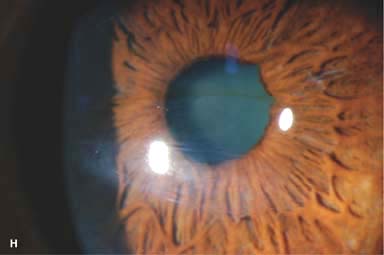
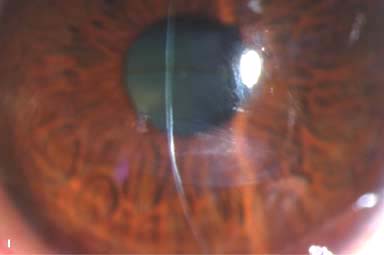
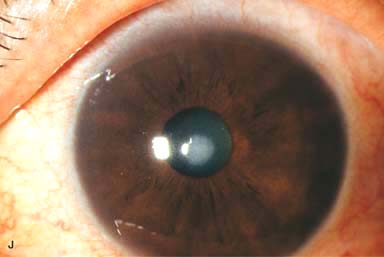
 Variable corneal scarring, depending on severity (Fig. 4-1G–I). May develop an elevated apical nodule (Fig. 4-1J)
Variable corneal scarring, depending on severity (Fig. 4-1G–I). May develop an elevated apical nodule (Fig. 4-1J)
 Munson’s sign: bulging of the lower eyelid in downgaze
Munson’s sign: bulging of the lower eyelid in downgaze
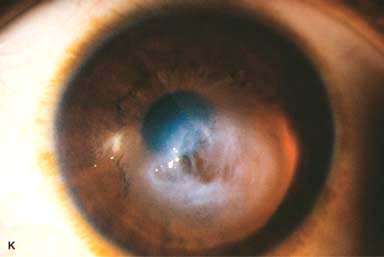
 Acute hydrops: severe corneal edema resulting from a tear in Descemet’s membrane (Fig. 4-1K–M)
Acute hydrops: severe corneal edema resulting from a tear in Descemet’s membrane (Fig. 4-1K–M)
Associations
 Ocular: vernal disease, blue sclera, retinitis pigmentosa, Leber’s congenital amaurosis, floppy eyelid syndrome
Ocular: vernal disease, blue sclera, retinitis pigmentosa, Leber’s congenital amaurosis, floppy eyelid syndrome
 Systemic: Down’s syndrome, Ehlers-Danlos syndrome, Apert’s syndrome, ocular allergies, osteogenesis imperfecta
Systemic: Down’s syndrome, Ehlers-Danlos syndrome, Apert’s syndrome, ocular allergies, osteogenesis imperfecta
Differential Diagnosis
 Pellucid marginal degeneration: inferior peripheral corneal thinning with protrusion of the cornea above the area of maximal thinning
Pellucid marginal degeneration: inferior peripheral corneal thinning with protrusion of the cornea above the area of maximal thinning
Treatment
 Mild cases: glasses and soft contact lenses
Mild cases: glasses and soft contact lenses
 Moderate cases: rigid gas-permeable contact lens (RGPCL), hybrid lens, or scleral lens
Moderate cases: rigid gas-permeable contact lens (RGPCL), hybrid lens, or scleral lens
 Severe and contact lens–intolerant cases:
Severe and contact lens–intolerant cases:
 Lamellar keratectomy with a blade or excimer laser for anterior nodules
Lamellar keratectomy with a blade or excimer laser for anterior nodules
 Placement of intracorneal ring segments
Placement of intracorneal ring segments
 Deep anterior lamellar keratoplasty
Deep anterior lamellar keratoplasty
 Penetrating keratoplasty
Penetrating keratoplasty
 Epikeratoplasty and thermokeratoplasty are rarely performed.
Epikeratoplasty and thermokeratoplasty are rarely performed.
 Refractive surgery in patients with keratoconus is unpredictable and generally not recommended.
Refractive surgery in patients with keratoconus is unpredictable and generally not recommended.
 Corneal collagen crosslinking: Generally performed by placing riboflavin drops on the cornea and then treating the cornea with ultraviolet light, it is being used to “strengthen” the cornea to prevent worsening of keratoconus in patients with documented progression. While not currently FDA-approved, short-term results are promising.
Corneal collagen crosslinking: Generally performed by placing riboflavin drops on the cornea and then treating the cornea with ultraviolet light, it is being used to “strengthen” the cornea to prevent worsening of keratoconus in patients with documented progression. While not currently FDA-approved, short-term results are promising.
Prognosis
 Most patients do well with RGP or hybrid CLs. The success rate with corneal transplantation in keratoconus is high.
Most patients do well with RGP or hybrid CLs. The success rate with corneal transplantation in keratoconus is high.
Figure 4-1. Keratoconus corneal topography. A. Significant irregular inferior corneal steepening is apparent using computerized corneal topographic analysis in this eye with moderate keratoconus. As seen on the color scale on the left, the red colors indicate corneal steepening and blue colors indicate corneal flattening. The figure on the right shows the Placido’s rings; this image is important to verify the quality and centration of the study. B. The irregular inferior steepening seen on computerized corneal topographic analysis of this eye with keratoconus reveals a slight crab-claw pattern, which is reminiscent of pellucid marginal degeneration. Eyes with “low sagging cones” can demonstrate this topographic pattern. Keratoconus.C. Slit-beam view of this eye with significant keratoconus demonstrates inferocentral corneal thinning and steepening. Note the thinnest and most protruded areas of cornea coincide. Keratoconus. D. A prominent Fleischer’s ring, iron pigment deposition at the base of the cone, is present in this eye with keratoconus. E. Prominent corneal nerves can be seen in this eye with keratoconus. These nerves can be distinguished from corneal “ghost” blood vessels because “ghost” vessels have a lumen, making them appear as two parallel lines. Keratoconus. F. Faint, vertical posterior stromal stress lines, Vogt’s striae, are visible at the apex of the cone. Gentle pressure on the limbus can cause these lines to change direction or disappear. G. Significant central stromal scarring is present in this eye with advanced keratoconus. Keratoconus. H. Moderate inferocentral corneal scarring can be seen in this eye after resolution of corneal hydrops. An iron line is visible at the superior edge of the scarring. I. Slit-beam image of the same eye demonstrates significant thinning in the area of scarring. Keratoconus. J. A hypertrophic nodule is present at the apex of the cone. These nodules can occur de novo or related to rigid contact lens wear. Such a nodule can affect vision and/or interfere with comfortable contact lens wear. These nodules can be removed with a superficial keratectomy with a blade or excimer laser phototherapeutic keratectomy (PTK). K. Acute corneal hydrops occurs when the cornea stretches to such a degree that a tear develops in Descemet’s membrane, allowing sudden inflow of aqueous fluid into the corneal stroma. The corneal stroma can swell to greater than five times its normal thickness. Acute hydrops is associated with a sudden decrease in vision and increase in pain. Keratoconus. L. Slit-beam view of the same cornea. Note the severe corneal thickening. A prominent cleft is apparent centrally, where corneal lamellae are separated by a large degree of aqueous fluid. M. Severe corneal whitening from acute corneal hydrops is present. The fellow eye has scarring from previous corneal hydrops (see Fig. 4-1H and I).




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


