Fig. 1 Atticotomy with preservation of the bony bridge in a case of intact ossicular chain. The posterior and superior tympanomeatal flaps are elevated, and superior and posterior tympanotomies are performed, exposing the tympanic cavity. The lateral wall of the attic is removed nearly up to the tegmen tympani. The superior ligaments of the incus and malleus, the posterior ligament of the incus, and the anterior ligament of the malleus are illustrated. In the tympanic cavity, the round window niche, the stapes with the stapedial muscle tendon, and the pyramidal process are illustrated. The posterior malleolar ligament is torn (short arrow)
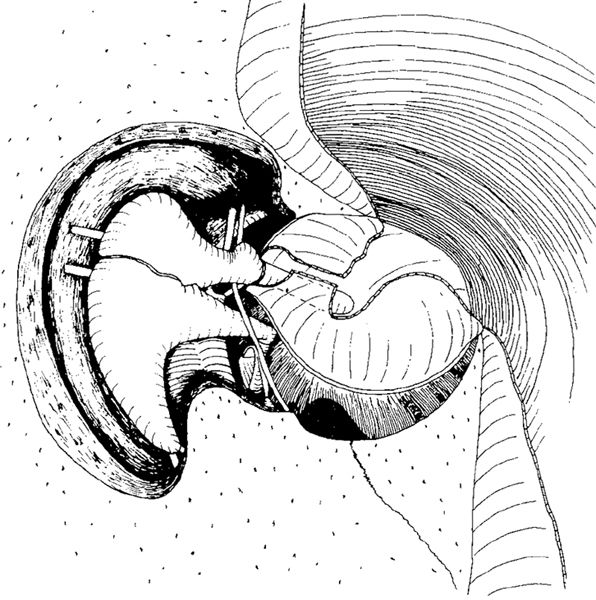
Fig. 2 Atticotomy with total removal of the bony bridge in a case with an intact ossicular chain. The posterior and superior tympanotomies are performed, and the bony bridge and lateral wall of the attic are removed, exposing the entire lateral attic. The entire course of the chorda tympani, from the chordal eminence posteriorly under the malleus handle and along the tendon of the tensor tympani muscle to the anterior wall of the attic, is illustrated
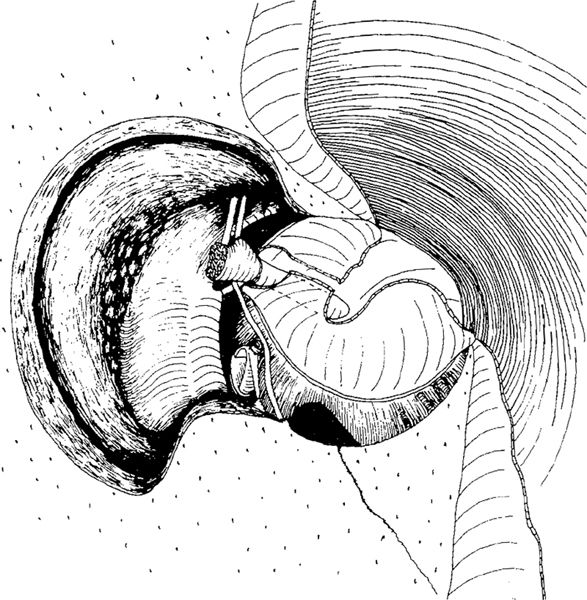
Fig. 3 Atticotomy with removal of the bony bridge in a case of resorbed malleus head and incus body, which are removed, leaving only the malleus handle. The medial attic is exposed, illustrating the eminence of the tensor tympani muscle (arrow) with the cochleariform process, the prominence of the horizontal part of the facial nerve, and the lateral semicircular canal. Small perilabyrinthine air cells are indicated

