Fig. 2.1
Leukocoria due to cataract induced by a chronic retinal detachment
Table 2.1
Differential diagnosis of childhood leukocoria
1. Tumors |
Retinoblastoma |
Medulloepithelioma |
Leukemia |
Combined retinal hamartoma |
Astrocytic hamartoma (Bourneville’s tuberous sclerosis) |
2. Congenital malformations |
Persistent fetal vasculature (PFV) |
Posterior coloboma |
Retinal fold |
Myelinated nerve fibers |
Morning glory syndrome |
Retinal dysplasia |
Norrie’s disease |
Incontinentia pigmenti |
Cataract |
3. Vascular diseases |
Retinopathy of prematurity (ROP) |
Coats’ disease |
Familial exudative vitreoretinopathy (FEVR) |
4. Inflammatory diseases |
Ocular toxocariasis |
Congenital toxoplasmosis |
Congenital cytomegalovirus retinitis |
Herpes simplex retinitis |
Other types of fetal iridochoroiditis |
Endophthalmitis |
5. Trauma |
Intraocular foreign body |
Vitreous hemorrhage |
Retinal detachment |
Table 2.2
Differential diagnosis of retinoblastoma: demographics and ultrasonographic features
Condition | Age of presentation | Risk factors | Laterality | Axial length | USG |
|---|---|---|---|---|---|
Retinoblastoma | 90 % <3 years old | Family history | Unilateral or bilateral | Normal | Intraretinal/subretinal mass with calcification |
Coats’ disease | 4–10 years of age | Male gender | Unilateral | Normal | Exudative RD |
Subretinal hyper-reflective particles | |||||
PFV | Days to weeks after birth | Unilateral | Short | Vitreous band from lens to optic nerve | |
Toxocariasis | Variable | Contact with dogs | Unilateral | Normal | Peripheral mass, vitreoretinal band, traction RD |
ROP | Days to months after birth | Prematurity, oxygen supplementation | Bilateral | Short | RD with retinal bands |
It is important to carefully and urgently evaluate any child with leukocoria for the possibility of retinoblastoma, although fortunately many children referred for this complaint will have a normal examination (i.e., pseudo-leukocoria). Commonly, it is the parents who first notice the abnormal or asymmetric pupil reflex in a photograph. The flash from a camera typically causes the eye to appear red, since the pupil does not have time to contract and the camera captures a red reflection from the normal retina. Any condition that blocks the camera’s flash from reaching the retina may produce a unilateral whitish pupil reflex (i.e., photoleukocoria) [2]. However, it should be kept in mind that photoleukocoria does not always indicate an underlying pathologic condition. There are case series of patients with documented unilateral leukocoria on photographs who had normal ocular examinations [6]. This phenomenon has been termed pseudo-leukocoria since the examination did not reveal any pathology. In these cases, the child appears to be fixating 15° off axis (inward deviation), which likely resulted in an abnormal light reflex off the optic nerve in that eye (Fig. 2.2). Therefore, photoleukocoria is expected to be unilateral (i.e., one eye in a given photo). Alternating photoleukocoria may occur. Simultaneous bilateral photoleukocoria indicates either true leukocoria or esotropia. However, it is critical that any child with possible leukocoria noted by the parents or any health care professional have an urgent eye examination by an experienced pediatric ophthalmologist or ocular oncologist [7].

Fig. 2.2
Pseudo-leukocoria noticed on a photograph. Notice unilateral occurrence in the eye that appears to be fixating 15° off axis (inward deviation)
2.2 Retinoblastoma
2.2.1 Clinical Presentation
The most important clinical finding associated with retinoblastoma is the presence of a retinal-based intraocular mass, which is typically absent with the other conditions on the differential diagnosis. Dilated fundus examination in the office will reveal a whitish tumor often with prominent vascularity (Fig. 2.3). Endophytic tumors grow into vitreous and are typically whitish with associated seeding and sometimes without much vascularity. The identification of vitreous or subretinal seeding is therefore very suggestive of retinoblastoma (Fig. 2.4). Exophytic tumors grow in the subretinal space causing exudative retinal detachment (Fig. 2.5).

