We have designed and developed several different integrated OCT/US probes for intravascular imaging [29–31]. Figure 72.2 shows an integrated probe with a focused ring ultrasound transducer [31]. The homemade 50 MHz focused ring transducer has an effective aperture of 2-mm with a 0.8-mm hole at the center to make room for the OCT probe. The coaxial US and light beams have a common focal length of 4 mm, and both are steered into tissue by a 45° mirror along their pathway. Co-registered rabbit aorta images from the integrated intravascular OCT/US system is shown in Fig. 72.3 [31]. Figure 72.4 shows another design of an integrated OCT/US probe that has an outer diameter of less than 0.7 mm [29]. In vitro OCT and US images of human coronary artery with pathology, as well as in vivo images of vascular tissue in rabbit and porcine animal models, were obtained using this integrated OCT/US probe. Figure 72.5 shows an intravascular OCT/US image from a human coronary artery specimen with a calcified plaque [29]. The plaque can be identified in both OCT and US images. From the OCT image, the plaque cap, as highlighted by the arrow, can be clearly identified due to the high axial resolution and high contrast of OCT. However, the OCT system could not visualize the entire depth features of the vessel wall. On the other hand, in the US image, the acoustic shadow as pointed by the arrow indicates the location of the plaque and US provides much deeper penetration depth than OCT. However, from the US image, one can hardly distinguish the border between calcium and the surrounding tissue due to inferior resolution of US. We have obtained, to the best of our knowledge, the first in vivo images of vascular tissue in rabbit and porcine animal models using this integrated OCT/US probe [29]. Although further research and development is required to translate this technology to clinical practice, these results clearly demonstrated the potential of the integrated IVUS/OCT system.
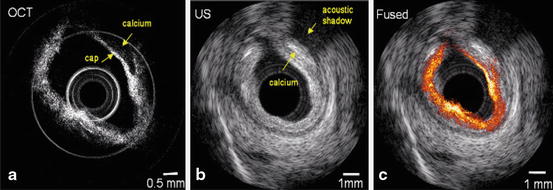

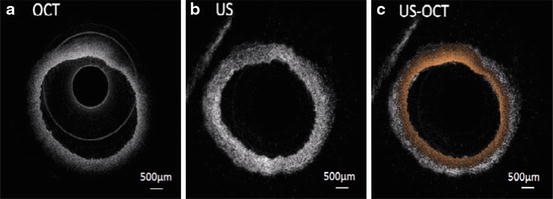

Fig. 72.5
OCT/US images of human coronary artery specimen from an integrated OCT/US system. (a) OCT image, (b) ultrasound image, (c) overlaid OCT/US image [29]
72.3 Integrated Intravascular OCT and Fluorescence Imaging
Diagnosis of the latent vulnerability of a plaque lesion relies on both structural and tissue chemical compositions. Although OCT has been used for vulnerable plaque evaluation due to its high resolution, it lacks molecular specificity for identification of tissue composition in plaques. Intravascular fluorescence molecular imaging provides biomolecular information of atherosclerosis inside the blood vessel [21, 54]. It is known that macrophage infiltration affects plaque stability [55]. A fluorescent tagged antibody, such as Annexin V, that targets apoptotic macrophages can provide critical information to determine vulnerability of plaques [56]. In addition, fluorescent lifetime measurement has also been used for the detection of macrophage/foam cell infiltration and discrimination of lipid-rich lesions in atherosclerotic artery [6]. Therefore, an integrated OCT/fluorescence imaging system combining the high spatial resolution of OCT with the molecular sensitivity of fluorescence imaging is capable of resolving both microstructure and biomolecular information at the same time [21, 40].