Fig. 4 Atticotomy with a partially removed bony bridge. The bridge is either drilled away or resorbed at its middle part—which is a very common situation in attic cholesteatoma
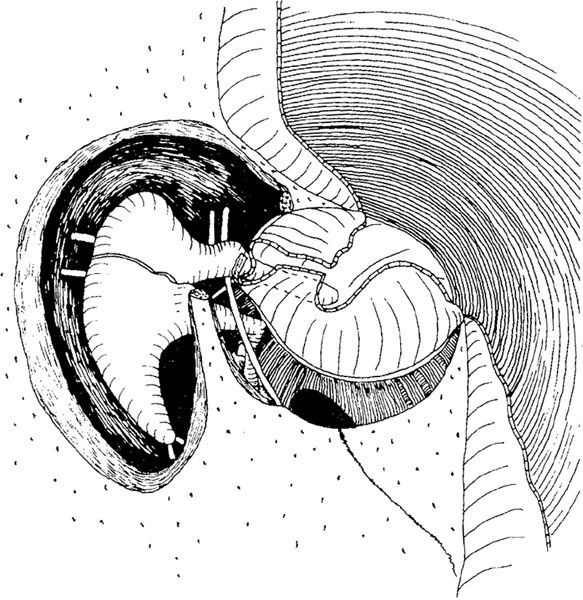
Fig. 5 Atticotomy with removal of the anterior part of the bony bridge, sometimes necessary in cholesteatoma extending into the anterior attic
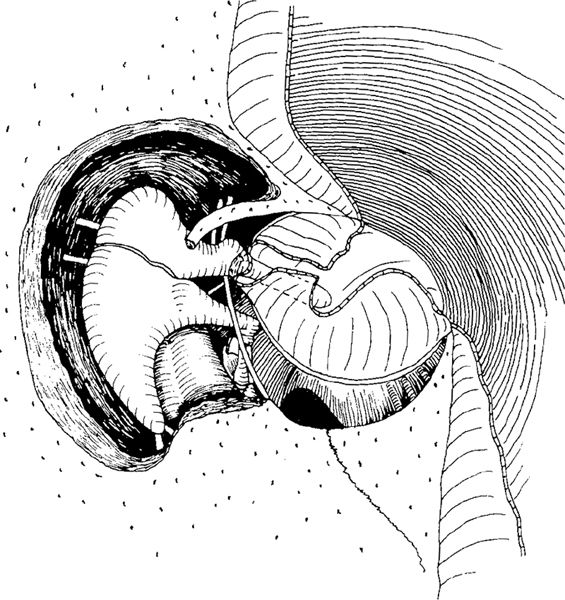
Fig. 6 Atticotomy with removal of the posterior part of the bony bridge, sometimes necessary in sinus cholesteatoma
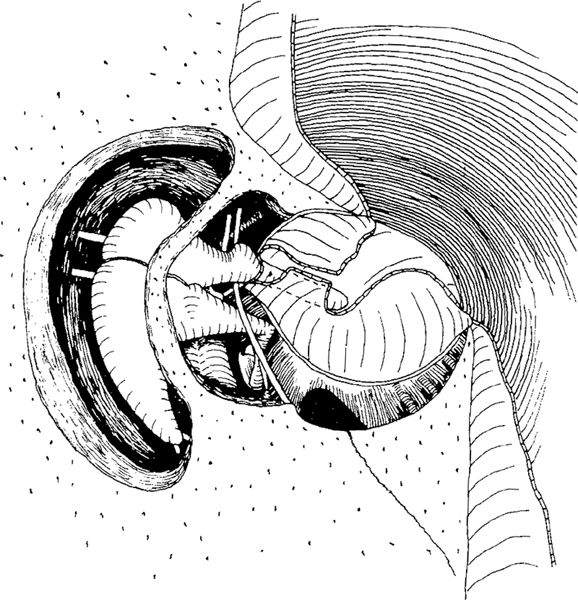
Fig. 7 Atticotomy with superolateral displacement of an intact bridge. First some of the bony bridge is drilled away in order to visualize the mesotympanum. An atticotomy with preservation of the bridge is then performed, resulting in a superolateral displacement of the bridge
The present author prefers atticotomy with preservation of the bridge, but the methods involving removal of the bridge have been quite popular, mainly because they are less time-consuming and are easy to perform. There are many possible combinations of the methods of partial removal of the bony bridge and displacement of the bridge, resulting in great variability in atticotomy.
Atticoantrotomy
Atticoantrotomy is an extension of the atticotomy in a posterior direction through the transmeatal route. The lateral attic and aditus walls are removed, and the antrum is entered. The posterosuperior bony ear canal wall is removed, and the access to the antrum is gradually widened (Figs. 8, 9).
