Chapter 18 Developmental anomalies of the lids
NORMAL DEVELOPMENT AND ANATOMY OF THE EYELIDS
CLINICAL EVALUATION OF THE EYELIDS
DEVELOPMENTAL ANOMALIES OF THE PERIORBITAL REGION
ABNORMAL ASPECT OF THE INNER CANTHUS
MAJOR MALFORMATIONS OF THE EYELIDS
ABNORMAL POSITION OF THE EYELIDS
SPARSE OR ABSENT EYEBROWS AND/OR EYELASHES
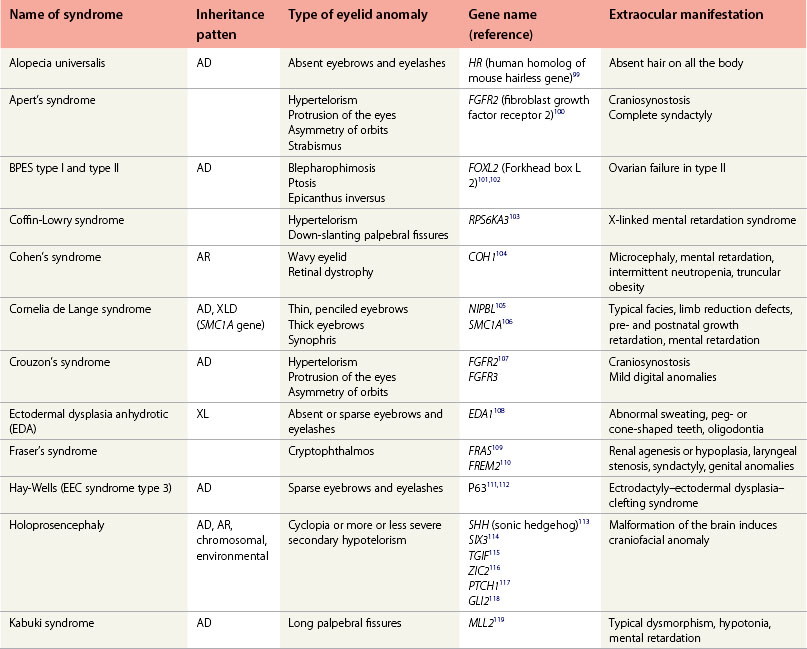
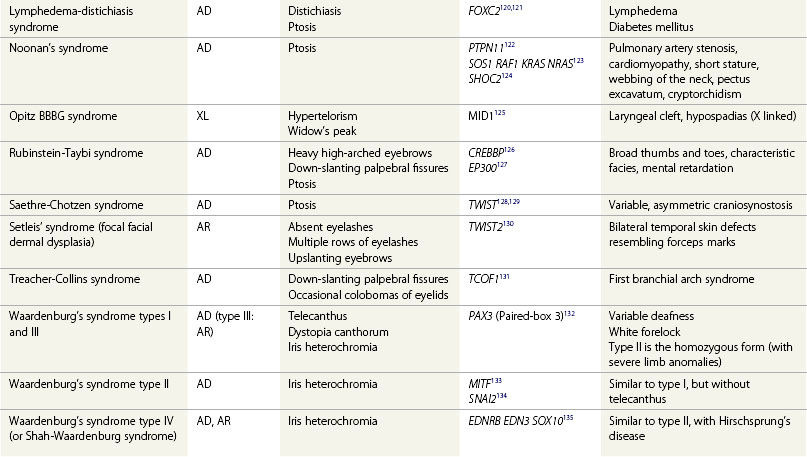
DYSMORPHOLOGY DATABASES AND GENES INVOLVED IN SYNDROMES WITH EYELID ANOMALIES
Major developmental anomalies create significant medical problems.1 They often require specific surgical or medical management. Minor anomalies are features that vary from those commonly seen in the normal population; they do not cause increased morbidity. Major anomalies are not a variation of the normal spectrum. Developmental anomalies of the eyelids can belong to both categories. They can be isolated or observed in a syndromic context.
Single developmental anomalies are divided into four categories:2
1. A deformation is caused by an abnormal external force (usually, but not always) before birth, that results in an abnormal growth or formation of a body part.
