Corneal Edema
Woodford S. Vanmeter
W. Barry Lee
Douglas G. Katz
Corneal edema may be associated with several pathologic conditions in all layers of the cornea. Consequently, a wide variety of clinical symptoms and etiologic entities present with corneal edema.
Cogan1 previously emphasized that two distinct phenomena encompass the term corneal edema: epithelial edema and stromal edema. They may occur independently or together, produce different symptoms, and have different causes. To properly manage and treat corneal edema, a basic understanding of anatomy and physiology of corneal tissue is required.
Corneal Physiology
The cornea is a vital structure of the eye and has an array of essential functions. Some of the critical functions of the cornea include maintenance of clarity, structural integrity, ocular defense mechanisms, and a powerful converging lens system. The cornea provides two thirds of the eye’s refractive power and must have a smooth surface and a high degree of transparency to refract light rays in an orderly fashion with minimal light scattering. Normally, more than 90% of the incident light is transmitted through the cornea.2 This high percentage of transmittance is the result of physical factors such as a smooth anterior surface, uniform and regular arrangement of the epithelial cells, closely packed stromal lamellae of uniform size, and the absence of vasculature. Factors that influence corneal hydration also affect corneal transparency.
Physical Factors
Epithelium
The corneal epithelium is composed of five to seven cell layers and has a thickness of approximately 50 μ m. In a normal cornea this accounts for about 10% of the total corneal thickness. The cornea is covered by nonkeratinized, stratified squamous epithelium that is constantly sloughed and regenerated. Stem cells located at the limbus produce epithelial cells that migrate centrally and superficially. The epithelium consists of flat cells at the surface, deeper winged cells, and an underlying monolayer of columnar basal cells. The basal cells are responsible for secretion of the basement membrane adjacent to the Bowman layer, which maintains organization of the epithelium and acts as a scaffold on which cells can migrate. One important function of the epithelium is to act as a mechanical barrier to absorption of tears and topical medications or pathogens residing on the ocular surface. Tight junctions between the walls of superficial epithelial cells help maintain the barrier function. Electrical resistance of the cornea predominantly resides in the epithelium, and the resulting impermeability of the epithelium is important in the pharmacokinetics of topical medication penetration.3 The endothelium and stroma have a lower electrical resistance, rendering greater permeability of these layers to the passage of molecules.4
The transparency of the normal epithelium is the result of the homogeneity of the refractive index of cells throughout this cellular layer.5 When epithelial edema occurs, the epithelium loses its homogeneity and the corneal surface becomes irregular. Surface irregularity causes a reduction in vision along with symptoms of glare, photophobia, and halos around light due to light scatter. The effect of epithelial edema on vision depends on ambient lighting conditions. In mesopic conditions, such as the ophthalmologist’s examining room, there may be minimal effect on visual acuity. However, in bright light, edematous epithelium creates light scatter, with marked effects on vision. Surface irregularities caused by epithelial edema are more damaging to vision than stromal edema or opacification. Often the influence of the epithelial surface irregularities on visual acuity is underestimated, whereas the role of stromal scarring and stromal edema is overestimated.
Stroma
The stroma makes up approximately 90% of the corneal thickness and has a composition of uniformly arranged collagen fibrils in lamellae. The collagen fibrils are surrounded by a ground substance made up primarily of glycosaminoglycans, which include keratan sulfate, dermatan sulfate, and chondroitin. The stroma is for the most part an extracellular compartment with keratocytes and nerves accounting for only 5% and 0.01% of its volume, respectively. Water makes up approximately 70% of the stromal volume.
The corneal stroma plays a primary role in maintenance of corneal shape and physical strength. Its constituents, in conjunction with the endothelium, help preserve transparency. Stromal edema may be caused by malfunction of the endothelium and/or epithelium. When the stroma swells, the diameter of the collagen fibrils remains constant. Swelling is caused by an increase in fluid in the ground substance, leading to an increased anteroposterior spatial separation between the lamellae of collagen fibrils.6 Because the collagen lamellae are oriented in the direction of the corneal diameter, only the corneal thickness and not the diameter of the cornea increases with corneal edema.
