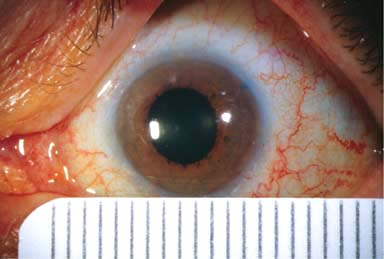
Infant horizontal corneal diameter less than 10 mm; adult horizontal corneal diameter less than 11 mm (Fig. 3-1)
 Shallow anterior chamber, angle-closure or open-angle glaucoma, corneal flattening, and hyperopia
Shallow anterior chamber, angle-closure or open-angle glaucoma, corneal flattening, and hyperopia
 May have associated nanophthalmos (Table 3-1)
May have associated nanophthalmos (Table 3-1)
 Other ocular dimensions are normal.
Other ocular dimensions are normal.
Treatment
 Manage refractive error and search for other ocular and systemic anomalies.
Manage refractive error and search for other ocular and systemic anomalies.
Prognosis
 Varies depending on associated ocular and systemic abnormalities
Varies depending on associated ocular and systemic abnormalities
TABLE 3-1. Association of Microcornea
Figure 3-1. Microcornea. This cornea measured 8.5 to 9.0 mm in diameter. Otherwise the eye was essentially normal.
MEGALOCORNEA
Megalocornea is an uncommon congenital, bilateral condition that is usually inherited in an X-linked recessive manner and is therefore found mostly in males.
Signs
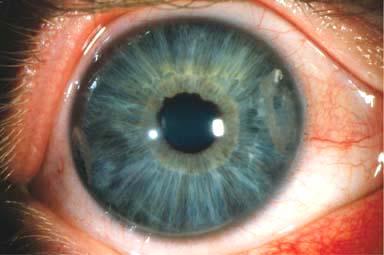
 Clear cornea with a horizontal diameter of greater than 12 mm in the neonate and 13 mm in adults (Fig. 3-2)
Clear cornea with a horizontal diameter of greater than 12 mm in the neonate and 13 mm in adults (Fig. 3-2)
 Very deep anterior chamber
Very deep anterior chamber
 Normal intraocular pressure
Normal intraocular pressure
 Corneal steepening, high myopia, and astigmatism, but good visual acuity
Corneal steepening, high myopia, and astigmatism, but good visual acuity
 Lens subluxation may occur as a result of zonular stretching.
Lens subluxation may occur as a result of zonular stretching.
 May develop glaucoma secondary to angle abnormalities
May develop glaucoma secondary to angle abnormalities
Treatment
 Manage refractive error and search for other ocular and systemic anomalies, especially glaucoma and lens abnormalities.
Manage refractive error and search for other ocular and systemic anomalies, especially glaucoma and lens abnormalities.
Prognosis
 Generally good, but depends on associated ocular and systemic abnormalities (Table 3-2)
Generally good, but depends on associated ocular and systemic abnormalities (Table 3-2)
TABLE 3-2. Associations of Megalocornea
Figure 3-2. Megalocornea. This cornea measured 14 mm in diameter. The cornea is clear except for some calcific degeneration nasally and temporally.
NANOPHTHALMOS
Nanophthalmos is an uncommon, congenital, bilateral condition in which the globe has reduced volume but is otherwise grossly normal.
Signs
 Very high hyperopia (e.g., +12D to +15D)
Very high hyperopia (e.g., +12D to +15D)
 Adult corneal diameter is reduced, but the lens has a normal volume.
Adult corneal diameter is reduced, but the lens has a normal volume.
 Short axial length (e.g., 16–18 mm)
Short axial length (e.g., 16–18 mm)
 Shallow anterior chamber
Shallow anterior chamber
 Thick sclera
Thick sclera
 Fundus may show a crowded disc, vascular tortuosity, and macular hypoplasia
Fundus may show a crowded disc, vascular tortuosity, and macular hypoplasia
Associated Problems
 Angle-closure glaucoma
Angle-closure glaucoma
 Uveal effusion
Uveal effusion
 Retinal detachment
Retinal detachment
 Poorly tolerated intraocular surgery
Poorly tolerated intraocular surgery
MICROPHTHALMOS
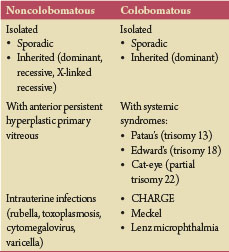
Microphthalmos is an uncommon unilateral or bilateral condition in which the axial length of the eye is reduced and the eye is malformed (Fig. 3-3). The effects on vision depend on its severity and the presence of associated anomalies. There are two types of microphthalmos: noncolobomatous and colobomatous (Table 3-3).