An atticoantrotomy can be performed through the transcortical route, but is usually performed through the transmeatal route. There is a gradual transition from an atticotomy to the conservative radical mastoidectomy, and in fact there are no rules as to when an extensive atticoantrotomy should be described as a conservative radical operation or as an atticoantrotomy (Fig. 8).
In cases with poor pneumatization, a small antrum, and a sclerotic mastoid process, an atticoantrotomy results in a small cavity with smooth walls (Fig. 9). In a large cell system, the atticoantrotomy results in a large cavity.
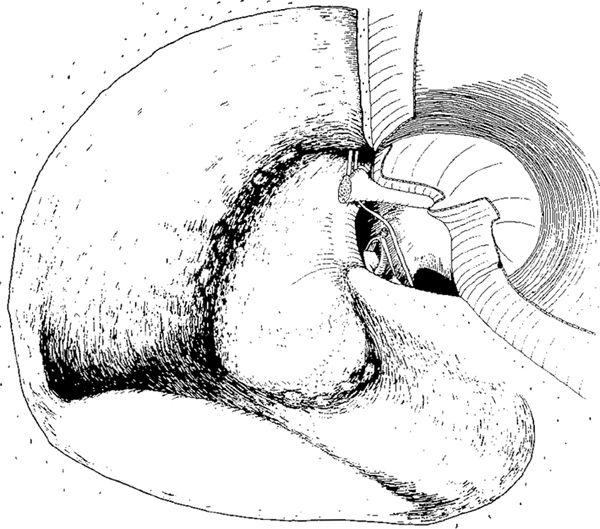
Fig. 8 The large atticoantrotomy. The posterosuperior bony wall of the external auditory canal is removed, and the tegmen tympani, tegmen antri, and tegmen mastoidei, as well as the prominence of the sigmoid sinus, are exposed, leaving thin, smooth, bony plates. The sinodural angle is cleansed, and the walls are smoothed. The sinus-facial angle is relatively deep, and the facial ridge is high. The malleus head and incus are removed, exposing the medial walls of the attic and aditus ad antrum, with the lateral semicircular canal and the eminence of the horizontal part of the facial nerve. In the anterior attic, the anterior malleolar ligament and chorda tympani are present. Some flat perilabyrinthine air cells superior to the lateral semicircular canal and inferior to the posterior semicircular canal remain
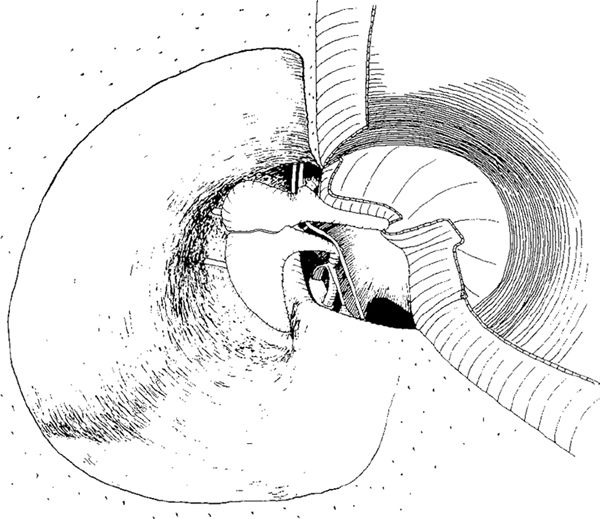
Fig. 9 A small atticoantrotomy in a case of sclerotic mastoid process, small antrum, and intact ossicular chain. The cavity is small, with smooth walls, the sinodural angle is flat, and the sinus–faciai angle is small. There is a smooth transition from the facial ridge to the eminence of the horizontal part of the facial nerve.
Bondy’s Operation
An atticoantrotomy is described as Bondy’s operation if the tympanic cavity is not entered (Bondy 1910). The lateral part of the cholesteatoma matrix is removed (Fig. 10) and the medial part is left in place (Fig. 11), marsupializing the cholesteatoma. If the tympanic cavity is entered (Fig. 12), the operation is not described as Bondy’s operation, but as an atticoantrotomy or conservative radical operation, even if the cholesteatoma matrix is left in place (Fig. 13).