Endothelium
The endothelium is a monolayer of homogeneous, closely packed, polygonal cells approximately 5 μm thick. The endothelial contributions to maintenance of stromal deturgescence and thus transparency occur by two mechanisms. The first mechanism is the barrier function of the endothelium separating the corneal stroma from the aqueous component. This is a passive barrier that is much less efficient than the epithelial barrier function. The second mechanism is a pump function consisting of active sodium-potassium adenosine triphosphatase (Na-K ATPase) pumps that actively remove fluid from the stroma, pumping it back into the aqueous compartment.
The normal endothelial cell density is 3,000 to 3,500 cells/mm2 in the young adult. The number decreases by about two thirds in elderly patients due to natural attrition.7 Even though human corneal endothelial cells have been shown to proliferate in laboratory cell cultures, they have little or no ability for mitosis after birth in vivo.8 When endothelial loss occurs through aging or trauma, the endothelial response is enlargement and sliding of the existing cells to cover the area previously occupied by the lost cells. When cell loss decreases cell density below a critical number (usually 500 cells/mm2, depending on the health of the cells), corneal edema ensues.
Corneal Hydration
In addition to physical factors, the transparency of the cornea depends on its hydration status. A clear and transparent cornea must remain relatively thin and dehydrated. The corneal stroma of most vertebrates, including humans, swells if placed in aqueous solution because the osmotic load of the glycosaminoglycans in the stroma draws fluid into the stroma. Because the cornea swells only in the anterior-posterior axis, corneal thickness and hydration are linearly related. This linear relation allows measurement of corneal hydration by measurement of corneal thickness. Preservation of adequate corneal dehydration results from the following five factors: stromal swelling pressure (SP), the barrier function of the epithelium and endothelium, the endothelial pump, evaporation from the corneal surface, and the intraocular pressure (IOP). Understanding the mechanisms of corneal hydration is critical in the management of patients with corneal edema.
Stromal Swelling Pressure
The cornea is normally 78% hydrated, but hydration can increase up to 98% when the cornea is placed in aqueous media, with a proportional increase in its thickness. The stromal swelling is due to interfibrillary imbibition of water, not swelling of collagen fibrils. If one extracts the glycosaminoglycans from the stroma, a marked reduction in swelling occurs, indicating that glycosaminoglycans are the major cause of this hydration phenomenon.2 Keratan sulfate and chondroitin both have fixed negative charges that repel each other, and electrostatic repulsion between the negative charges appears to be a major force involved in the swelling. Because the collagen fibrils in the cornea have poor cross-linking, the glycosaminoglycans can expand with very little resistance. This relatively unhindered potential for expansion allows the marked degree to which the stroma can swell.
The potential ability of the stroma to swell decreases as its hydration increases, which limits the amount of swelling. The SP of the normal excised cornea is 50 mm Hg. SP is caused by the presumed anionic repulsion of the glycosaminoglycans, which expands the tissue and permits fluid seepage into the stroma. The negative pressure drawing fluid into the cornea is called imbibition pressure (IP). In excised corneal tissue, the values of SP and IP are equal. However, in vivo, IP is lower than SP because of the compressive effect of IOP on the stroma. The following relationship establishes imbibition pressure: IP = IOP – SP. The compressing effect of IOP on the endothelium in vivo creates an IP of 30 to 40 mm Hg (Fig. 16-1). Water flow occurs from inside the eye as aqueous percolates into the corneal stroma and evaporation occurs from the epithelial side.