2. A disruption occurs when a normally growing region is disrupted by some process, such as anoxic necrosis. Usually, disruptions and deformations are isolated and not associated with multiple congenital anomalies.
3. A malformation is an abnormal development of a body part due to an underlying genetic, epigenetic, or environmental or stochastic factor that alters normal development.
4. A dysplasia is an alteration of an intrinsic cellular architecture that can appear, or evolve with time (by opposition to a malformation). Malformation and dysplasia are not mutually exclusive: a malformation can be underlined by a tissue dysplasia.
When several developmental anomalies are present, three situations are defined:
1. An association is a group of anomalies that occur more frequently together than expected by chance, but which do not have a unified underlying etiology. Many associations described in the literature are syndromes (such as the CHARGE “association”).
2. A sequence is a group of anomalies that stem from a single major anomaly that alters the development of other surrounding or related tissues or structures. The term “field defect” describes malformations of distinct anatomic structures located in a particular region of the body.
3. A syndrome is a well-characterized constellation of major and minor anomalies that occur together in a predictable fashion, presumably due to a unique underlying etiology that may be monogenic, chromosomal, mitochondrial, or teratogenic in origin. A syndrome is clinically defined, and several distinct etiologies may be causative (e.g. Bardet-Biedl syndrome can be caused by more than 16 different gene defects).
Normal development and anatomy of the eyelids
Embryology of the eyelids
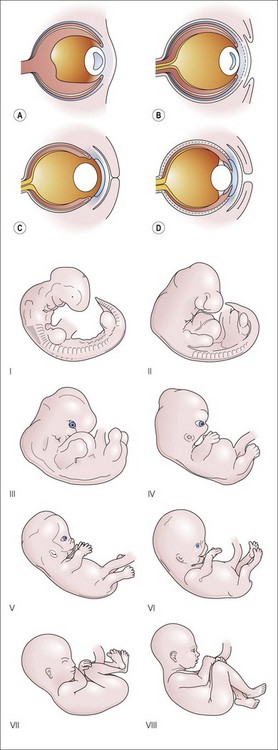
Development of the eyelids is characterized by three main stages:
Final reopening
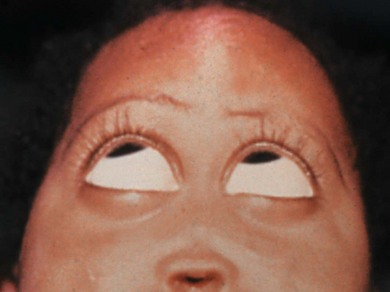
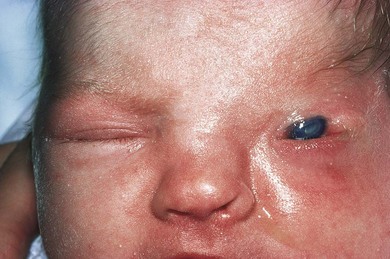
Separation begins from the nasal side, and is usually completed during the sixth or seventh month of development. Very rarely, this process is incomplete at birth in a full-term infant (Fig. 18.1).3 The specialized structures in the lids develop between 8 weeks and 7 months. By term, the lid is fully developed.
Morphology and anatomy of the eyelids
The eyelids have several characteristic horizontal and vertical folds.