If the tympanic cavity is opened and the cholesteatoma marsupialized with the matrix being left in place in the attic, fascia has to be placed under the matrix in order to prevent ingrowth of the cholesteatoma into the tympanic cavity, and also to allow safe adaptation between the keratinized squamous epithelium of the matrix and the epithelium of the replaced drum remnant and canal skin (Fig. 14).
The principal difference between Bondy’s operation and atticoantrotomy or conservative radical surgery with marsupialization of the cholesteatoma is therefore the opening of the tympanic cavity. If there is no need for hearing improvement and ossiculoplasty, the tympanic cavity is not opened in Bondy’s operation, is contrast to atticoantrotomy with marsupialization, where a tympanoplasty is also performed, either to prevent ingrowth of the cholesteatoma into the tympanic cavity or as part of an ossiculoplasty (Fig. 14).
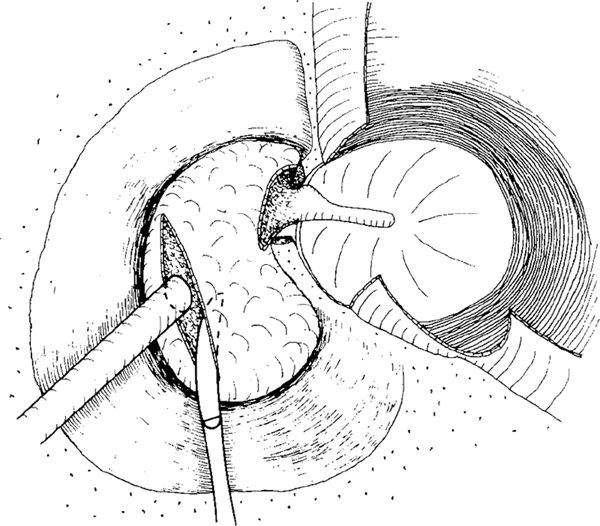
Fig. 10 Bondy’s operation. After atticoantrotomy with removal of the posterosuperior bony meatal wall, the cholesteatoma sac involving the atticus and antrum is exposed. The sac is incised, a suction tube is placed in the sac, and the cholesteatoma mass is sucked away. The lateral part of the matrix is cut off. The tympanic cavity is not entered
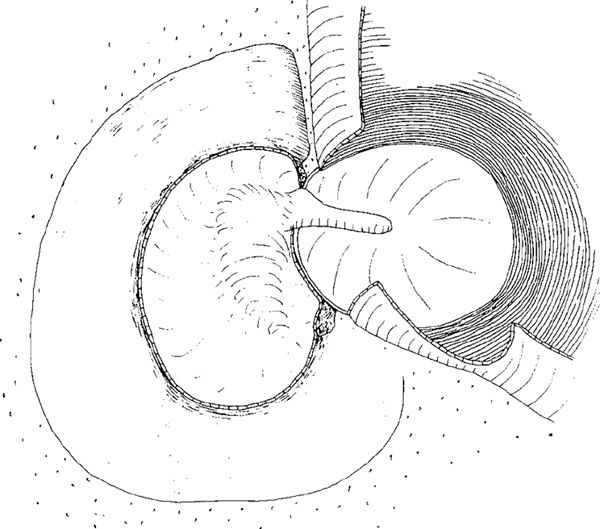
Fig. 11 The completed Bondy’s operation, with the atticoantrotomy. The medial part of the cholesteatoma matrix is left in place, and the bridge is removed, exposing all the cholesteatoma matrix. The malleus and incus are intact, but covered with the cholesteatoma matrix. Superiorly, the epithelial flap will be returned to cover the superior wall of the cavity. Inferiorly, the flap will cover the facial ridge. The smooth walls of the cavity will soon be epithelialized