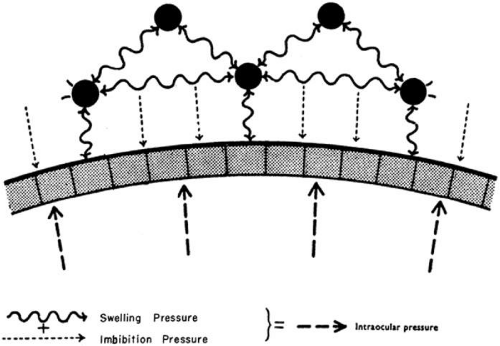 Fig. 16-1. Pressure relationships at the endothelium. (Reproduced with permission from Doughman DJ: Corneal physiology. In Peyman GA, Sanders DR, Goldberg MF (eds): Principles and Practices of Ophthalmology, vol 2. Philadelphia: WB Saunders, 1980.) |
Glycosaminoglycan molecules between collagen fibrils create a high resistance to water flow across the stroma in the normally dehydrated cornea. This resistance is reduced as corneal hydration increases, so that in the more edematous cornea, there is less resistance to water flow across the stroma. There is no lateral flow of water in the cornea except at the limbus.9
Barrier Function of Epithelium and Endothelium
Both the epithelium and endothelium act as semipermeable membranes, creating a barrier to diffusion of electrolytes and to the flow (not diffusion) of water. The epithelium offers twice the resistance to flow of water compared to the endothelium, and relative resistance to diffusion of electrolytes is 200 times greater in the epithelium than in the endothelium.10 Therefore, the epithelium constitutes a relatively impermeable membrane. The ultrastructural basis for this impermeability comes from the tight junctions known as zonula occludens that seal the intercellular space between the superficial epithelial cells.
By contrast, gap junctions bridge the intercellular space at the apical end of the endothelial cells.11 Permeation of water and diffusion of small ions into the stroma from the aqueous is due to the semipermeable nature of the endothelium and is driven by the IOP and negative IP of the stroma. The interaction of all these forces on the hydration of the corneal stroma is shown in Figure 16-2. Factors that affect barrier function are listed in Figure 16-3.
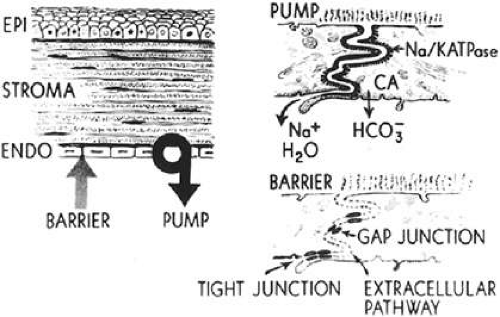 Fig. 16-2. Location of corneal endothelial metabolic pump and barrier. (Reproduced with permission from Waring GO, Bourne WM, Edelhauser HF et al: The corneal endothelium. Normal and pathologic structure and function. Ophthalmology 89:546, 1982.) |
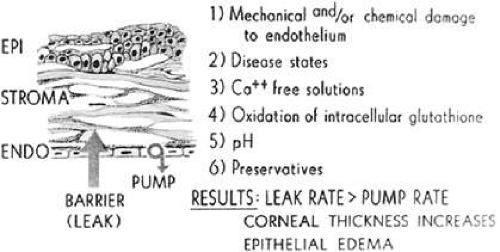 Fig. 16-3. Factors that affect barrier functions. (Reproduced with permission from Waring GO, Bourne WM, Edelhauser HF et al: The corneal endothelium. Normal and pathologic structure and function. Ophthalmology 89:546, 1982.) |
Endothelial Pump
A constant amount of fluid leakage occurs across the endothelium from the anterior chamber, a finding that suggests that another mechanism aids in maintaining corneal deturgescence. The cornea has been observed to thicken in cooled enucleated eyes, whereas subsequent warming promotes thinning to the original thickness.12 This “temperature reversal” of hydration requires oxygen and does not occur in the presence of metabolic inhibitors, such as ouabain, which block cation transport.13,14 Deturgescence with warming indicates that there is an active transport of water and/or electrolytes from the stroma to maintain normal corneal hydration. Furthermore, after the epithelium has been removed, the temperature reversal effect still occurs, showing that the metabolic pumps exist within the endothelium.13 Evidence now points to ion transporter complexes within the endothelium that facilitate the passive secondary movement of water from the stroma to the aqueous.