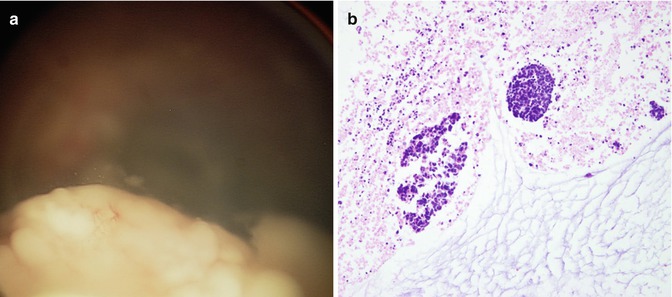
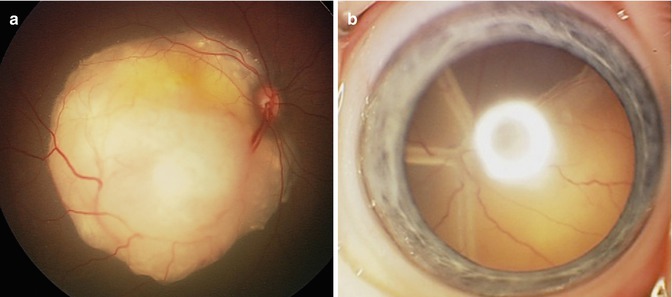
Fig. 2.3
Typical appearance of retinoblastoma. Note a whitish tumor with prominent retinal vascularity
Fig. 2.4
Endophytic retinoblastoma. Prominent vitreous seeding without intrinsic vessels (a). Histopathology of vitreous seeding (b)
Fig. 2.5
Exophytic retinoblastoma grows in the subretinal space (a). When large, they can cause exudative retinal detachment (b)
Subretinal lipid exudation can be rarely observed with exophytic tumors and should not be considered pathognomonic for Coats’ disease [8]. Diffuse infiltrative growth pattern is rare and typically presents in older children but can be difficult to distinguish from endophthalmitis or uveitis (Fig. 2.6) [9]. Vitreous hemorrhage can be seen occasionally with very advanced tumors. As a general rule, retinal traction or cataracts are not seen with untreated retinoblastoma. Anterior segment involvement by retinoblastoma can cause pseudohypopyon or hyphema (Fig. 2.7). In advanced cases, rubeosis iridis, neovascular glaucoma, buphthalmos, and even orbital cellulitis and proptosis may be encountered (Fig. 2.8) (Chap. 17) [7].
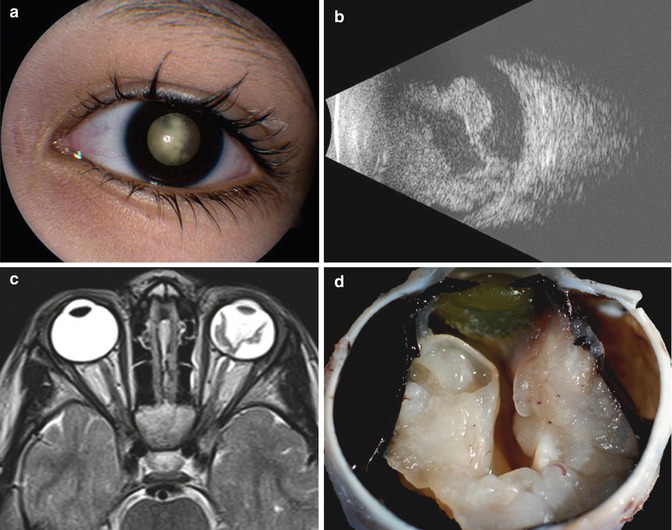

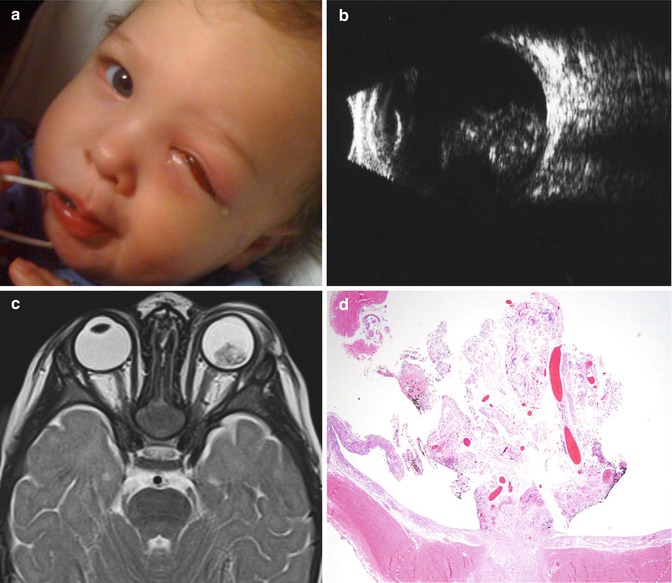
Fig. 2.6
Diffuse variant of retinoblastoma. External photograph demonstrating the appearance of diffuse retinoblastoma (a), B-scan ultrasonography revealed irregularly thickened retinal detachment with vitreous cells (b). Typical features of retinoblastoma including intraocular mass and intraocular calcification were not present. Magnetic resonance imaging confirmed enhancing thickened retina (c). Enucleated globe with diffuse infiltrating retinoblastoma (d) (Reproduced with permission from Turell et al. [11], Chapter 11)
Fig. 2.7
Anterior segment involvement by retinoblastoma presenting as pseudohypopyon (Courtesy of Paul Rychwalski MD, Cleveland Clinic, Abu Dhabi, UAE)
Fig. 2.8
Retinoblastoma presenting as orbital cellulitis. External appearance (a). B-scan ultrasonography reveals a large intraocular mass extending from the optic disk. Multiple hyperechogenic intensities are present throughout the mass consistent with calcium deposition (b). T2-weighted axial magnetic resonance image reveals an intraocular mass emanating from the optic nerve and retina of the left eye (c). Retrobulbar stranding as well as preseptal edema are evident as well. Histopathologic section (hematoxylin–eosin, original magnification ×40) of the enucleated globe consists of fibrin, detached and degenerating retina, inflammatory cells, prominent vascularity, a small amount of necrosis, and calcification (d) (Reproduced with permission from Sachdeva et al. [12])
2.2.2 Demographics/History
Approximately 90 % of diagnosed cases of retinoblastoma cases are sporadic, while 10 % have a positive family history. The average age of diagnosis is 18 months, but retinoblastoma may be present at birth or as old as 8 years. The majority of cases diagnosed below age 1 tend to have bilateral disease while children older than 2 years typically have unilateral disease. Overall, retinoblastoma is unilateral in 70 % and bilateral in 30 % of cases. The incidence is equal in males and females and there is no significant racial or ethnic predilection. There is a genetic association with 13q deletion syndrome, which also presents with other systemic anomalies including mental retardation.
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