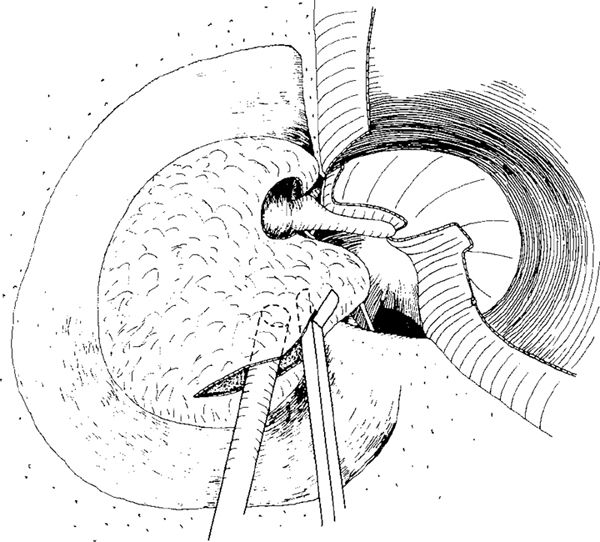
Fig. 12 Atticoantrotomy, or conservative radical operation, with marsupialization of an attic cholesteatoma extending into the tympanic cavity, which is open. The sac is incised, and the cholesteatoma is sucked out. The tympanic cavity is entered, with the tympanomeatal flap being elevated posteriorly
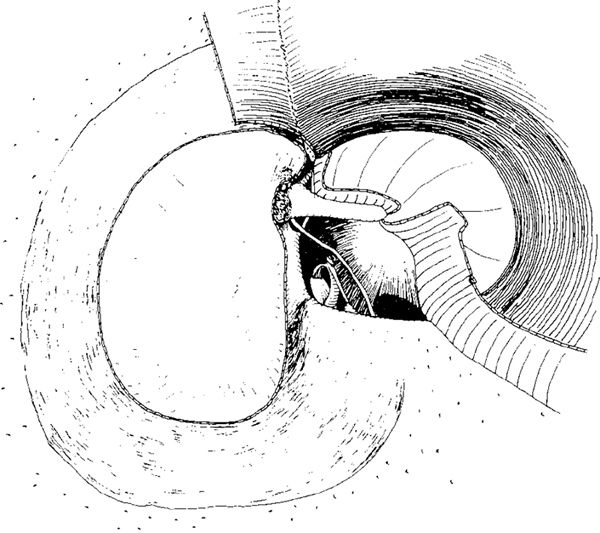
Fig. 13 After removal of the partly eroded incus, and after resection of the head of the malleus, the medial part of the cholesteatoma matrix is left in place. The cholesteatoma is marsupialized in the attic and antrum regions, but removed from the tympanic cavity
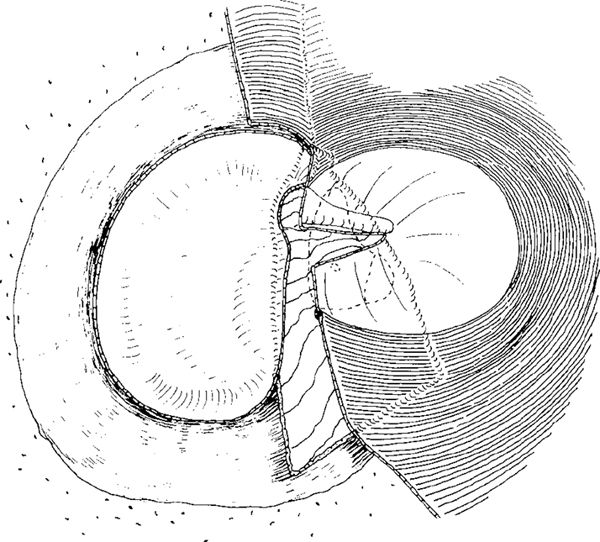
Fig. 14 After an incus interposition between the stapes and the malleus handle, after placement of the fascia under the epithelial edges and under the drum, and after replacement of the skin flaps, the conservative radical operation is completed
In the treatment of attic cholesteatoma, a gradual transition from an atticotomy with removal of the bony bridge (Fig. 3) to Bondy’s operation can be seen. Usually, it is only the extent of bone removal from the posterosuperior ear canal wall and the adherence of the cholesteatoma membrane to the lateral semicircular canal, with blockage of the ventilation through the tympanic isthmus, that distinguishes a large atticotomy from a small Bondy’s operation. In both types, the medial part of the cholesteatoma sac is left in place, covering the intact ossicular chain (Figs. 15, 16), or the medial wall of the aditus ad antrum with the lateral semicircular canal (Fig. 17) and the medial wall of the antrum (Fig. 18). These techniques are fast, safe, and simple, and can easily be performed under local anesthesia.