Although the active transport of sodium and potassium ions may play a role in the endothelial pump, the major component of the pump is the active transport of bicarbonate ions into the aqueous humor.15 A negative electrical potential exists on the aqueous side of the endothelium, suggesting the bicarbonate anion, rather than the sodium or potassium cation, is responsible for the fluid transport across the endothelium.16 The endothelial pump is dependent on oxygen, glucose, carbohydrate metabolism, and ATPase (Fig. 16-4). Dactinomycin, ouabain, and oligomycin are potent inhibitors of this system. Factors that influence the endothelial pump function are listed in Figure 16-5.
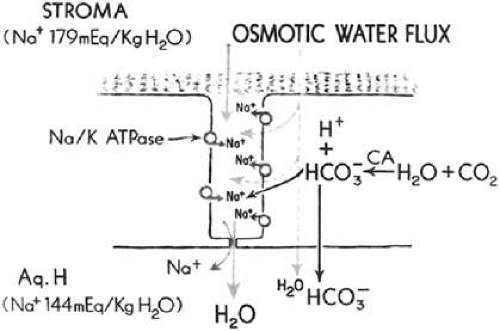 Fig. 16-4. Corneal endothelial pump mechanism. (Reproduced with permission from Waring GO, Bourne WM, Edelhauser HF et al: The corneal endothelium. Normal and pathologic structure and function. Ophthalmology 89:546, 1982.) |
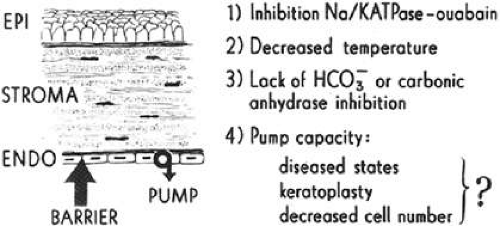 Fig. 16-5. Factors that affect pump function. (Reproduced with permission from Waring GO, Bourne WM, Edelhauser HF et al: The corneal endothelium. Normal and pathologic structure and function. Ophthalmology 89:546, 1982.) |
Evaporation from the Corneal Surface
Evaporation was shown to play a major role in the thinning of rabbit cornea.17 However, only 4% of thinning occurs in humans as a result of osmotic extraction of fluid due to tears made hypertonic by evaporation.18 This loss of fluid from the stroma through the epithelium is readily replaced by aqueous and therefore plays little role in corneal dehydration.
Intraocular Pressure
Elevated IOP can cause epithelial edema, but it is not associated with a change in corneal thickness. Ytteborg and Dohlman19,20 showed that when the IP becomes positive—that is, when the IOP exceeds the SP—epithelial edema ensues. Microcystic changes may occur in several settings. One case involves high IOP and normal stromal SP and thickness, as in glaucoma. The other setting occurs with a normal IOP and low stromal SP, such as that seen in the corneal edema of endothelial dystrophies. Stromal edema may follow microcystic epithelial changes.
In summary, maintenance of normal corneal hydration is achieved by the barrier function of both the epithelium and endothelium, preventing excessive imbibition of water from the tears and aqueous. In addition, the active transport of some anions and cations contributes to the normal corneal thickness with obligatory transport of water out of the cornea via the endothelial pump.
Clinical Entities
Any insult to the cornea that compromises endothelial cell function may lead to corneal edema. Various factors, such as trauma, inflammation, degenerations, or dystrophies, have the potential to disturb the endothelium. Various causes of cornea edema are listed in Table 16-1 according to etiology. The common denominator for all of these conditions is clinical stromal and/or epithelial edema, which may be caused by endothelial dysfunction or by physiologic situations that exceed the barrier and pump capacity of the endothelium.
Table 16-1. Clinical Entities of Corneal Edema | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Corneal Edema with Normal Endothelial Function
Transient corneal edema may occur with an anatomically correct and physiologically functioning endothelium in transient circumstances. These situations develop because the corneal stroma accumulates more fluid than normal. If an influx of fluid into the stroma overcomes the effective ability of the endothelial pump to deturgesce the stroma, corneal edema may occur and may remain as long as the underlying source of edema persists.