The palpebral fissure is the entrance into the conjunctival sac bounded by the margins of the eyelids; it forms an asymmetrical ellipse that undergoes complex changes during infancy.4 After birth, the upper lid has its lowest position with the lower eyelid margin close to the pupil center. Between ages 3 and 6 months, the position of the upper lid reaches its maximum. The distance between the pupil center and the lower eyelid margin increases linearly until age 18 months.4 By adulthood, the upper eyelid covers the upper 1–2 mm of the cornea, the lower lid lies slightly below its inferior margin.5 Palpebral fissures have a slight outer-upward inclination as the outer canthus is positioned 1 or 2 mm higher than the inner canthus. The normal orientation of the eyelids varies depending on ethnic origin. Palpebral fissure length increases during normal development.6
Clinical evaluation of the eyelids
Dysmorphology is the study of abnormal development. Guidelines were proposed by an international group for most dysmorphologic terms.7–10
Morphologic measurements can be easily performed with a transparent ruler. The measurements are compared to a normal database.5
Clinical landmarks
The embryonic separation of the globes (the angle between the optic nerves at the chiasm of the fetus) progresses from a 180° angle between the ocular axes in the first weeks of development to 70° at birth, 68° in adulthood 11,12 (Fig. 18.2A). The interorbital distance (the shortest distance between the inner walls of the orbits) increases with age13 (Fig. 18.2B). The most accurate interorbital measurements are obtained from X-rays (Waters half-axial projection, or posteroanterior cephalograms) or computed tomograms.14
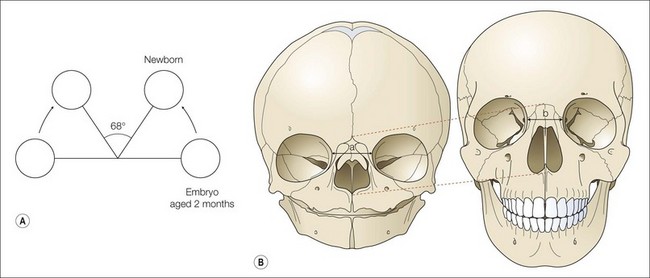
Fig. 18.2 Evolution of the ocular axis and the inner interorbital wall during development of a human face. (A) Ocular axis from 180° for an 8-week-old embryo to 68° for a newborn (adapted from Zimmermann et al.8). (B) Evolution of the bony orbit: a face from a newborn compared to an adult.
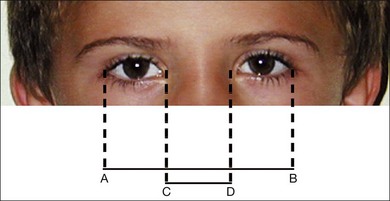
Clinical evaluation of the interocular distances is based on the measurement of the following lid-based landmarks:15–19
An approximate “rule of thumb” is that the inner intercanthal distance should be equivalent to the palpebral length (Fig. 18.3).
There are tables presenting the change in interocular distances according to age. The clinical method for assessing interocular distance is based on a biometric study that includes measurements of the inner intercanthal distance, the outer intercanthal distance, and the interpupillary distance in Caucasians from birth to 14 years. The normal intercanthal distance is 20 ± 2 mm (1 SD) at birth, increasing to 26 ± 1.5 mm by 2 years of age. The normal interpupillary distance is 39 ± 3 mm at birth, increasing to 48 ± 2 mm by 2 years of age.4
Ethnic variations of orbital features are important; comparison of newborns from England and Africa showed that the Caucasian and the African newborns had the same inner canthal distance, whereas the outer canthal distance and palpebral fissure length were significantly smaller in Caucasian newborns than in African newborns.20
Normal growth curves for many physical parameters have been compiled by Hall et al.21
Developmental anomalies of the periorbital region
Abnormal distances between the eyelids and orbits
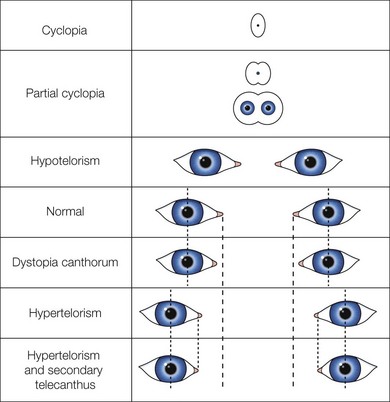
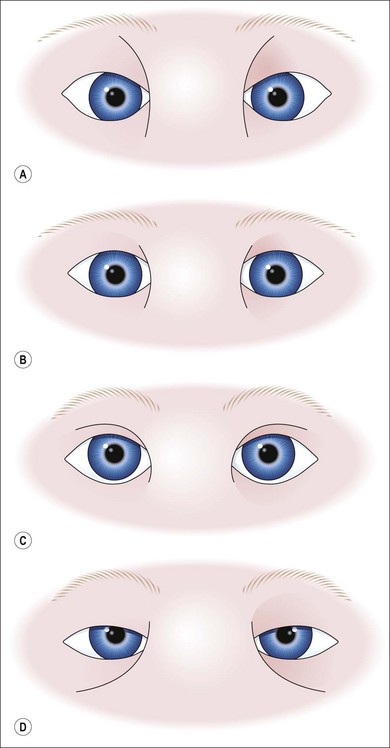
Conditions with abnormal distances between the eyelid landmarks are defined in Table 18.1 and schematically presented in Fig. 18.4.