Integration of intravascular OCT and fluorescence imaging has been reported by a number of groups [21, 40]. The schematic of an integrated swept source OCT-fluorescence system based on a micro motor is shown in Fig. 72.6 [40]. For the OCT system, a swept laser with a center wavelength of 1310 nm, FWHM bandwidth of 100 nm, and output power of 8 mW is used as the light source. The laser beam is split in an 80/20 ratio by a 1 × 2 coupler, with 80 % of the power directed to the WDM input port then to the combined OCT and fluorescence probe, and 20 % to the reference arm. Two circulators are used in the reference and sample arms, respectively, to redirect backscattered and back-reflected light to the two input ports of a 50/50 2 × 2 coupler for balanced detection. For the fluorescence imaging system, a continuous-wave (CW) laser diode with a center wavelength of 635 nm and output power of 5 mw is used as the excitation source for fluorescence imaging. A photomultiplier tube (PMT) is used to detect fluorescence emission light. The excitation light and the OCT beam are combined together with a wavelength division multiplexer (WDM coupler 635/1,310). A double-clad fiber (DCF) combiner with one single-mode fiber port, one multimode fiber port, and one DCF port is used to deliver the OCT and fluorescence excitation light beams to the sample and collect the OCT fluorescence signals. The OCT and fluorescence excitation light are transported through the 8 μm core of the DCF, and the back-reflected fluorescence emission light is collected through the 105 μm inner cladding of the DCF. Subsequently, the backscattered OCT signal from the sample is coupled back through the single-mode fiber port of the combiner and the WDM coupler to the OCT system. Fluorescence emission light backscattered from the sample is coupled back through the multimode fiber port of the combiner and detected by the PMT. The use of a single-mode DCF core to deliver the fluorescence excitation light improves the lateral resolution of the fluorescence image. The schematic diagram of the dual-modality intravascular probe is shown in Fig. 72.6b. A micro motor is used for circumferential scanning of the inner blood vessel wall. This distal scanning design eliminates the disadvantage of unstable vibration and uneven rotational speed in a proximal scanning design and can be applied to more flexible materials without the need of rotational torque transfer [57]. A linear motor outside the endoscope is used to pull back the entire probe to create 3-D helical OCT scanning and to achieve a 2-D superficial fluorescence intensity image. OCT and fluorescence emission signals are digitized by a two-channel, 250 M samples/s 12 bit data acquisition card and transferred to a computer for processing.
Fig. 72.6
Schematic of the OCT/fluorescence system. Black line denotes single-mode fiber (SMF28), red line denotes multimode fiber, and blue line denotes double-clad fiber (DCF). (b) Intravascular probe based on a DCF combiner. OCT and fluorescence excitation light are transported through the single-mode core of the DCF; the back-reflected fluorescence emission light is collected through the inner cladding of the DCF [40]
We have used integrated OCT/fluorescence to image the aorta of a New Zealand white rabbit. Annexin V conjugated Cy 5.5 was used as the fluorescent contrast to target the plaques and stain the tissue. Annexin V is an antibody that targets apoptotic macrophages which accumulate in the necrotic core, a key characteristic of vulnerable plaques [56]. OCT/fluorescence images from phantom plaques are shown in Fig. 72.7. Figure 72.7a shows the schematic of the two phantom plaques inside the blood vessel wall. Figure 72.7b illustrates the fused fluorescence-OCT image of the model plaques. Figure 72.7c shows the 3-D OCT image and Fig. 72.7d shows that the OCT image of the mimic plaque matches well with the 2-D fluorescence intensity image. This experiment demonstrates that our system is capable of obtaining both OCT and fluorescence intensity signals simultaneously. We can choose different agents to target various molecular factors in vulnerable plaques.
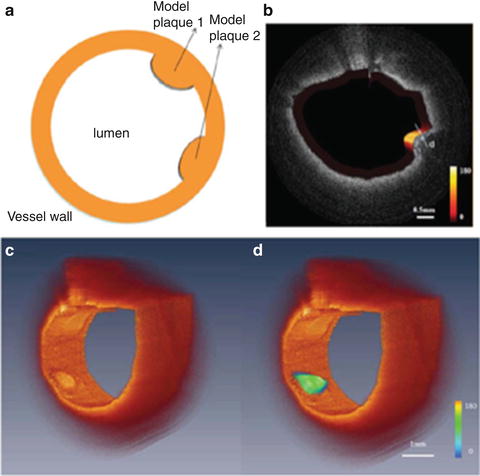
Fig. 72.7
(a) Schematic of model plaques, (b) fused OCT/fluorescence image of normal rabbit aorta with phantom plaques. The thickness of the plaque cap is around 128 μm as indicated in label (d). The color scale in (b) shows the relative intensity of the fluorescence signal. (c) 3D OCT image and (d) combined 3-D OCT/fluorescence image [40]
72.4 Phase-Resolved Acoustic Radiation Force Optical Coherence Elastography (ARF-OCE)
Tissue mechanical properties provide critical information to assess the vulnerability of plaques [41–45]. The stress in the cap increases with decreased thickness and increased macrophage infiltration. High strain locations in the vessel wall indicate the presence of vulnerable plaques [41–44]. Elastography is an imaging technique [58], which measures the local deformation of tissue induced by stress to estimate the strain and stiffness which are directly related to the biomechanical properties. Elastography has become a powerful technique to distinguish healthy and diseased tissues, particularly in cardiovascular research.
