 efractory corneal ulcers can sometimes take months to heal. In such cases, corneal transplantation shorten the course of the disease. However, keratoplasty is not possible in some situations, because of either a lack of adequate facilities or the unsuitability of the case. It is also important to rule out predisposing factors, such as diabetes mellitus and immunodeficiency.
efractory corneal ulcers can sometimes take months to heal. In such cases, corneal transplantation shorten the course of the disease. However, keratoplasty is not possible in some situations, because of either a lack of adequate facilities or the unsuitability of the case. It is also important to rule out predisposing factors, such as diabetes mellitus and immunodeficiency.
Corneal healing requires a clean base over which the epithelium can grow and adhere to firmly cover the gap. Sometimes necrotic tissue adheres to the healthy cornea. Infection may be present, but local anti-infective agents may fail to reach the infected site. Oral medication then becomes the sole agent that may control infection to some extent. Medication and infection may come to a standoff, making no further progress in either direction.
On its own, the body’s removal of dead tissue might take weeks or months, in which case the dead tissue/detritus/callus is slowly undermined and broken up by the growing epithelium. But to hasten the healing process, necrotic material must be removed. Cleaning the debris from the corneal ulcer is a serious and delicate process, with the ever-present risk that lurking infection may flare up.
The Fugo blade is useful in managing corneal ulcers.
CASE STUDIES
Case 1: Corneal Ulcer in Uncontrolled Diabetes
A 55-year-old diabetic female patient had a nonhealing corneal ulcer with a hypopyon. She had been under treatment with antibiotics and antifungal agents for over 4 months. A large round central area, the “callus,” was firmly adhered to the underlying cornea. This was her only eye. The patient also suffered from severe cardiac and renal problems. Her diabetes remained uncontrolled despite treatment. We opted to remove the callus as a first step to further treatment (Fig. 41.1).
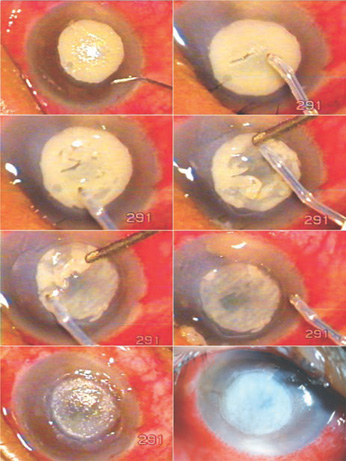
Figure 41.1. The callus is removed under a stream of saline with a 600-µm Fugo blade tip. The final image is the same patient 1 day after surgery.
Surgical Technique
- In our case, we first used a hockey-stick knife to abrade the callus. The callus felt gritty. No progress was made after two attempts with the hockey-stick knife.
- We then used a Fugo blade tip at low power and low intensity, but also without success. We realized that it was because the lesion was completely dry.
- We wetted the cornea and ablated it with the Fugo blade and saw instant results. The callus disappeared in a few seconds. A seemingly healthy cornea appeared from the underneath.
- We placed a bandage lens on the cornea.
Postoperative Management
Local antibiotic and antifungal drops and artificial tears were used postoperatively. It took almost 2 months for the epithelium to cover half of the ulcer. The patient was able to find her way around her home with her little improvement in vision. That was the last information we had on this patient.
Summary
This case demonstrates the utility of the Fugo blade for cleaning corneal ulcers. It is important to note, however, that the ablating tip should be kept moving at all times under a stream of fluid. Avoid using the Fugo blade when the cornea is very thin.
As with mechanical methods, Fugo blade ablation can make the cornea vulnerable to infection flare-up. Frequent local medication is necessary during the early postoperative period. Eye drops should be used even overnight.
Shield Ulcers
Shield ulcers are common in some patients with severe spring catarrh. The allergy may manifest at the limbus, on the palpebral conjunctiva, or in both places. In every case of shield ulcer, eversion of the lid reveals the classic raised knob or multiple cobblestones. These knobs or cobblestones feel like stones as they press on or rub over the soft cornea. This results in epithelial abrasion, which appears as an elongated ulcer that may look clean, but usually harbors dead, white adherent tissue in the floor. These ulcers do not heal unless the allergy subsides on its own or is treated. In tandem with systemic treatment of the allergy by a specialist, the corneal lesion has to be spared recurrent trauma and pressure from the palpebral lesions.
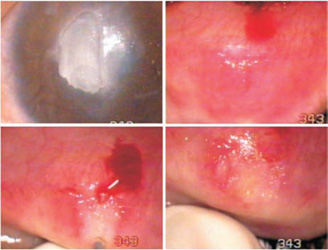
Figure 41.2. A large raised, round, hard nodule, the causative factor in a shield ulcer, is exposed by everting the upper lid. The nodule is rubbed with 600-µm Fugo blade tip until the tarsal lesion becomes flat or even concave.
Manual removal of the palpebral lesions is difficult and accompanied by heavy bleeding. Electrocautery is also traumatic and causes a severe postoperative reaction. The tarsal lesions remain untouched for long periods. The usual approach is to control them with local and systemic steroids.
The Fugo blade is very useful in these cases (Fig. 41.2). Anesthesia consists of everting the lid and injecting lignocaine along the upper edge of the tarsal plate. A single lesion can be decimated in a few seconds. The plethora of cobblestones can be managed as described below.
Surgical Technique
- Expose the palpebral conjunctiva with an everter.
- Use a 600-µm Fugo blade tip at high power and high energy. Treat each cobblestone with one, two, or more pushes of the activated tip. The tip removes the bulk from these hard nodules and flattens them.
- Do not touch the areas between the nodules. The whole process is complete in just a few minutes.
- At the end of surgery, inject dilute triamcinolone along the whole breadth of the conjunctiva, along the upper edge of the tarsal plate (Fig. 41.3). Patients with shield ulcers from spring allergies should be followed by both an ophthalmologist and an allergist.
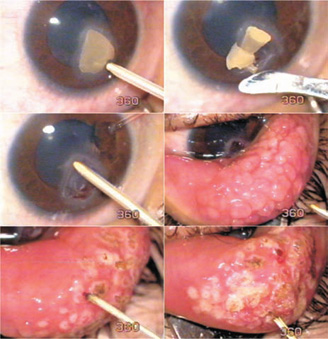
Figure 41.3. The Fugo blade had no effect on the dry callus on this shield ulcer; the callus was removed mechanically. However, the base was cleaned with the Fugo blade and individual cobblestones were “debulked” with Fugo blade ablation.
Suggested Reading
Guttman C. Anterior segment tool proves ideal for many applications. Ophthalmol Times. 2005;30:14–16.
McGrath D. Fugo blade effective tool for multiple surgical applications. Eurotimes. 2008;13:43.
Winn CW. Broad applications seen for electrosurgical instrument. Ocular Surg News. 2001;19:45–46.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