In cases with a small attic cholesteatoma, good hearing, and no significant discharge, and in which the bottom of the cholesteatoma or a deep retraction pocket cannot be seen, an atticotomy can be performed by removing the scutum until the bottom is visible (Figs. 15, 19). The lateral wall of the cholesteatoma sac is removed, and the medial wall is left in place, improving access to the cholesteatoma sac and facilitating migration of the keratin from the sac.
In an attic cholesteatoma involving the aditus ad antrum, a large part of the posterosuperior bony ear canal has to be drilled in order to perform a large atticotomy and marsupialize the cholesteatoma (Figs. 16, 20). Ventilation of the antrum still occurs through the tympanic isthmus under the incus body and the malleus head, and under the medial part of the cholesteatoma matrix, which is not yet adherent to the lateral semicircular canal (Fig. 16). The adherence of cholesteatoma membrane to the lateral semicircular canal is probably the most reliable sign differentiating the atticotomy from the Bondy’s operation in cases of attic cholesteatoma. In cases with adherence of the cholesteatoma membrane to the lateral semicircular canal (Fig. 17), the aditus ad antrum is involved in the cholesteatoma, and ventilation of the antrum cannot take place through the tympanic isthmus. Extensive removal of bone is necessary to visualize the cholesteatoma sac, and the result resembles a small open atticoantrotomy cavity—a Bondy’s operation (Figs. 11, 17). Similarly, in cases with involvement of the antrum (Fig. 14), a Bondy’s operation is performed, resulting in a small open cavity.
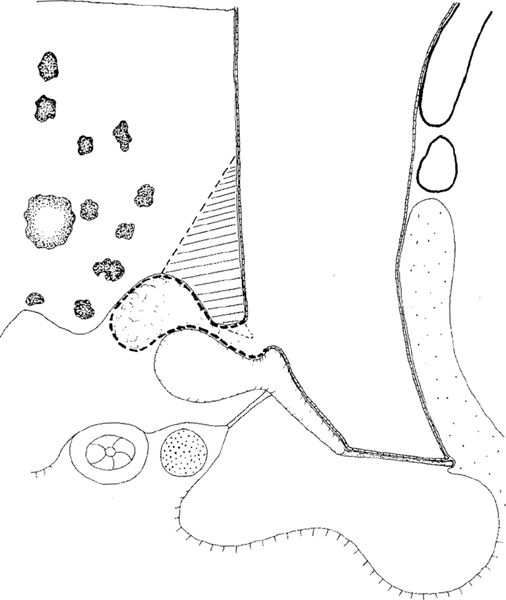
Fig. 15 Side view of an atticotomy with removal of the scutum and the bony bridge (hatched area) in a case of small attic cholesteatoma located in the lateral attic between the head of the malleus and the scutum (thick dashed line). The lateral membrane of the cholesteatoma sac is removed exposing its medial wall. The antrum is aerated from the mesotympanum through the tympanic isthmus