Persistent Epithelial Defect
Persistent epithelial defects represent one way in which corneal edema occurs despite a normally functioning endothelium. Chronic, persistent epithelial defects may initially present with decreased vision from corneal edema localized to the area of the defect. Infectious keratitis, if present, can alter the pH of surrounding corneal tissue exacerbating corneal edema.
Because the epithelium serves as a semipermeable membrane that is 200 times more impermeable than the endothelium, a barrier for diffusion of electrolytes and the flow of fluid from the tear film into the stroma exists. If the epithelium is removed and replaced with a glued-on rigid contact lens, no increase in stromal thickness is seen.21 The etiology of corneal stromal edema in persistent epithelial defects is initially associated with abnormal lamellar structure due to imbibed fluid from the tear film. In later stages, collagenolysis from tear film enzymes can cause loss of the epithelial barrier, cause alterations in stromal pH, and retard the normal deturgescent forces of an otherwise healthy endothelium.
Increased Intraocular Pressure
Another example of corneal edema in the face of an intact and functional endothelium occurs in acute glaucoma. As discussed earlier, elevated IOP combined with normal stromal SP in the presence of a normal functioning endothelium may initially compress the stroma with or without epithelial edema. However, persistent elevated IOP drives fluid across the endothelium, creating edema of both the epithelium and stroma, as seen in acute angle-closure glaucoma. Although increased IOP in itself does not disrupt the barrier function, a greater pressure gradient forces more fluid across an intact barrier, decreases the efficiency of the endothelial pump, and can result in increased corneal thickness.22
Primary Endothelial Disease
Primary diseases of the endothelium can compromise endothelial function by adversely affecting both the barrier and the endothelial pump function. Corneal edema may result from a decrease in endothelial cell function, cell number, or both. Entities called primary endothelial diseases are seen in patients with no history of trauma to the cornea and no previous intraocular surgery. There are three disorders in this group of primary corneal endothelial conditions: (i) congenital hereditary dystrophies (e.g., CHED), (ii) adult endothelial dystrophies (e.g., Fuchs endothelial corneal dystrophy [FECD]), and (iii) acquired (e.g., corneal endothelial [ICE] syndrome). Of these, Fuchs dystrophy is by far the most common.
Fuchs Endothelial Corneal Dystrophy
History
Ernest Fuchs,23 professor and chair of ophthalmology at the University of Vienna, described bilateral central corneal clouding in 13 elderly patients in 1910. This entity he referred to as dystrophia epithelialis corneae has now become known as Fuchs endothelial corneal dystrophy (FECD). Fuchs suggested that changes in the endothelium of his patients were similar to those that he had noted in patients following traumatic intraocular surgery or prolonged glaucoma.23 Kraupa24 in 1920 and Vogt25 in 1921 hypothesized that the endothelial changes observed with the slitlamp may precede the epithelial disease. Kirby26 and Gifford27 referred to the disorder as an endothelial dystrophy of the cornea, whereas Stocker28 suggested the name endothelial and epithelial dystrophy of the cornea.
FECD is an inherited, bilateral but often asymmetric, noninflammatory disorder in which the corneal endothelial cells develop morphologic and functional abnormalities that lead to varying degrees of epithelial and stromal edema with corneal guttae. Pain and decreased vision are frequent subjective findings. Vogt25 first coined the term corneal gutta in 1921 to describe a “droplike excrescence of the posterior surface of the cornea.” Guttae (Latin: [noun] = drop; guttate [adjective] = droplike) represent collective excrescences on the endothelium seen with slitlamp biomicroscopy. Guttae may be present without corneal edema in stage 1 of FECD. They may also form secondarily to inflammatory conditions involving the cornea. However, peripheral corneal guttae, known as Hassall-Henle warts, are not associated with FECD. They occur without corneal edema or decreased endothelial cell count and are a manifestation of aging.29
Clinical Manifestations
FECD can be grouped into four recognized categories.30,31,32 The four stages usually evolve gradually over a period of 25 years and, like other corneal dystrophies, are bilateral yet often asymmetric.
