Diagnostic Techniques for Ocular Viral Infections
Jay C. Bradley
Rachael H. Bradley
Francisco J. Garcia-Ferrer
Vahid Feiz
Ivan R. Schwab
Viruses are obligate intracellular microorganisms that lack ribosomes and often other systems required for replication. Thus, viruses rely on the cellular host to produce viral gene products. As a result, viral agents are more difficult to identify morphologically and are more difficult to isolate in culture than are other classes of organisms such as bacteria and fungi.
The basic unit of a virus is the virion, which is composed of ribonucleic acid (RNA) or deoxyribonucleic acid (DNA) surrounded by a symmetrical protein coat, the capsid. Some viruses possess a lipoprotein outer membrane or envelope that may be coded by viral genes or may be acquired from the host on exit from the host cell. Many viruses depend on mechanisms such as pinocytosis to allow penetration into a cell. Because individual viruses generally infect only certain types of host cells, susceptible cells are believed to have specific receptors for viral attachment. Knowledge of these and other viral properties is helpful in virus identification.
History and Physical Examination
Clinical history and physical examination are the best diagnostic tools for viral infections. For example, a patient with the appropriate epidemiologic exposure, a follicular conjunctivitis, a mild keratitis, a preauricular lymph node, and scattered subepithelial opacities should easily be diagnosed as having adenoviral conjunctivitis. Most cases of herpetic ocular disease can be made by history and clinical examination, making laboratory tests unnecessary. Misdiagnosis can occur in atypical presentations, especially in the immunocompromised, or when patients present to nonspecialists, and diagnostic testing can be helpful in these cases. Laboratory confirmation allows appropriate treatment with antiviral medications and can also be useful in unresponsive cases. In this chapter the laboratory tools and techniques to assist the clinician in diagnosis are emphasized, but the importance of the history and physical examination and a skilled observer cannot be overemphasized.
Traditionally, laboratory techniques such as microscopic cytology, culture, and immunocytochemistry supplemented clinical data. Recently, nucleic acid hybridization techniques and DNA amplification methods have revolutionized the field of molecular biology and are increasingly important in ophthalmic research. Several of these techniques, particularly the polymerase chain reaction (PCR) have become vital clinical tools in the diagnosis of infectious ocular diseases. These advances necessitate at least a rudimentary understanding by clinicians of the science behind these evolving methods to appropriately utilize each technique.
Ocular Diagnostic Techniques
Viral Culture
Viral species differ in the cell lines in which they can grow, although some viruses can grow in a variety of tissues or cells. Herpes simplex virus (HSV), for example, can be isolated after intracerebral inoculation of suckling mice, from the chorioallantoic membrane of embryonated hen eggs, from mink lung, or from several susceptible cell lines. Conversely, some viruses (e.g., adenovirus) are difficult to isolate and may require specific human cell lines for isolation. Cell culture generally includes essential ingredients for cell growth, serum, antibiotics, and antifungals. Depending on the virus in question and its particular cell culture requirements, a specific cytopathic effect on the cell line is achieved (Tables 88.1 and 88.2).
TABLE 88.1 Diagnostic Tests for Specific Viruses | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
TABLE 88.2 Commonly Used Ocular Diagnostic Techniques | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Traditional cultures allow accurate diagnosis but can take 21 days or more before evidence of viral cytopathic effect. A modification of this procedure, the shell vial culture, has significantly decreased the time required to just days. In this assay, the patient’s sample and tissue culture media are added to a vial containing a circular coverslip covered with fibroblasts on the bottom. This shell vial is centrifuged and incubated for 1 to 2 days. The coverslip and fibroblast culture is then removed and a labeled monoclonal antibody is applied. These antibodies will bind viral antigens present in infected fibroblasts and are subsequently visualized using fluorescence microscopy. This technique is available for most viruses associated with ocular disease including HSV, varicella zoster virus (VZV), cytomegalovirus (CMV), adenovirus, and enterovirus.1
A modified culture technique recently reported for ocular specimens called enzyme-linked virus-inducible system (ELVIS) can provide results in 24 hours. ELVIS HSV was developed using a transgenic baby hamster kidney-21 cell line. In this cell line, HSV infection causes the expression of a beta-galactosidase “reporter gene,” and it is the expression of this gene that can be used to monitor infection by HSV. Cultures positive by ELVIS are confirmed by immunofluorescent staining (discussed later).2
Cell culture is the gold standard for confirmation of suspected viral infection. Many authorities believe cultures underestimate the true prevalence of active HSV infection,3,4,5 as viral cultures are quite specific but may lack sensitivity.6 Unfortunately, viral cultures are relatively expensive and laborious. Culture also requires 1 to 5 days, which can delay initiation of appropriate therapy. Specimen storage and transport in viral transport media can also limit its sensitivity. Consequently, this tool is not available at every hospital and is almost never found in a private office.