Table 18.1 Conditions with abnormal spacing of the orbits and eyelids
| Condition | Definition | Comments |
|---|---|---|
| Hypertelorism | Increased distance of the inner and outer intercanthal distances | |
| Hypotelorism | Reduced distance between the medial walls of the orbits with reduced inner and outer intercanthal distances | |
| Telecanthus | Increased distance between the inner canthi | Often mistaken as hypertelorism |
| Primary telecanthus: increased distance between the inner canthi (normally spaced outer canthi and normal interpupillary measurement) | ||
| Secondary telecanthus: increased inner canthi distance (associated with ocular hypertelorism) | ||
| Dystopia canthorum | Similar to secondary telecanthus (telecanthus) together with lateral displacement of the lacrimal puncta | Clinical tip: an imaginary vertical line passing through the lacrimal punctum cuts the cornea |
Hypertelorism
Hypertelorism corresponds to an interpupillary distance of more than 2 SD above the mean. It results from excessive distance between the medial wall or bony orbits. Hypertelorism occurs in more than 550 disorders (Figs 18.5 and 18.6) and is often subjectively appreciated and confused with telecanthus. Three pathogenic mechanisms have been suggested:13
1. The early ossification of the lesser wings of the sphenoid, fixing the orbits in fetal position
2. The failure of development of the nasal capsule, allowing the primitive brain vesicle to protrude into the space normally occupied by the capsule, resulting in morphokinetic arrest in the position of the eyes as in frontal encephalocele (see Chapter 56)22
3. A disturbance in the development of the skull base as in craniosynostosis syndromes (i.e. Crouzon’s or Apert’s syndromes) or in midfacial malformations such as frontonasal dysplasia.

Fig. 18.5 Hypertelorism in Optiz’ syndrome (esophageal abnormalities, hypospadias, and other midline defects).
(Image courtesy of Clinique Ophthalmologique des Hôpitaux Universitaires de Strasbourg.)

Telecanthus and dystopia canthorum
Telecanthus is defined as a distance between the inner canthi more than 2 SD above the mean for age, sex, and ethnicity. It is common and often associated with hypertelorism. Dystopia canthorum is a specific feature of Waardenburg’s syndrome (WS) type 123 (Fig. 18.7), where telecanthus results from abnormal outward displacement of the inner canthi relative to the ocular globe. This condition is an autosomal dominant syndrome with variable expressivity, characterized by:

WS type 2 differs from WS type 1 by the absence of dystopia canthorum. Type 3 is the homozygous state of type 1 with limb anomalies; type 4, a genetically heterogeneous, autosomal dominant or autosomal recessive disorder, is associated with Hirschsprung’s disease.25
Hypotelorism
Hypotelorism is an interpupillary distance more than 2 SD below the mean. Hypotelorism occurs in more than 60 syndromes (Fig. 18.8). It can result from premature closure of the metopic sutures resulting in vertical frontal ridge, up-slanted palpebral fissures and hypotelorism.26
Hypotelorism can also result from insufficient development of the brain hemispheres, as in holoprosencephaly. Holoprosencephaly is a rare brain anomaly, frequently associated with facial anomalies (see Chapter 56).27,28 It results from an early abnormal formation of the telencephalic vesicles: they remain partially or totally fused. Holoprosencephaly usually leads to underdevelopment of middle facial structures. Severity of midfacial anomalies usually correlates with the severity of the underlying brain malformation,29,30 forming a spectrum that goes from:
• A single median orbit with fused eye globes (cyclopia with or without synophthalmia), to
• Nasal and premaxillary agenesis, to
• A single central maxillary incisor with hypotelorism (see Table 18.1).
