 n traditional cyclodialysis, an incision is made in the sclera some distance from the limbus to reach the suprachoroidal space. Through this scleral slit, an instrument introduced into the suprachoroidal space enters the anterior chamber after breaking the scleral spur. The scleral spur is broken for about 2 mm on either side of the entry point. The ciliary body detaches from the sclera, and a cleft is created that allows the fluid to freely enter the suprachoroidal space. From there the aqueous is supposed to flow through the sclera to the subconjunctival space. Cyclodialysis using the Fugo blade follows along the same lines, but in a different and more effective manner, as described below.
n traditional cyclodialysis, an incision is made in the sclera some distance from the limbus to reach the suprachoroidal space. Through this scleral slit, an instrument introduced into the suprachoroidal space enters the anterior chamber after breaking the scleral spur. The scleral spur is broken for about 2 mm on either side of the entry point. The ciliary body detaches from the sclera, and a cleft is created that allows the fluid to freely enter the suprachoroidal space. From there the aqueous is supposed to flow through the sclera to the subconjunctival space. Cyclodialysis using the Fugo blade follows along the same lines, but in a different and more effective manner, as described below.
CASE STUDY
Case 1: Buphthalmos
The patient was 5-year-old suffering from buphthalmos. The eye had suffered trauma and had become a painful blind eye. There was no light perception in the affected eye. The child had been in severe pain for over a month and was getting no relief from medication. The parents were desperate to end the child’s suffering, even if that meant that the eye had to be removed.
The eye was hard. There was blood in the anterior chamber, and a streak of blood lined the back of the cornea at the site of a huge tear in the Descemet membrane. We performed surgery as described below.
Surgical Technique
- Use a 100-µm Fugo blade tip to make a hole in the conjunctiva close to its attachment to the cornea. Balloon the conjunctiva with lignocaine injected with a cannula through the hole.
- Make a large conjunctival incision close to its corneal attachment, again using a Fugo blade (Fig. 33.1). In our case, there was no bleeding.
- Retract the conjunctiva upward (fornix-based) for almost 7 to 8 mm.
- Roughly judge the location of the angle of the anterior chamber by visual inspection; you can also judge it by transillumination with fiber light. In our case, we needed to incise the sclera 4 to 5 mm posterior to the chamber angle.
- Use a 500-µm Fugo blade at low power and energy settings to make an approximately 1.5-mm-long gutter on the sclera parallel to the limbus. Deepen the gutter slowly until the ciliary body is visible. Carefully ablate any remnant of sclera to provide a sharp and clear edge.
- Introduce a long, thin cannula under the anterior edge of the scleral gutter. Advance the cannula gradually, hugging the sclera, until it reaches and then breaks the scleral spur. Extend the spur break for about 2 mm on either side. In our case, some blood-stained aqueous issued from the scleral gutter.
- Inject air into the anterior chamber through the same route.
- Make a 500-µm hole in the wide limbus.
- Trypan blue dropped on the scleral gutter and the anteriorly placed hole is rinsed away by the draining aqueous.
- Suture the conjunctiva back to the cornea.
Figure 33.2 shows functioning cyclodialysis after the procedure.
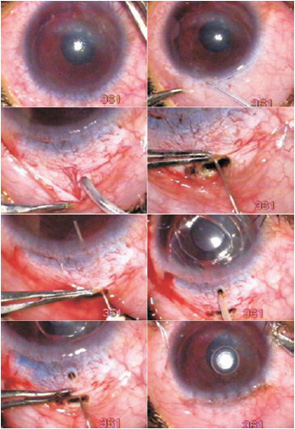
Figure 33.1. The ballooned conjunctiva is incised with Fugo blade. A 500-µm Fugo blade tip is used to make a scleral gutter. Cyclodialysis is done with a long 30-gauge cannula. A 500-µm track is made at the limbus, over the cyclodialysis track. A cannula passed under the sclera appears at the limbal hole before passing into the anterior chamber. The conjunctival flap is sutured back.
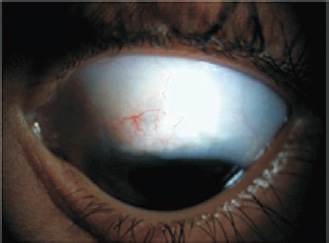
Figure 33.2. Functioning cyclodialysis in a case of buphthalmos (Case 1).