The first stage is marked by the onset of corneal guttae, usually in the fourth decade of life. Slitlamp biomicroscopy shows central corneal guttae, a variable amount of pigment dusting on the posterior corneal surface, and a thickened, beaten-metal appearance of Descemet membrane by direct illumination and specular reflection in later stages. The focal excrescences on the endothelial layer initially in stage 1 may become more numerous and confluent. Individual gutta may be completely lost in the beaten-metal appearance of the endothelial surface (Fig. 16-6). As the disease progresses, the guttae spread to the periphery. The first stage is usually recognized only retrospectively or as an incidental finding because patients have no corneal edema and are asymptomatic.
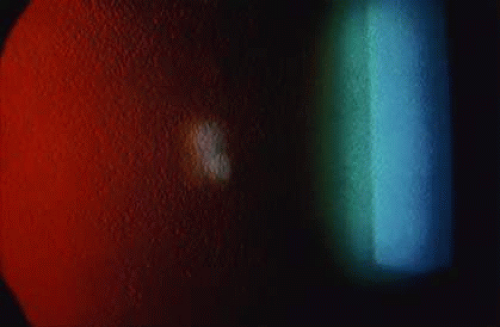 Fig. 16-6. Slitlamp photograph of corneal guttata from retroillumination in Fuchs endothelial dystrophy. |
In stage 2, patients have a painless decrease in vision and symptoms of glare and halos around lights, which are usually more severe on awakening. These symptoms are primarily caused by varying degrees of epithelial and stromal edema. Epithelial edema can be seen as small droplets (bedewing) on slitlamp retroillumination. Decreased evaporation of tears during sleep causes increased tear osmolarity and promotes increased edema and decreased visual acuity on awakening. As guttae become more confluent in the center of the cornea, an opaque posterior collagenous layer can result in a thickening of the underlying Descemet membrane.
Stage 3 develops after epithelial microcysts coalesce to form bullae. The bullae eventually burst and produce varying amounts of pain, hence the name bullous keratopathy (Fig. 16-7). Wrinkles in the Descemet membrane known as striae develop as the cornea thickens posteriorly because of stromal swelling. These striae form when the cornea swells as a result of shortening in the arc of the Descemet membrane from limbus to limbus. As the microcystic epithelial vesicles break, foreign-body sensations and severe pain ensue along with more extensive corneal epithelial disruption. Recurrent corneal erosions, microbial ulceration, and persistent pain may occur during this stage.
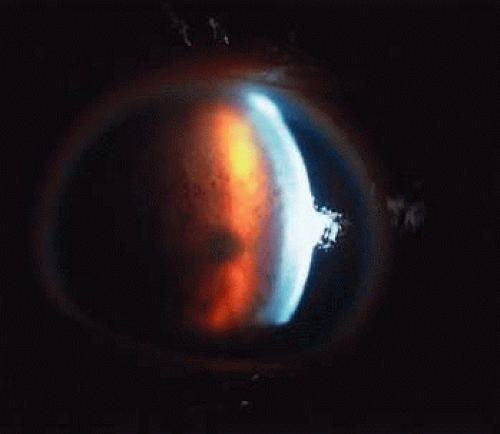 Fig. 16-7. Bullous keratopathy in stage 3 Fuchs endothelial dystrophy. |
The fourth and final stage of FECD is marked by the development of subepithelial pannus along the epithelial basement membrane (Fig. 16-8). The degenerative pannus markedly reduces vision, but at the same time, it reduces painful epithelial bullous formation and promotes relief from pain. Although the epithelial edema is reduced, the stromal edema persists. The scar tissue from the pannus stabilizes the epithelial layer and leads to patient comfort and pain relief despite marked thickening of the cornea.
