 or the cornea to maintain hydration, transparency, and metabolism, fluid must move throughout the stroma. But does the fluid move because of diffusion only between the stroma and the limiting membranes on both sides, or is there a more efficient channel system? Is the cornea kept transparent by simple dehydration or hydration only, or is there a more efficient system that handles the cornea’s metabolic requirements? For all practical purposes, the cornea is transparent, so it is difficult to visualize any channels that may run through it.
or the cornea to maintain hydration, transparency, and metabolism, fluid must move throughout the stroma. But does the fluid move because of diffusion only between the stroma and the limiting membranes on both sides, or is there a more efficient channel system? Is the cornea kept transparent by simple dehydration or hydration only, or is there a more efficient system that handles the cornea’s metabolic requirements? For all practical purposes, the cornea is transparent, so it is difficult to visualize any channels that may run through it.
My colleagues and I have been studying the conjunctival lymphatics for many years. We have demonstrated conjunctival lymphatics by injecting trypan blue under the distal subconjunctival area. Further research revealed that injecting the dye in the peripheral cornea, rather than in the subconjunctival area, made the lymphatics even more apparent. We also tried to chart lymphatics in the cornea. To demonstrate channels in the cornea, we injected trypan blue in the corneal stroma close to the limbus in painful blind eyes undergoing glaucoma surgery. A small ball of the dye could be created locally. At the edges of the ball, small projections of the dye were visible toward the center and the periphery, but there was whitening of the cornea due to pressure from the injected fluid. Slit-lamp examination did not show positive proof that the dye was moving toward the center, but the dye did disappear toward the periphery within a few days, proving that at least centrifugal fluid movement in the cornea was present. Visualization of the corneal channels has not yet been documented.
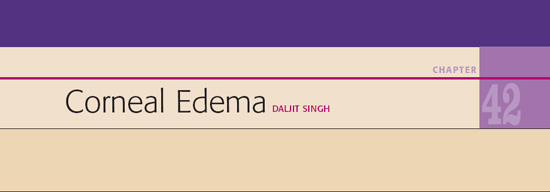
At one point, while studying pictures of conjunctival lymphatics, I found that the dye that had filled them had also created a thin circular line in the periphery of the cornea. The line could not be the Schlemm canal, because it was anterior to the angle of the anterior chamber (Fig. 42.1). On another occasion, during an enucleation procedure, dye was injected with great force into the cornea some distance from the limbus. The dye filled a ring-like space along the limbus (Fig. 42.2).
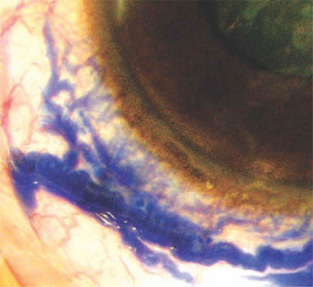
Figure 42.1. Dye injected into the peripheral cornea demonstrated not only the conjunctival lymphatics but also a blue arc in the corneal periphery.
One would expect any form of invisible corneal channels, if present, to be transparent and similar to sinusoids, rather than definitive vessels like arteries and veins. But suppose a corneal pathology renders the corneal tissue translucent or semi-opaque, thus making the channels visible, just as the transparent limbal lymphatics become visible when slight pigment is around them?
This possibility occurred to me when I first saw a young patient with keratoglobus who had an opacity in the center of the cornea. Prominent networklike, darkish lines divided the large nebular corneal opacity into many geometrical compartments. The lines were nearly uniform in size and became fainter and then disappeared toward the transparent peripheral cornea. They did not appear to be any kind of pathology, but were visible because of the tissue changes around them. On optical section they were seen to be in the stroma. The endothelial side was normal. We have been watching this patient for over 9 years; his corneal condition remains the same (Fig. 42.3).
A case of postoperative striate keratitis also sheds light on the existence of the corneal channels. Corneal edema is present, and some sort of channel network is visible. Optical section shows that the channels are in the corneal stroma. The appearance is not attributable to changes in the Descemet membrane. How does so much postoperative keratitis/edema disappear in a matter of hours or days? This probably occurs because the channels in the cornea act like flood drains, as they do elsewhere in the body (Fig. 42.4).
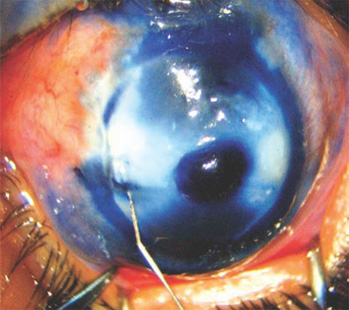
Figure 42.2. Trypan blue injected into the cornea has assumed a circular form inside the limbus.
