CHAPTER 116 Differential Diagnosis of Neck Masses
History and Physical Examination
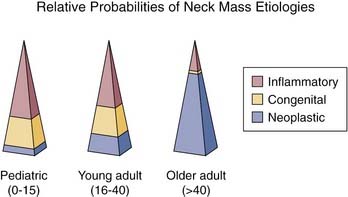
Age is a crucial element of the history-taking when evaluating a patient with a neck mass. For the purposes of the workup, patients can be broken up into several age groups: pediatric (0 to 15 years old), young adult (16 to 40 years old), and older adult (older than the age of 40) (Fig. 116-1). The difference in relative probabilities of congenital versus inflammatory versus neoplastic neck masses within these groups makes their differentiation important. In the pediatric population inflammatory masses are more common than those of congenital origin, and congenital masses are more common than neoplastic neck masses. The same can be said for the young adult population, although, as the patient ages, the risk for a neck mass of congenital origin decreases as the risk for a neoplastic process increases. The major distinction can be made in the older adult population, where consideration for neoplasia should be highest on the differential diagnosis list.1 With the exception of masses that occur in the thyroid, 80% of adult neck masses are neoplastic and 80% of those are malignant. In a child, however, more than 90% of neck masses are benign.2,3 Other important elements of the history include the time course to presentation, risk factors for immunodeficiency, and prior trauma, travel, irradiation, or surgery. Associated symptoms are also important and can help differentiate neck mass etiology and origin. Of these, fever, dysphagia, weight loss, otalgia, hearing loss, and respiratory difficulty are just a few.
Diagnostic Imaging of the Neck
The preferred imaging modality in the workup of a neck mass may differ on the basis of patient age, time course to presentation, and the clinical suspicion of the examiner (Table 116-1). In a child with suspected infectious adenopathy, ultrasound can be used to differentiate a fluid-filled abscess from a solid lymph node and help in the eventual treatment protocol.3 Ultrasound imaging is helpful in the diagnosis of pediatric neck masses because it does not require the use of sedation or general anesthesia as do the more detailed imaging modalities such as computed tomography or magnetic resonance; it is inexpensive and allows the patient to avoid ionizing radiation. Ultrasound is useful for soft tissue imaging, the differentiation of cystic versus solid masses, thyroid pathology, and salivary gland pathology,4 but it is extremely limited in providing detail regarding soft tissue invasion and approximation to bone.
Table 116-1 Imaging of Neck Masses
| Modality | Basic Indications |
|---|---|
| Ultrasound | Good for pediatric neck masses, thyroid masses. Differentiates cystic versus solid. |
| Computed tomography | Workhorse imaging modality for adult neck masses. Provides three-dimensional relationships, excellent detail of mucosal disease and involvement of adjacent bone. |
| Magnetic resonance imaging | Superior soft tissue delineation. Good for lesions of the salivary glands and tongue (where dental amalgam may obscure the view on a CT). Modality of choice for determining nerve enhancement. Consider for thyroid imaging in cases necessitating radioiodine. |
| Radionuclide scanning | Useful for midline lesions in children—differentiates functioning from nonfunctioning tissue. |
| Positron emission tomography | Useful for staging of head and neck malignancies. Can be used in cases of unknown primary malignant neck masses or treated neck disease. |
| Angiography/magnetic resonance angiography/computed tomography angiography | Useful for lesions encasing the carotid and vascular lesions. Conventional angiography should be considered for preoperative assessment in cases of potential carotid artery sacrifice or where embolization is required. |
| Plain radiograph | Generally should not be considered in the workup of a neck mass. |
Computed tomography (CT) is the workhorse imaging modality for adult neck masses. CT provides excellent resolution of both soft tissue and bone and, when used in conjunction with iodinated intravenous contrast, allows for superior delineation of vascular lesions. Neck masses can be evaluated for invasion of surrounding soft tissue and bone, airway compression, and perineural and perivascular invasion. CT also allows for determination of jugular vein occlusion in the case of infectious neck masses. CT locates masses within or outside of glands or nodal chains and provides three-dimensional relationships.4 In the workup of an adult with a suspected unknown primary metastatic neck node, CT gives excellent detail regarding head and neck mucosal sites.
