Chapter 45 Drainage Procedures for Petrous Apex Lesions
 Videos corresponding to this chapter are available online at www.expertconsult.com.
Videos corresponding to this chapter are available online at www.expertconsult.com.
Pain may be present with benign or cystic lesions, but is more common in neoplastic lesions. Its distribution depends on the region involved. The mastoid cavity is innervated by CN IX and may radiate pain into the neck. The middle fossa and superior petrosal regions are innervated by CN V and may cause retro-orbital or facial pain. Lesions extending into the posterior fossa may cause pain along the routes of distribution of CN IX and X and the first three cervical nerves.1 Although 80% of adult mastoid bones are aerated, only 30% of petrous bones have air cells extending to the apex, and 7% may have asymmetric pneumatization of the petrous apex.2,3 The increasing use of MRI of the head and neck makes it imperative that the clinician can differentiate pathology from normal variant in the temporal bone. Table 45-1 summarizes common lesions of the petrous apex and their associated radiologic findings.
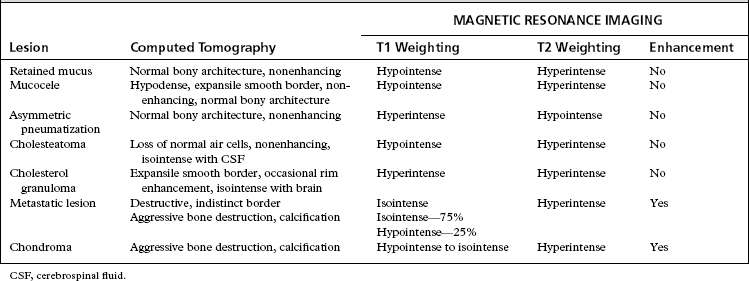
Radiologic descriptions of other, less common lesions are also summarized in Table 45-1. Differentiating between chordoma, chondroma, and chondrosarcoma of the temporal bone remains difficult, even with the scanning techniques currently available. The area of origin and the age of the patient must be considered when the pathology of destructive lesions of the petrous apex is determined.4–6
PATIENT SELECTION
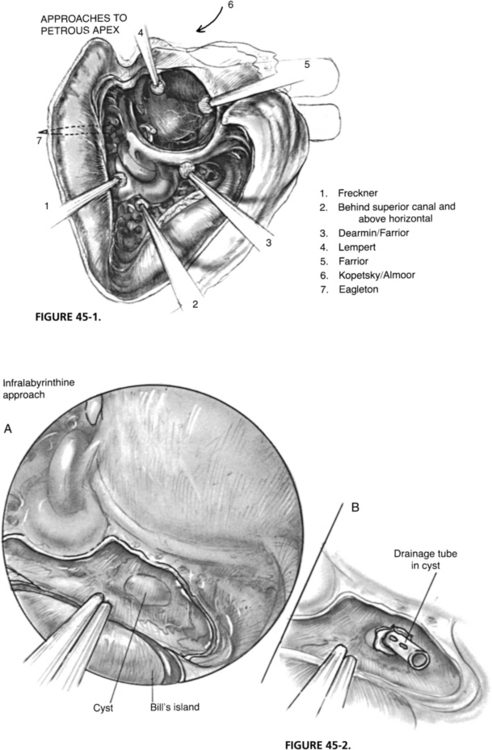
Air cell tracts extend above, below, and anterior to the otic capsule, allowing the potential of safe passage to the petrous apex. Approaches that follow superior air cell tracts include middle fossa,7 through the superior semicircular canal,8 the attic, and the root of the zygomatic arch.9 Approaches below the inner ear include the infralabyrinthine and the infracochlear.10–13 Anterior approaches have been described by Ramadier,14 Eagleton,15 and Lempert,16 who used the triangle between the anterior border of the cochlea, the carotid artery, and the middle fossa dura. All these approaches are used for drainage of inflammatory disease processes that are not responsive to antibiotic therapy or simpler operations for chronic ear disease (Fig. 45-1).
Cholesterol granuloma is the most common cystic lesion of the petrous apex, occurring 30 times less frequently than acoustic neuroma.17 It may develop in any aerated portion of the temporal bone, but most commonly occurs in the mastoid air cells distant to a lesion that prevents normal aeration. Cholesterol granuloma of the petrous apex probably develops when a pathologic process or trauma obstructs the air cell tracts to a well-pneumatized petrous apex.
PREOPERATIVE EVALUATION AND PATIENT COUNSELING
Preoperatively, patients are counseled to expect resolution of pain, if present, and the possibility of improvement in cranial nerve function if it is decreased preoperatively. Cranial nerves that have been affected for shorter periods seem to have a better prognosis and fewer long-standing deficits than nerves that have been affected longer. Patients are reminded that this is a drainage procedure with the goal of decompressing the lesion and providing an aerated cavity, if possible. The goal is not the removal of the lesion, and close follow-up may be necessary. Recurrence of the lesion secondary to inadequate drainage is usually heralded by the return of preoperative symptoms. Follow-up MRI frequently reveals a cholesterol granuloma cyst that remains full of fluid, but the T1-weighted image is hypointense compared with the preoperative hyperintense image on T1-weighted views. A return of hyperintensity on the T1-weighted image suggests inadequate drainage in a symptomatic lesion.18
SURGICAL TECHNIQUES
Infralabyrinthine Drainage of the Petrous Apex
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