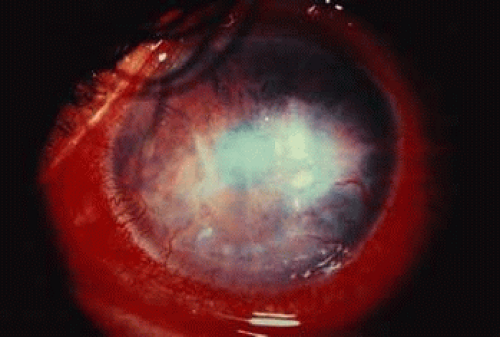 Fig. 16-8. Slitlamp photograph of extensive fibrovascular pannus from stage 4 Fuchs endothelial dystrophy. |
Epidemiology
FECD, beyond stage 1, occurs with a 3-to-1 ratio of women to men. Expressivity of the disorder is more pronounced in female patients.6,32 Although the incidence of FECD has not been reported since Fuchs original description, several studies have determined that 3% to 18% of all patients have asymptomatic corneal guttae.33,34,35 Lorenzetti et al36 in 1967 studied 2,002 eyes in 1,016 patients, looking for a relation between guttae and FECD. They found that 31% of patients younger than age 40 years had guttae, and 70% of patients older than age 40 years had corneal guttae. Of this 70%, only 3.8% had greater than stage 1 FECD and only 0.1% had epithelial edema or bullae.
Although corneal guttae have been linked with familial inheritance patterns since 1939, recent studies have confirmed the autosomal dominant inheritance of corneal guttae and FECD.6,32,37,38,39,40 Krachmer et al41 examined the relatives of 228 patients with corneal guttae and found 38% of patients’ relatives older than age 40 years were affected. Studies by Magovern et al40 and Rosenblum et al6 concluded that FECD is indeed an autosomal dominant disorder with 100% penetrance and variable expressivity.
Histopathology
The underlying pathologic mechanism in FECD is dysfunctional and diseased endothelial cells. This dysfunctional state can increase the corneal thickness from the normal average of 520 μ m to 1,000 μ m or more.42 Additional investigations suggest alternative abnormalities within the cornea may add to the effects of dysfunctional endothelium in causing FECD. Aberrant apoptotic regulatory molecules within stromal keratocytes may play a role in the pathogenesis of this disease, whereas other investigators have suggested abnormal mitochondrial DNA as a possible inciting agent in FECD.43,44
In the normal cornea of a middle-aged person, the Descemet membrane is 12 μ m thick and consists of type IV collagen. The Descemet membrane is composed of an anterior banded portion, which is 3 μ m thick, and a posterior nonbanded portion of variable thickness. The thickness of the nonbanded component averages 9 μ m in adults, but increases from 3 μ m at age 20 years to 10 μ m at age 80 years as a result of continuous secretion by the endothelium throughout life. Clinically evident corneal guttae create thickening of the Descemet membrane, viewed in prepared specimens as focal densities from confluent excrescences or warts.45
In patients with FECD, the posterior nonbanded portion of the Descemet membrane is attenuated or absent because the dysfunctional endothelial cells produce abnormal banded collagen instead of normal collagen. The posterior banded layer in FECD accounts for most of the increased thickness of the Descemet membrane (Fig. 16-9). Bourne et al46 reported that a posterior nonbanded layer is normally found in the cornea of patients older than 20 years, so the presence of a posterior banded layer suggests abnormal endothelial function starting at an early age. Diseased endothelium can secrete 110° banded portions in focal areas of the Descemet membrane, and consequently a localized abnormality may account for the Hassall-Henle warts and/or corneal guttae. Additional disease may result in secretion of collagen that is so disrupted that it forms a nonbanded appearance. Different areas of the Descemet membrane can reflect different mixtures of nonbanded (normal) and banded (abnormal) portions of collagen secreted by the endothelium in different areas of the same cornea.