Holoprosencephaly may be due to environmental/maternal factors (such as maternal diabetes), chromosomal abnormalities (trisomy 13, 18q deletion), or single gene defects31 (Table 18.2).
Abnormal aspect of the inner canthus
Epicanthus palpebralis
Epicanthus palpebralis (or epicanthal fold) is a vertical cutaneous fold arising from the nasal root and directed toward the internal part of the upper lids (Fig. 18.9). It can be subdivided into the areas where they occur such as preseptal, pretarsal, or orbital. The fold may cover the inner canthus. It is normal in fetuses of all ethnic origins and common in young children with a flat nasal bridge. Epicanthus palpebralis is a normal feature in many populations, mostly Asians. It is common in syndromes where the nasal bridge is flat, such as trisomy 21. Epicanthus often vanishes with age.


Major malformations of the eyelids
Ablepharon
Ablepharon is the absence of lids. It occurs in several settings:
1. Neu-Laxova syndrome – with intrauterine growth retardation, syndactyly, swollen “collodion” skin, microcephaly, and severe developmental brain defects.32
2. Autosomal dominant ablepharon-macrostomia syndrome – absent or rudimentary eyelids,33 a hypoplastic nose, ambiguous genitalia, absent zygoma, and macrostomia with possible familial recurrence34 (Fig. 18.10).
3. Say-Barber syndrome35 – hypertrichosis of the back, macrostomia, microblepharon, ectropion, and sometimes ablepharon. It could be allelic to ablepharon-macrostomia syndrome.

Cryptophthalmos (see Chapter 17)
Cryptophthalmos is rare: there is failure of development of the eyelid folds with continuity of the skin from the forehead to the cheek.36,37 In complete cryptophthalmos, the epithelium that is normally differentiated into cornea and conjunctiva becomes part of the skin that passes continuously from the forehead to the cheek. The eyebrow is usually absent and the globes are microphthalmic. In the incomplete form, a rudimentary lid and conjunctival sac is present. Abortive cryptophthalmos presents with a normal lower lid and an absent or abnormal upper lid, the forehead skin passing directly to and fusing with the superior cornea (Fig. 18.11).
Cryptophthalmos may be an isolated finding or present as part of Fraser’s syndrome.36 Fraser’s syndrome is a rare autosomal recessive syndrome with cryptophthalmos, hypoplasia of the genitalia, laryngeal stenosis, and renal hypoplasia or agenesis.
Ankyloblepharon
Ankyloblepharon is partial or complete adhesion of the ciliary margins of the superior and inferior eyelids. Ankyloblepharon filiforme ad natum is usually a sporadic isolated malformation in which the upper and lower lids are joined by tags (easily cured by a simple surgical procedure)38 (Fig. 18.12). Ankyloblepharon may be inherited as an autosomal dominant trait. It may occur in association with ectodermal defects and cleft lip and/or palate in Hay-Wells syndrome,39 an allelic variant of the ectodactyly– ectodermal dysplasia–cleft lip palate (EEC) syndrome (see Chapter 28). Ankyloblepharon may occur in trisomy 18.40

Clefting or notching of the eyelids (“coloboma”)
Notches or clefts of the eyelid have been described as eyelid colobomas, but there is no embryologic relation with defects due to malclosure of the embryologic fissure. They are usually triangular with the base at the lid margin. The size varies from a discrete notch to a major defect with exposure keratopathy requiring surgery.41
Eyelid colobomas may occur in all areas of the eyelids but are most common in the nasal half of the upper lid. More than one lid may be involved; there may be multiple colobomas in the same lid. The eye may be normal or have abnormalities such as corneal opacities, and iris and retinal colobomas extending to microphthalmos and anophthalmos. There may be associated bands limiting ocular motility; strabismus is common.42 The cause of eyelid colobomas remains uncertain. They may be equivalent to facial clefts, but intrauterine factors may play a major role.43 Amniotic bands may cause mechanical disruptive clefting of the eyelids in the amniotic deformity, adhesions, mutilations (ADAM) syndrome.44
Coloboma of the upper lid can occur in the oculo-auriculo-vertebral dysplasia syndrome (Goldenhar’s syndrome), which has no clear genetic basis (Fig. 18.13
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


