 he patient in this case presented with a huge orbital cyst that appeared at the upper lid. She also had severe hypotropia and ptosis. She was a poor man’s daughter, and they could not afford to travel to seek help from an orbital or oculoplastic surgeon. We used the Fugo blade to excise the cyst.
he patient in this case presented with a huge orbital cyst that appeared at the upper lid. She also had severe hypotropia and ptosis. She was a poor man’s daughter, and they could not afford to travel to seek help from an orbital or oculoplastic surgeon. We used the Fugo blade to excise the cyst.
TECHNIQUE
Anesthesia
Administer general anesthesia.
Surgical Technique
- Make a skin incision over the most prominent part of the cyst. In this case, when the cyst was reached, I attempted to separate it from the surrounding tissues with a 100-µm capsulotomy tip. It quickly became apparent that it would be impossible to remove the cyst in toto without making a huge incision. I decided to drain the cyst before removing the cyst wall.
- Make a 1-cm incision in the thick cyst wall. In this case, I removed a large amount of cheesy material and hair by applying pressure to the outside of the eye and scooping material from inside.
- I attempted to separate the wall of the empty cyst with the same ablation tip but stopped because the tip was very soft and flexible, it was taking far too long, and it could not be done without magnified vision.
- Excise the anterior part of the wall that has been separated from the surrounding tissues. In this case, I was able to remove the rest of the contents of the cyst through a large hole.
- Perform all further dissection, separation, and cutting with a blunt scissors aided by an artery forceps. Minor bleeding may be controlled by applying pressure. Remove the cyst completely, leaving the bed of the cyst very smooth.
- Close the incision line in two layers, the orbicularis and the skin. Use 80-µm vanadium steel sutures. In this case, recovery was uneventful (Fig. 46.1).
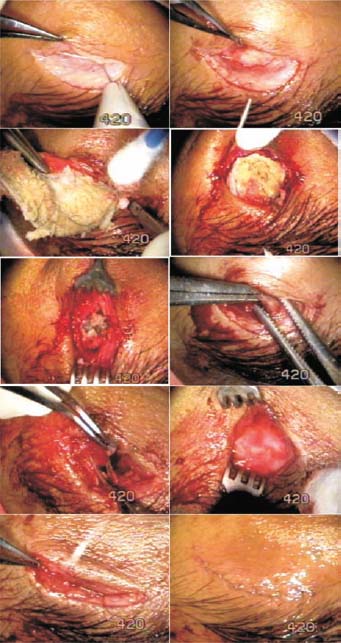
Figure 46.1. The cyst is incised over the most prominent projection and separated from the surrounding tissues with a 100-µm Fugo blade tip. A 1-cm incision is made in the cyst, and a large amount of cheesy material and hair is expressed. The visible cyst wall is excised to expose and remove more contents. The emptied cyst is held with artery forceps, and further isolation and excision of the wall is done with a scissors. The smooth bed of the cyst is visible. The incision is closed in two layers with 80-µm steel sutures.
Summary
This surgery was a unique and exhilarating experience for me because I had never ventured so far into the orbit. Subsequently, I discovered that blunt dissection could be done bloodlessly using a 600-µm Fugo blade tip. If I were to encounter a similar case tomorrow, I would alter the surgical technique slightly as follows.
- Incise the skin with 100-µm tip and reach the cyst.
- Use scissors to dissect the cyst away from the orbital contents.
- Incise the cyst wall and drain or remove the contents of the cyst.
- Close the incised cyst with 80-µm steel sutures.
- Grasp the cyst with an artery forceps and pull it out from every direction. Continue separating the cyst from the surrounding tissues with a 600-µm Fugo blade until all of the cyst is removed in one piece.
Suggested Reading
Winn CW. Broad applications seen for plasma blade. Ocular Surg News Asia Pacific Ed. 2001;19:45–46.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