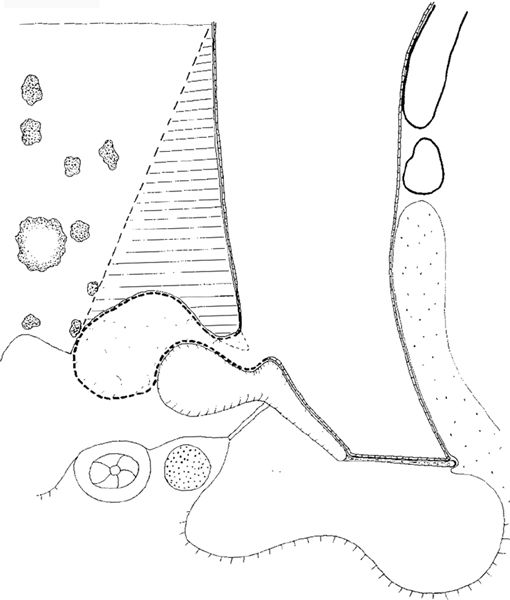
Fig. 16 Side view of an atticotomy with large removal of the superior bony ear canal wall (hatched area) and the lateral part of the cholesteatoma in order to marsupialize the attic cholesteatoma (dotted line). Ventilation of the antrum through the tympanic isthmus is still possible
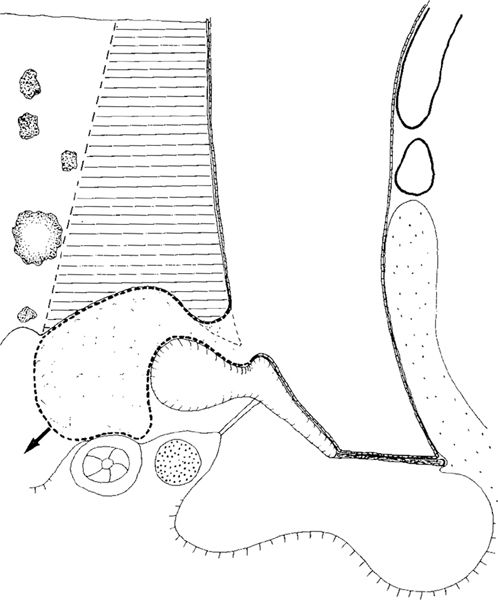
Fig. 17 Side view of a large atticotomy or a small Bondy’s operation in an attic cholesteatoma involving the aditus ad antrum, adherent to the lateral semicircular canal closing the tympanic isthmus, and blocking the ventilation of the antrum. Even after removal of the large part of the superior bony ear canal wall (hatched area) and the lateral membrane of the cholesteatoma sac (dashed line) with good exposure of the medial cholesteatoma wall, progression of the cholesteatoma is possible towards the antrum (arrow)
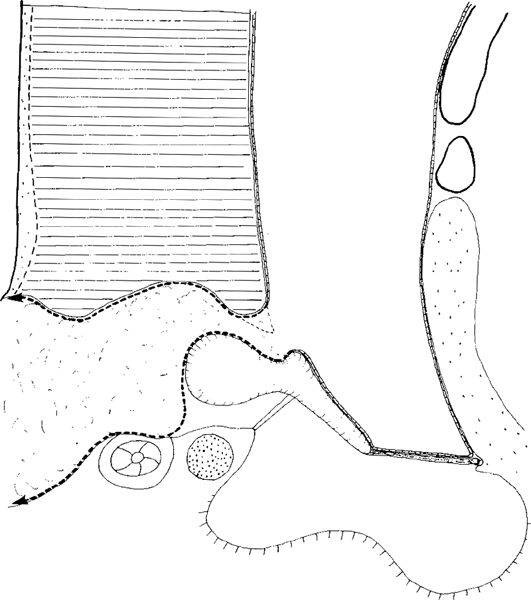
Fig. 18 Side view of a Bondy’s operation in a case with large attic cholesteatoma. All bone from the posterosuperior canal wall up to the middle fossa dura plate is removed (hatched area), together with the lateral membrane of the cholesteatoma sac (dashed line). The cholesteatoma is marsupialized, with wide access to the small open cavity. The ossicular chain is intact, and the medial cholesteatoma membrane is adherent to the medial aditus and antrum walls
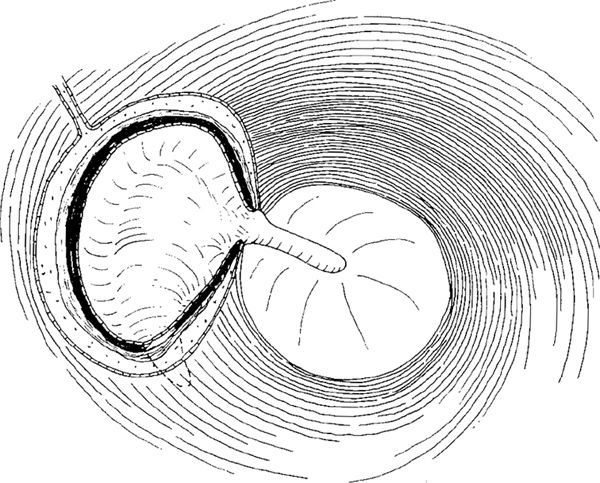
Fig. 19 Atticotomy with removal of a small part of the bony bridge, marsupializing a small attic cholesteatoma. Its medial membrane continues from the Shrapnell’s membrane region and covers the malleus head and incus body. The tympanic cavity is not entered, and the exposed bone will soon be covered with the ear canal skin
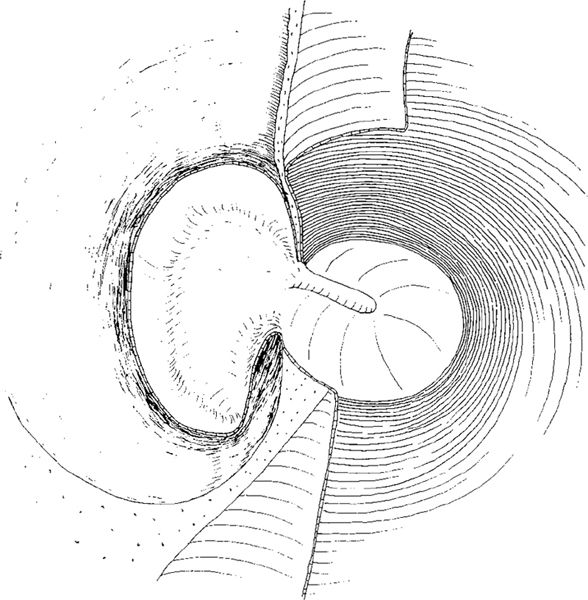