TABLE 3-3. Types of Microphthalmos
 CHARGE syndrome (coloboma, heart anomaly, choanal atresia, retardation, and genital or ear anomalies)
CHARGE syndrome (coloboma, heart anomaly, choanal atresia, retardation, and genital or ear anomalies)
Figure 3-3. Microphthalmos. This microphthalmic eye has a small cornea, abnormal iris, and overall small size. (Courtesy of Peter Laibson, MD.)

BUPHTHALMOS
Buphthalmos is an uncommon, usually bilateral condition in which the globe is enlarged as a result of stretching of the cornea and sclera because of increased intraocular pressure before birth or during the first 3 years of life.
Signs
 Large cornea with variable scarring; may develop corneal edema later in life
Large cornea with variable scarring; may develop corneal edema later in life
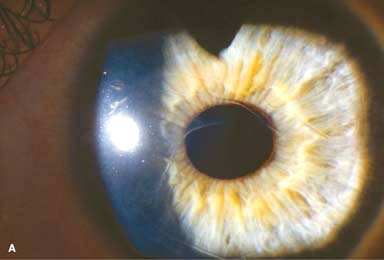
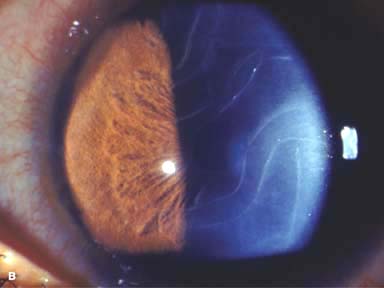
 Horizontal or curvilinear ruptures in Descemet’s membrane (Haab’s striae) (Fig. 3-4)
Horizontal or curvilinear ruptures in Descemet’s membrane (Haab’s striae) (Fig. 3-4)
 Very deep anterior chamber
Very deep anterior chamber
 Angle anomalies
Angle anomalies
 Myopia
Myopia
 Optic disc cupping
Optic disc cupping
Associations of Infantile Glaucoma
 Ocular
Ocular
 Aniridia
Aniridia
 Anterior segment dysgeneses
Anterior segment dysgeneses
 Congenital ectropion uveae
Congenital ectropion uveae
 Systemic
Systemic
 Down’s syndrome
Down’s syndrome
 Lowe’s syndrome
Lowe’s syndrome
 Mucopolysaccharidoses
Mucopolysaccharidoses
 Neurofibromatosis type 1
Neurofibromatosis type 1
 Nevus of Ota
Nevus of Ota
 Patau’s syndrome (trisomy 13)
Patau’s syndrome (trisomy 13)
 Pierre Robin’s syndrome
Pierre Robin’s syndrome
 Rieger’s syndrome
Rieger’s syndrome
 Sturge-Weber syndrome
Sturge-Weber syndrome
Treatment
 Management of glaucoma by a glaucoma specialist
Management of glaucoma by a glaucoma specialist
Prognosis
 Guarded, depending on amount of optic nerve damage prior to diagnosis, efficacy of treatment, and associated ocular and systemic disorders. Haab’s striae of the cornea do not prevent good vision.
Guarded, depending on amount of optic nerve damage prior to diagnosis, efficacy of treatment, and associated ocular and systemic disorders. Haab’s striae of the cornea do not prevent good vision.
Figure 3-4. Haab’s striae. A. These breaks in Descemet’s membrane occurred secondary to congenital glaucoma. Note the multiple parallel swirling lines, which are rolled-up edges of Descemet’s membrane. B. Multiple parallel swirling lines are evident in this eye with congenital glaucoma.
CONGENITAL ANTERIOR STAPHYLOMA/KERATECTASIA
Congenital anterior staphyloma and keratectasia are extremely rare, congenital, usually unilateral conditions resulting in severe corneal protrusion and occasionally perforation (Fig. 3-5).
Etiology
 It is probably due to intrauterine keratitis.
It is probably due to intrauterine keratitis.
Signs
 Severe corneal opacification and protrusion of corneal tissue beyond the plane of the eyelids.
Severe corneal opacification and protrusion of corneal tissue beyond the plane of the eyelids.
 Endothelium, Descemet’s, and posterior corneal tissue are absent.
Endothelium, Descemet’s, and posterior corneal tissue are absent.
 It may be lined by uveal tissue posteriorly.
It may be lined by uveal tissue posteriorly.
Treatment
 A penetrating keratoplasty or anterior segment transplant can be attempted in bilateral cases, but the success rate is extremely poor. Most eyes will undergo an enucleation.
A penetrating keratoplasty or anterior segment transplant can be attempted in bilateral cases, but the success rate is extremely poor. Most eyes will undergo an enucleation.
Prognosis
 Poor
Poor
Figure 3-5. Keratectasia. Gross specimen after enucleation of an eye with a large corneal staphyloma after suspected intrauterine infection. Note the massive protrusion anterior to the corneal limbus. (Courtesy of Peter Laibson, MD.)

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