Significant progress has been made in developing intravascular ultrasound (IVUS) elastography [42, 59–62]. However, since the dimensions of the structural components of the vulnerable atherosclerotic plaques, such as fibrous caps and carotid arteries, are on the order of 50–200 μm, the resolution of the IVUS imaging system, which lies in the range of 150–300 μm [63], is not sufficient to resolve the entire structural details of plaques.
Optical coherence elastography (OCE) has a superior micrometer scale resolution and is therefore suitable for imaging subtle mechanical changes in the early stages of disease [64]. Excitation and detection are generally the two prominent characteristics of an OCE system. There are two main categories of OCE with respect to the excitation method: static/quasi-static excitation OCE and dynamic excitation OCE [65, 66]. The former applies compression to the subject statically/quasi-statically and measures the relaxation dynamics, which has limited imaging speed for in vivo imaging. The latter dynamically excites the subject using various waveforms and detects the induced displacement in a gated time window, which enables a much higher imaging speed and makes it possible for in vivo imaging. For the detection system, a phase-resolved OCT system can detect displacements with up to nanometer sensitivity [67]; this is especially important for intravascular imaging as better sensitivity in displacement measurements means reduced force needs to be applied to a vessel wall to quantify tissue mechanical properties. Phase-resolved dynamic OCE has been investigated previously for shear wave propagation detection [68, 69], but this method requires separation of excitation and detection points which limits the speed and spatial resolution. Adaptation of this method is difficult for in vivo real-time 2D and 3D vascular elastography.
We recently developed a phase-resolved ARF-OCE system that uses an acoustic wave to apply pressure to the tissue and uses phase-resolved OCT to evaluate the elastic properties of vascular tissue [46]. The ARF-OCE combines the high-speed excitation of ARF with sub-micrometer/nm detection sensitivity of phase-resolved OCT. This elastography technique allows high-speed and high-resolution point-by-point mapping of local strains in atherosclerotic coronary tissue. Since the mechanical properties of fibrous and fatty plaques are different, PR-ARF-OCE has the potential to differentiate between various plaque components.
Phase-resolved ARF-OCE utilizes chirped acoustic radiation forces to produce excitation along the sample’s axial direction and phase-resolved Doppler OCT to measure the vibration of the sample. Figure 72.8 shows imaging of a section of atherosclerotic human coronary artery with phase-resolved ARF-OCE. An OCT intensity image, shown in Fig. 72.8a, provides a general morphological view of the tissue with no obvious evidence of the presence of atherosclerosis. By applying a 500 Hz chirped acoustic radiation force onto the tissue, a strong vibration phase contrast can be clearly imaged using ARF-OCE (Fig. 72.8b). The region indicated by the white arrow in ARF-OCE image is characterized by less vibration and therefore represents less elastic, stiffer tissue such as plaques. The strong vibration representing softer tissue is indicated by yellow arrows. In this ARF-OCE image the stiffer tissue, in this case atherosclerotic plaque, is clearly distinguished from the softer (usually normal) tissue area highlighted by brighter colors. The transition between the plaque and normal region appears blue (indicated by blue arrows) and is characterized by intermediate elasticity. This result clearly shows that our ARF-OCE method has great potential to quantitatively characterize mechanical properties of vascular plaques, which may provide critical information towards determining plaque vulnerability.