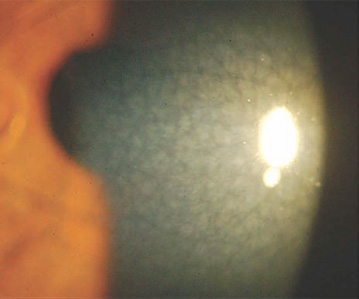
Figure 42.3. Slit-lamp view in a 10-year-old patient with megalocornea. A network of channels is visible in the central and paracentral parts of the cornea. The flashlight could highlight only a part of the opacity.
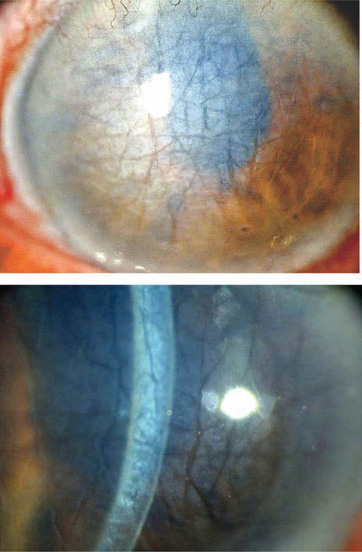
Figure 42.4. A case of severe striate keratitis showing island formation due to the appearance of a network of corneal channels. The optical section shows that they are located in the deep corneal stroma. They also show anterior connections.
We soon learned that the best place to study corneal channels is the area in and around the arcus senilis. The semi-opacification of the arcus highlights the channels. The pattern of the channels is practically the same as in the case of keratoglobus described above. The channels go right up to the lucid interval of arcus senilis. Many of the network channels terminate in the lucid interval, which is lucid seemingly because it has more sinusoidal channels than elsewhere. An optical section of a lucid interval shows a roughly triangular shape, with the base toward the periphery and semi-opaque plates of the corneal tissue on both sides (Fig. 42.5–42.7).
It is probably that even finer channels have so far escaped our notice. If we examine cases of nondescript keratitis under high magnification, we see very fine feathery structures. If these are the finest branches of the corneal sinusoidal channels, they could permeate elements of the corneal tissue (Fig. 42.8).
Fluid flows from the cornea in myriad lymphatic channels in the limbus. Their corneal ends disappear into the corneal periphery and their proximal ends merge into the conjunctival lymphatics. It is not farfetched to say that continuity exists between the corneal sinusoidal system and the limbal and conjunctival lymphatics. One can liken the eyeball to a sponge, with the porosity of the channels varying from one tissue to the next. We have been trained to study the tissues histopathologically. When we do not find a structure, it is supposed not to exist. At present, the corneal channels can be studied only in vivo under a slit-lamp microscope (Fig. 42.9 and 42.10).
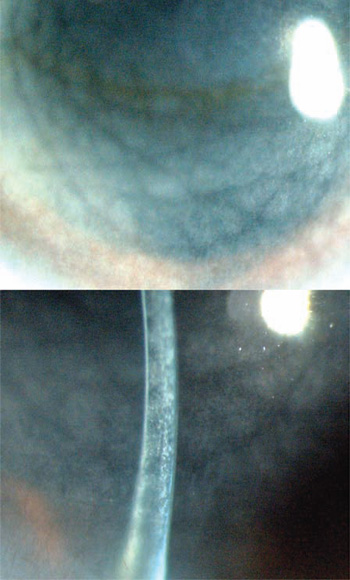
Figure 42.5. A profusion of large and small network channels in an 82-year-old patient. Optical section shows that the wider channels are situated in the deeper layers and that they have connections anteriorly.

Figure 42.6. Network of corneal channels. Notice a periodic merging of the channels into the lucid interval.
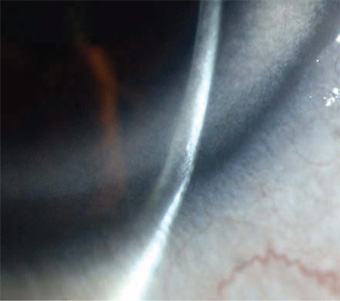
Figure 42.7. Optical section through the corneal periphery. The arcus senilis shows a prominent lucid interval. Fine channels in the arcus and lymphatics at the edge of the lucid interval are also visible.