Case 2: Deformed Anterior Segment
If the cyclodialysis cleft and the scleral gutter remain open, a filtration track will begin functioning. To facilitate aqueous flow, a 300-µm Fugo blade tip can be used to ablate a subscleral groove by moving the activated tip from the edge of the scleral gutter into the anterior chamber. The activated tip is directed anteriorly toward the sclera as it moves toward the anterior chamber. Entry into the anterior chamber is confirmed by the appearance of cavitation bubbles within the chamber. We treated a 65-year-old patient with pseudophakia who had a deformed anterior seg- ment from earlier antiglaucoma operations. The patient suffered bouts of pain and had a high intraocular pressure. The steps of the operation are given below.
TECHNIQUE
Anesthesia
Administer facial and retrobulbar block.
Surgical Technique
- After making a bloodless puncture with a 100-µm Fugo blade tip, balloon the conjunctiva with saline. Make an 8-mm-long incision in the conjunctiva with the same tool, as close to the limbus as possible.
- Retract the conjunctiva to expose the sclera (Fig. 33.3).
- Use a 500-µm Fugo blade tip to make a scleral gutter approximately 1.5 mm long to reach the ciliary body. Perform ablation at medium power and a high energy setting.
- Because the scleral pit has steep walls, bevel the upper edge of the scleral pit to facilitate the next step.
- Insert a cyclodialysis spatula under the anterior edge of the scleral gutter and traverse the suprachoroidal space, breaking the scleral spur and entering the anterior chamber. Do not break the scleral spur on either side, as is usually done. When the spatula is withdrawn, the aqueous fluid does not flow out, so the scleral pit remains dry.
- Make a gutter with a 300-µm Fugo blade tip on the underside of the sclera from the scleral pit to the anterior chamber. Ablate the anterior edge of the scleral gutter and advance the tip toward the anterior chamber, pressing it toward the sclera at all times to create a channel underneath it. Once the anterior chamber is reached, withdraw the ablating tip. The aqueous starts flowing from the anterior chamber to the scleral pit.
- A drop of trypan blue over the scleral pit is washed away by the draining aqueous.
- Suture the conjunctiva.
- A drop of trypan blue over the scleral pit is washed away by the draining aqueous.
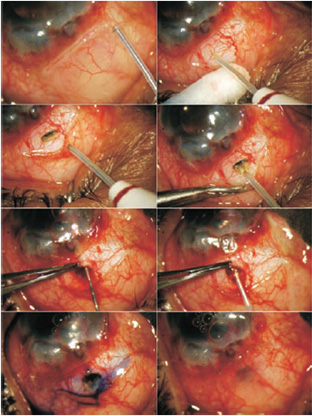
Figure 33.3. The conjunctiva is incised with a 100-µm Fugo blade tip. The scleral gutter is created and the upper edge of the scleral pit is beveled using a 500-µm tip. A cyclodialysis spatula separates the sclera from the ciliary body and enters the anterior chamber. The 300-µm tip of Fugo blade follows the same track, but also ablates the undersurface of the sclera. The fluid flows out as the tip is withdrawn. Trypan blue dye gets washed away. The conjunctiva is sutured back.
This technique can be used to introduce a seton or glaucoma valve tubing in the suprachoroidal space.
This procedure does not resemble classical cyclodialysis. Instead, a filtering track has been made between the anterior chamber and a gap in the sclera at the site of the gutter. Aqueous fluid can reach the suprachoroidal space through the hole created by the Fugo blade in the angle of the anterior chamber. It can spread out or pass out of the scleral gutter.
Insertion of the cyclodialysis spatula and, especially, the 300-µm Fugo blade tip are greatly facilitated by first beveling the superior edge of the gutter.
The scleral gutter approach has been used to drain both dark suprachoroidal hemorrhage and pale yellow suprachoroidal fluid in cases of choroidal detachment.
Summary
Cyclodialysis was introduced by Heine in 1905.1 It was performed as an alternative to filtering surgery, especially in aphakic eyes, or in combination with cataract surgery. Use of the technique has largely been abandoned, however, owing to its unpredictable results, a lack of improvements to the technique over the years, and the development of better procedures. Use of the Fugo blade, however, has revived the surgeon’s ability to use the suprachoroidal space as a conduit for aqueous fluid in selected cases.
Reference
1. Schaffer RN, Weiss DL. Concerning cyclodialysis and hypotony. Arch Ophthalmol. 1962;68:25–31.
Suggested Reading
Alpar JJ. Sodium hyaluronate (Healon) in cyclodialysis. CLAO J. 1985;11:201–204.
Roy FH. Master techniques in ophthalmic surgery. Philadelphia, Pa: Williams & Wilkins, 1995.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