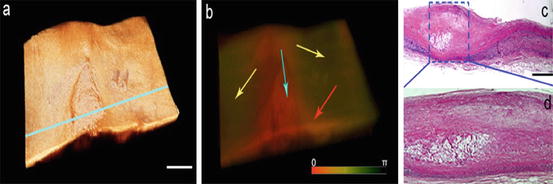
Fig. 72.8
(a) OCT structural, (b) ARF-OCE phase images of a human cadaver coronary artery under 500-Hz, 350-mV AM modulated excitation; an atherosclerotic lesion was identified as the red region corresponding to the blue box in (c). (c) Histological image and (d) close-up view of the atherosclerotic lesion. Scale bars: 1 mm [46]
72.5 Summary
Recent landmark intravascular imaging studies have highlighted the morphological characteristics of high-risk plaques and have generated substantial interest in this area [2, 21, 70–76]. These studies have led to substantial developments in basic science and clinical understanding of plaque stability and progression [77]. They have emphasized the areas requiring further investigation and the urgent need for more intravascular studies [78]. It is particularly important to address functional and compositional aspects of high-risk plaques. Our current knowledge of inflammatory pathways and mechanisms is solely provided by either postmortem specimens of coronary vasculature or circulatory biomarkers. However, the first are not representative of the sequence of events during plaque development, while the later are not representative of the local microenvironment [79]. In vivo imaging, therefore, is of utmost importance despite the fact that it is not currently used for day-to-day clinical practice [80]. It will enable the further understanding of plaque disruption mechanisms and development of strategies for the prevention of acute coronary events, including sudden death.
The clinical need and value for an imaging system that can identify patients with vulnerable plaques at high risk of rupture has been discussed extensively in the literature [7, 81–83] and also highlighted in this year’s NIH/NHLBI Working Group Report on Detection of High-risk Atherosclerotic Plaque [80]. Currently there is no imaging system that can reliably determine plaque risk or predict late occlusion after drug-eluting stent placement [7, 82, 84]. Several interventional procedures to treat vulnerable plaques at high risk of rupturing are under clinical trials [85–87]. The widespread clinical application of these measures requires the improved risk stratification of vulnerable plaques with better predictive power [80, 88]. The ability to detect these vulnerable plaques noninvasively is likely to serve as a powerful stimulus for an increased effort in the development of such therapies [85–87]. This chapter describes integration of intravascular OCT with ultrasound, fluorescence, and elastography. A number of other label-free optical techniques, such as second harmonic generation (SHG) imaging of collagen, two-photon excited fluorescence (TPEF) imaging of elastin, CARS imaging of lipids, and photoacoustic imaging of absorption contrast, have not yet reached the stage of clinical studies but have shown great potential for atherosclerotic research [8–16]. An integrated intravascular imaging modality that can measure structure, chemical composition, and tissue mechanical properties and detect and characterize vulnerable plaques will provide a critically important tool for monitoring the progression of disease and evaluating the efficacy of intervention. The surveillance and early diagnosis of vulnerable lesions will prove to be of the utmost importance in further efforts to tailor therapeutic interventions in patients at risk [89].
Acknowledgments
I would like to thank many of our colleagues who have contributed to the intravascular imaging project at UCI Beckman Laser Institute, Department of Medicine Cardiology Division, and Department of Biomedical Engineering, particularly the students and postdoctoral fellows. In addition, I would like to thank my collaborators, Drs. Qifa Zhou and K. Kirk Shung, as well as their students at USC NIH Ultrasonic Transducer Resource Center and Department of Biomedical Engineering, for joint development of miniature ultrasound transducers for the intravascular imaging project. Finally, I also want to acknowledge grants support from the National Institutes of Health (R01EB-10090, R01EY-021529, R01HL-105215, R01HL-125084, and P41EB-015890), Air Force Office of Scientific Research (FA9550-04-0101), and the Beckman Laser Institute Endowment.
References
2.
C. Weber, H. Noels, Atherosclerosis: current pathogenesis and therapeutic options. Nat. Med. 17(11), 1410–1422 (2011)CrossRef
3.
R. Virmani, F.D. Kolodgie, A.P. Burke, A.V. Finn, H.K. Gold, T.N. Tulenko, S.P. Wrenn, J. Narula, Atherosclerotic plaque progression and vulnerability to rupture: angiogenesis as a source of intraplaque hemorrhage. Arterioscler. Thromb. Vasc. Biol. 25(10), 2054–2061 (2005)CrossRef
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