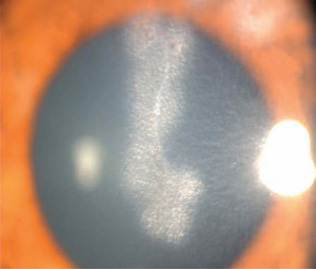
Figure 42.8. The finest chinks in the corneal structure are visible in this particular form of stromal keratitis.
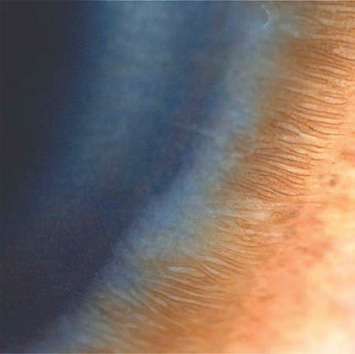
Figure 42.9. Numerous lymphatics appear over the arcus senilis and at the edge of the lucid interval.

Figure 42.10. The relationship between the limbal lymphatics and channels in lucid interval and arcus senilis.
Relationship to the Intra-ocular Aqueous
When such a dense network exists close to the limbus right on top of the Schlemm canal, it is inconceivable that connections do not exist between them. We do not have photographic proof of interconnecting channels, but we have a clinical situation that points to the existence of that connection, as discussed below.
The cornea becomes edematous in cases of acute glaucoma. The moment the pressure is released by paracentesis, the cornea clears up within seconds. This change could not occur without the assumed channels and their connections to the source of raised intraocular pressure. Why do many advanced cases of open-angle glaucoma, with intra-ocular pressures as high as 50 mm Hg or greater, not show corneal edema? It is possible that the channels system has been adapting and increasing the flow along the channels, so that the cornea remains transparent, while the optic disc continues to excavate.
Also, what is the function of limbal capillaries? Do they function the way they function in the rest of the body? We imagine a regular formation of lymph around the cornea that nourishes it through a network of channels. Following this theory, then, fluid movement is dynamic activity, making the cornea a living and throbbing entity, rather than a piece of transparent tissue.
Corneal Decompensation
Fluids do not stay still in the body, and the cornea is no exception. Every heartbeat moves fluids throughout the body. Fluid loads increase or fluid movement is retarded by local causes, and these manifest as edema or decompensation. The presence of edema reduces the transfer of oxygen toward the endothelium, further damaging the endothelium. When the endothelium is at fault, this vicious cycle has to be broken; the standard solution is a full-thickness corneal graft.
In many situations, a corneal graft is either not available or is not performed for personal, social, or medical reasons. At such times, it is possible to help the patient by making new channels to improve or increase drainage of the cornea. Vertical ablation channels/pits are made with the help of the Fugo blade. These ablation pits drain the posterior layers of the cornea toward the anterior layers; from there the fluid is picked up by the more superficial drainage channels and carried to the limbal–conjunctival system and ultimately to the general circulation.
Ablation Pits for Corneal Edema
Management by creating ablation pits is indicated in cases of bullous or nonbullous keratopathy resulting from corneal decompensation, when either corneal graft material is not available or the patient is medically unfit for corneal graft surgery or cannot afford it. The technique is described below.
TECHNIQUE
The corneal thickness is visually estimated on optical section with a slit-lamp microscope. The more sophisticated methods are pachymetry and optical coherence tomography. This is important because a proper length of Fugo blade ablating tip is required in order to avoid the danger of perforation during surgery. A 100-µm tip, about 350 to 400 mm long is selected for surgery. The chosen tip is bent to meet the ergonomic needs of the surgeon.
Anesthesia
Topical anesthesia is enough for this surgery.
Surgical Technique
- Creation of the pit with the Fugo blade starts at the periphery of the cornea. Make 8 to 12 pits close the limbus. Because the Fugo blade tip has a stopper at the preselected length, the danger of perforation is avoided. Select medium power and energy settings. A pit is instantly created as the activated tip is pressed into the cornea.
- Make the second row of ablation pits inside the outer row.
- Make the third row approaching the edge of the pupil. Leave the pupillary area untouched.
Some patients have thick scarred epithelium loosely attached to the corneal stroma. In such cases the epithelium should be removed. Keep in mind the remaining thickness of the cornea mind when dealing with such a case.
CASE STUDIES
Case 1
This 85-year-old, very poor patient traveled over a thousand miles to see me, some 18 years after I had implanted an intra-ocular lens in his remaining seeing eye. This time, the patient presented with a frank case of corneal decompensation. The only conceivable treatment was a full-thickness corneal graft. However, I did not have a suitable facility to perform the procedure, nor was there one available anywhere in the state. Regardless, the patient could not have afforded it anywhere because of his inability to pay.