Fig. 20 Large atticotomy with removal of the bony bridge in an attic cholesteatoma. Extensive drilling of the superior ear canal wall is performed, and the cholesteatoma is marsupialized. The medial wall of the cholesteatoma sac covers the head of the malleus and the body of the incus. The cholesteatoma is not adherent to the lateral wall of the semicircular canal, providing good ventilation of the antrum through the tympanic isthmus. After replacement of the canal skin flaps, the denuded bone will be reepithelialized, providing good migration from the attic region
Cortical Mastoidectomy
The cortical mastoidectomy (Schwartze 1873) is a transcortical opening of the mastoid cells and the antrum. It is the initial stage of any transmastoid surgery of the middle ear, inner ear, facial nerve, endolymphatic sac, labyrinth, internal auditory canal, and various procedures on the skull base for removing skull base tumors. The extent of the mastoidectomy depends on the main operation and the access it requires.
The term simple mastoidectomy is usually used for drainage of a mastoid abscess. The bony meatal wall remains intact, and is relatively thick medially. The anterior attic in simple mastoidectomy is not exposed, and only the superior aspects of the malleus head and incus body, as well as the prominence of the lateral semicircular canal, are visualized. The cavity walls are usually not polished, and the mucosa is widely preserved (Fig. 21).
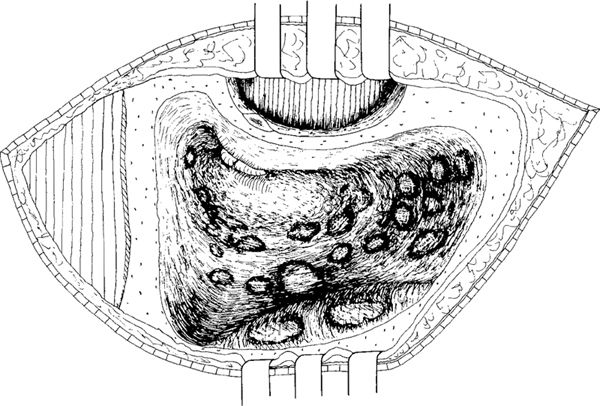
Fig. 21 Simple cortical mastoidectomy in a retroauricular approach. The antrum and the mastoid cells are opened. The bony meatal wall is intact but thick, because the small cells of the ear canal have not been removed. The lateral semicircular canal, the malleus, and the incus are just visible. The lateral attic wall is not opened, neither nor is the anterior attic. The ear canal skin is elevated only laterally to identify the spine of Henle. The ear canal is not entered from behind
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