Cytology
Exfoliative Cytology
Conjunctival exfoliative cytology, a well-established technique familiar to all ophthalmologists, is an important if underappreciated diagnostic tool. Gram stain, almost universally available in a hospital setting, is perhaps the prototype for diagnostic exfoliative cytology; however, this technique is designed principally for bacteria and fungi rather than viruses.
Giemsa stain emphasizes cellular morphology and can be useful in diagnosing viral infections. Tzanck smear is another simple, inexpensive preparation used to show viral-induced cellular abnormalities.7 HSV infections often show multinucleated giant cells with either Giemsa stain or Tzanck smear.7 These epithelial cellular aggregates with 3 to 20 nuclei have relatively little cytoplasm and a pale halo between nuclei and cytoplasm. Although somewhat difficult to find on a smear, multinucleated giant cells are diagnostic of infection by either HSV or VZV. Less specifically, lymphocytes predominate in smears from superficial viral infections.
Intranuclear viral inclusions may be found with Giemsa stain, with Tzanck smear (with eosin),7 or perhaps better with Papanicolaou stain. HSV and CMV infections produce intranuclear eosinophilic inclusions (Lipschutz inclusions), but these are difficult to find with any of the three stains. Molluscum contagiosum produces eosinophilic cytoplasmic inclusions (Henderson-Patterson inclusions), especially from expressed lesions, although inclusions are best seen with hematoxylin and eosin staining. Although these exfoliative cytologic techniques are perhaps less sensitive and specific than newer immunologic tools, they are inexpensive and quick, and are an essential base for many of the newer methods.
The application of these cytologic techniques is not limited to exfoliative cytology. Cell samples from intraocular fluids or ocular biopsy may be evaluated by any of the previously mentioned cytologic techniques. Exfoliative cytologic samples are usually applied directly to a slide or can be obtained by impression cytology.8 However, intraocular fluids are best handled by centrifugation9 or cytocentrifugation10 before microscopic evaluation. Membrane filter techniques,11,12 which require that the fluid be passed through a filter (e.g., Millipore) to trap solid material, are perhaps superior to both centrifugation and cytocentrifugation.12 This technique is especially valuable with scanty specimens. Cell block techniques can be used on the pellet formed with centrifugation as well as for small fragmented biopsy material.
Electron Microscopy
Electron microscopy with negative staining is relatively quick (2 to 5 hours), but it requires an electron microscope, trained personnel, and a sample with an adequate number of viral particles. It is also less sensitive than viral culture techniques. Occasionally the technique may be useful, as illustrated by one report of herpetic uveitis diagnosed by examination of cells in the aqueous humor.13
Immunologic Exfoliative Cytology
Immunocytochemistry techniques have been used to diagnose infectious cornea and external ocular disease for decades. Indirect and direct immunofluorescent techniques, immunoperoxidase techniques, and most recently immunoenzyme techniques are available. Simple, commercially available kits utilize this technology for rapid (within 24 hours) diagnosis of a potential pathogen, often a virus. Immunologic techniques utilize the relationship between an antibody and a particular antigen on a target organism. A series of antisera are used to bind the antigen to the antibody, and then the antisera are tagged with a detection agent such as fluorescein or biotin.
Indirect immunofluorescent technique.
The indirect immunofluorescent technique is performed by placing cells from the infected area on a clean glass slide. A primary antiserum obtained from an animal (e.g., rabbit) vaccinated against the suspected antigen is then applied. A fluorescein-conjugated, second antiserum from a different species (e.g., goat) is directed against the immunoglobulin type of the primary antiserum (e.g., goat antirabbit immunoglobulin; Fig. 88.1). Controls include suspected antigen-bearing cells stained with a negative primary antiserum (or not stained at all), followed by all reagents. Such controls provide a measure of nonspecific fluorescence.14
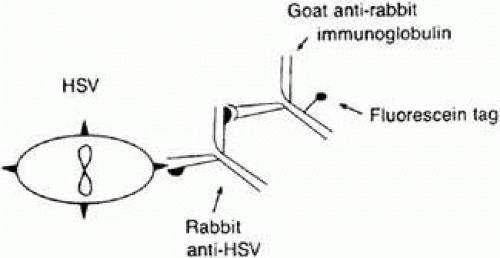 FIGURE 88.1 The indirect immunofluorescent technique uses a fluorescein-labeled secondary antibody. |
Direct immunofluorescent technique.
The direct immunofluorescent technique is a variation on the indirect technique.3 Primary antibody is produced by vaccinating an animal (e.g., rabbit) with antigen (e.g., HSV). The primary antibody is then conjugated to fluorescein isothiocyanate. The antiserum containing this conjugated antibody is applied to a slide containing the cells suspected to have the antigen, and the immunofluorescence is evaluated under an immunofluorescence microscope (Fig. 88.2).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