At the time, I was looking into the concept of corneal channels. By this time, too, I had had 2 years of experience using the Fugo blade. I knew that it would ablate tissues without collateral damage. The patient and I were in a hopeless situation. I thought: Why not try draining the cornea with Fugo blade pits? I explained my plan to the patient and his grandson, and both agreed readily.
First we tried hypertonic saline every 2 minutes for 1 hour. The cornea cleared to some extent, but it was obvious that not much could be achieved through this approach, so we went ahead with the ablation pit approach.
Surgery was done by making multiple pits in the cornea as described above. The cornea appeared somewhat clear 4 hours after surgery. Hypertonic drops were instilled every hour. On the 5th day after surgery the condition was even better. By the 10th day after surgery, the patient could walk about freely without assistance. The endothelial-cell count 10 days after surgery was 458 cells per cubic millimeter, as determined using a Bioptics (high-powered microscope) contact-type specular endothelial microscope.
We sent the patient home and requested that he return after 2 months, if possible. His health was not good and I expected never to see him again. However, he did return, and we were delighted with what we saw. He had a perfectly clear cornea in which the position of Fugo blade pits was marked by gray spots. His corrected vision was 6/12. The endothelial-cell count had risen to 980 cells per cubic millimeter. He kept coming for 4 more years. Transparency of the cornea and good vision persisted, and his endothelial-cell counts hovered around 1000 cells per cubic millimeter (Fig. 42.11).
Case 2
A 70-year-old patient presented with full-blown corneal decompensation after about 20 years of lens implant surgery. Treatment corneal pits made with the Fugo blade resolved the edema in about 3 months. Her best vision was 6/6 and the endothelial-cell count was 680 cells per cubic millimeter (Fig. 42.12). She did not return to the clinic.
Summary
Over the past 6 years we have performed this corneal pit treatment on more than 40 patients with all grades of corneal decompensation severity. Regardless of the cause of the condition, every patient has improved to some extent, and a few to a great extent. Pain and grittiness lessened or disappeared in cases of bullous keratopathy. Corneal edema is reduced or completely disappears, with consequent improvement in vision. Patients’ visual improvement has been constant over years of follow-up. Endothelial-cell counts have risen as the corneal condition improves. Some patients have been treated more than once. Depending on the visual demands of the patient, he or she can be referred for cornea transplantation at any time. Fugo blade pits do not interfere with any kind of corneal procedure.
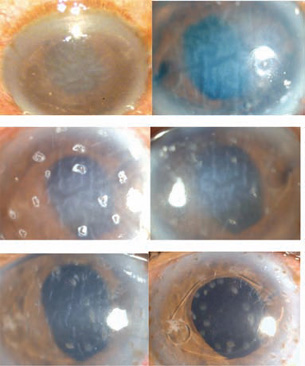
Figure 42.11. This 85-year-old patient with corneal decompensation (Case 1) improved slightly with hypertonic saline. Fugo blade pits on the 1st, 5th, and 10th days after surgery show rapid improvement. The last image, taken 2 months after surgery, shows complete clearing of the cornea. The marks of the Fugo blade tip are visible.
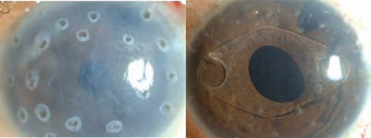
Figure 42.12. A 70-year-old patient (Case 2) with corneal decompensation 1 day and 3 months after surgery.
It is a common belief that the number of endothelial cells is fixed. This is most probably not true. Real life is more dynamic. We have seen endothelial-cell counts increase after patients stop using contact lenses and after removing lenses supporting dislocated irises. Using a Bioptics contact type specular endothelial microscope, we have seen evidence of amitotic cell division close to the site of endothelial injury. We have studied the corneal endothelium immediately after photorefractive keratectomy and in the following days. The endothelial damage increases with increasing degrees of refractive error treated. The process of repair and recovery starts soon. During this period, we frequently see evidence of amitotic cell division. It seems that endothelial-cell recovery plays an important part in the improvements noted after treating corneal decompensation with Fugo blade pits.
Fugo blade pits are made in a matter of minutes. Little medication is required after surgery, and immune complications present no risk, as with corneal grafts. This treatment and its great benefits can be extended to every patient for whom a corneal graft is not possible.
Suggested Reading
Singh D, et al. The conjunctival lymphatic system. Ann Ophthalmol. 2003;35:99–104.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