Magnetic resonance imaging (MRI) is the most superior imaging modality for soft tissue detail, although it is less readily available and more expensive than the choices described previously. MRI is useful in pregnant women because it does not require radiation, and it is also a good choice for cases of well-differentiated thyroid malignancies where radioiodine therapy is to be used because iodinated contrast is not necessary.4 MRI is the best choice of imaging when perineural spread is to be determined. CT and MRI are often complementary imaging tools for the workup of an adult with a suspected head and neck malignancy.5
Radionuclide scanning can be of help in the workup of an anterior or midline neck mass, particularly in the pediatric population. Radionuclide scanning gives the added benefit of differentiating functioning from nonfunctioning tissue and thus can be considered in the workup of a lingual thyroid or thyroglossal duct cyst, where the presence of normal functioning thyroid tissue must be determined before any consideration for surgical excision. Radionuclide imaging can also be considered in the workup of salivary gland pathology because lesions can be localized to within or outside of the major salivary glands.3
Positron emission tomography (PET) is a useful imaging adjunct in the workup of head and neck malignancies, but it should not be considered standard for first-line evaluation. PET can differentiate persistent disease from postradiation effects, particularly when it is used in conjunction with contrast-enhanced CT to evaluate treated nodal disease,6 and can occasionally detect metastatic nodal disease equivocal on CT or MRI. PET is also helpful in the diagnosis of distant metastatic disease for patients with known head and neck malignancies.
Initial Workup of the Unknown Neck Mass
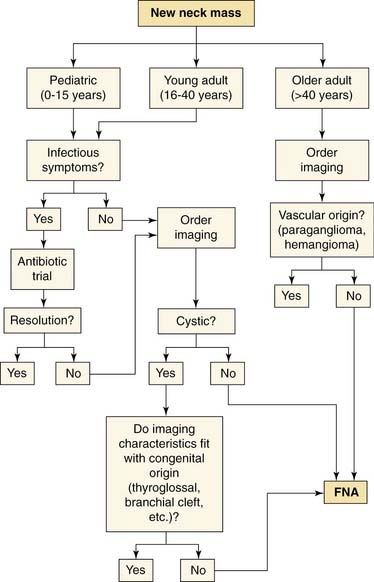
If a patient has failed an antibiotic trial, or in any case of an adult with a new neck mass, biopsy should always be considered as an essential step in making a diagnosis. The gold-standard biopsy modality in the workup of a neck mass is fine-needle aspiration (FNA) (Fig. 116-2). The sensitivity and specificity of FNA for both pediatric and adult head and neck masses have been reported to be approximately 97% when diagnostic material is obtained.7–9 FNA should always be done before the consideration of any open procedures. FNA can be used for both cytology and culture (in cases in which a suspected infectious neck mass does not respond to conventional antibiotic therapy). If an FNA is unsuccessful or if sufficient information is not obtained from an initial FNA, the FNA should be repeated before open biopsy. Multiple aspirations using a thin needle (usually 25-gauge) are necessary. The FNA should be performed in the presence of an experienced cytopathologist to ensure ideal slide preparation and thus useful diagnostic information.8,9 Studies comparing the sufficiency, accuracy, and diagnostic outcome of FNAs performed by cytopathologists versus those performed by clinicians have actually shown that cytopathologists’ FNA attempts yield significantly more useful diagnostic information than those of clinicians.8 Cells obtained by FNA can be analyzed for microbiologic, molecular, and cytogenetic properties if these techniques are useful in the diagnosis.5,8,9 If an FNA has been unsuccessful or has failed to reveal useful results after several attempts, a core needle biopsy should be considered.3,5,9 FNA may miss the true lesion in cases where a neck mass is especially bloody, necrotic, or fibrotic, and specific diagnostic information may be unattainable in lesions where complex tissue architecture is necessary.7 Open biopsy of neck masses should only be considered as a last resort for diagnosis. In the case that squamous cell carcinoma is identified in the neck during open biopsy, the surgeon should be prepared to proceed with a comprehensive neck dissection. This possibility should be part of the patient’s preoperative counseling.
Once the diagnosis is made, it will be necessary to determine whether the particular diagnosis warrants further investigations. The best example of this is the case of an unknown primary malignancy of the neck. A detailed diagnostic protocol must be adhered to in the workup of an unknown primary malignancy in the neck. A variety of pathologic entities can manifest with the primary presentation being an enlarged metastatic cervical lymph node. Among these, adenocarcinoma, thyroid malignancies, poorly differentiated carcinoma, and melanoma are seen on occasion, but squamous cell carcinoma is the most common.3,5 The detailed workup required in the evaluation of the unknown primary squamous cell carcinoma of the neck is discussed later in this chapter.
Unknown Neck Mass: Differential Diagnosis
Inflammatory Neck Masses
Inflammatory neck masses represent the most common and ubiquitous neck masses across all age groups.
Lymphadenopathy/Lymphadenitis
Inflammatory lymphadenopathy can occur in response to any infectious or inflammatory process in the head and neck and is typically a self-limited process lasting days to weeks. Lymph nodes will enlarge and become tender in the face of infection or inflammation, then typically subside without treatment. Occasionally lymph nodes will become necrotic in the face of bacterial or viral infection, and an abscess forms. These nodes can be differentiated by ultrasound or CT. Staphylococcus and Streptococcus are the organisms most commonly cultured from neck abscesses.3,4,10 Diffuse lymphadenopathy is common in patients with human immunodeficiency virus, but a growing or dominant mass should raise suspicion for lymphoma.11