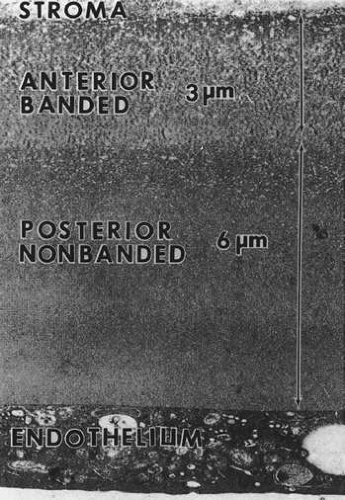 Fig. 16-9. Electron microscopic image of a normal posterior cornea. In Fuchs endothelial dystrophy, the posterior nonbanded layer is abnormal and a posterior banded portion is abnormally present. |
Additional irregularities may be found in the corneal stroma of FECD. Edematous widening of the interfibrillar spaces alters the structure of the collagen lamella within the stroma and decreases its transparency. In the advanced stages of FECD, vascular connective tissue is found between the epithelial basement membrane and the Bowman layer, with fingers of fibrous tissue produced by fibroblasts that protrude upward into the epithelium, and may encapsulate islands of epithelium. The fibrous tissue formation causes other complications, such as epithelial erosions, microbial ulceration, and corneal vascularization.
The thickened Descemet membrane makes the beaten-metal appearance of the corneal endothelium seen centrally in the early stages of the disease. On specular microscopy, the endothelial cells are large and lose their hexagonal appearance. They become quite thin as the cell area increases to cover the posterior surface of the cornea with a diminishing number of cells. However, they constantly maintain a complete and intact covering over the posterior cornea. Fewer cells are present to maintain corneal deturgescence. The metabolic demands on the thinner cells become relatively increased in each cell, thus exacerbating the stress and causing corneal decompensation.
Two-dimensional scanning fluorophotometry demonstrated no difference in the endothelial permeability between patients with mild corneal guttae, advanced corneal guttae, and normal age- and sex-matched controls.47,48 Moreover, an altered Na-K ATPase pump rate in the endothelium of patients with advanced guttae was found, suggesting that a decreased pump rate may be the earliest defect seen in FECD. Subsequent studies demonstrated that Na-K ATPase pump site density is decreased as well.49,50,51,52 These studies suggest that diminished pump function, rather than increased permeability, is the cause of corneal edema in FECD.
Treatment
Stage 1 FECD requires no treatment, as the patients by definition are asymptomatic. Initial treatment for the early stages of FECD consists of medical management to alleviate symptoms. Dehydration techniques, such as desiccation with topical hyperosmotic preparations and dehumidification of the environment, may provide temporary improvement in symptoms of mild cases. Ultimately, surgical management is warranted with either endothelial keratoplasty (EK) or penetrating keratoplasty (PK) with EK representing the treatment of choice in most cases. Penetrating keratoplasty can be considered in cases with significant scarring that would limit vision despite resolution of corneal edema or painful bullae. (Treatment options for corneal edema are discussed later in the chapter.)
Posterior Polymorphous Dystrophy
History
Posterior polymorphous dystrophy (PPMD) is an autosomal dominant inherited, bilateral disorder of the posterior cornea. PPMD was initially described by Koeppe53 in 1916 and later characterized as a dystrophy by Theodore37 in 1939. The clinical appearance can vary dramatically even between affected family members. Most cases are asymptomatic, with no reduction in visual acuity, but the expression of the disease is quite variable and some patients may develop stromal edema and secondary epithelial edema that causes severe and permanent impairment in visual acuity.54
Clinical Manifestations
Posterior polymorphous dystrophy can manifest as three distinct patterns within the cornea. The most common corneal finding on slitlamp biomicroscopy is a small, discrete, round gray vesicular lesion within an otherwise clear cornea. On high magnification, the lesions appear as focal indentations or “pox marks” on the endothelium. A second less common presentation includes band lesions and small, diffuse gray endothelial opacities in the posterior cornea at the level of the Descemet membrane and the endothelium. Third, larger geographic lesions representing a coalescence of grouped vesicles may be found in the same region of the cornea. These large lesions can result in corneal edema (Fig. 16-10), although small lesions may remain asymptomatic. The posterior corneal findings correspond to abnormal deposits of collagenous tissue on the posterior surface of the Descemet membrane, which is irregular and thin in localized areas.30,55 Additional anterior segment findings may be present in conjunction with the corneal edema, and congenital corneal edema has been reported as well.54,56,57
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


