Conventional Squamous Cell Carcinoma
Conventional squamous cell carcinoma (SCC) is the most common malignant diagnosis made based on biopsy specimens from the upper aerodigestive tract. In fact, it may be the most common diagnosis of any type rendered on biopsy specimens from this area. This chapter discusses the epidemiology and clinical aspects of the disease, the histologic features of conventional SCC, and some difficulties that can be faced with biopsy specimens. Specific variants of SCC that generally lead to more diagnostic difficulties are discussed in Chapter 5.
EPIDEMIOLOGY
SCC of the upper aerodigestive tract is a disease of older individuals, especially of men. A few notable exceptions occur (Epstein-Barr virus [EBV]-related nasopharyngeal carcinoma and human papillomavirus [HPV]-related oropharyngeal carcinoma); however, more than 90% of cancers of the oral cavity and pharynx and more than 95% of cancers of the larynx are diagnosed in patients older than 45 years.1,2 According to the National Cancer Institute, slightly more than 35,000 cancers of the oral cavity and pharynx and nearly 13,000 cancers of the larynx were diagnosed in the United States in 2010. In the same year, there were approximately 7,800 deaths from oral and pharyngeal cancers and approximately 3,600 deaths from laryngeal cancers. Thus, the combined incidence of these cancers is similar to that of pancreatic cancer, whereas their mortality is similar to that of renal cell carcinoma.
Stage is the most important prognostic factor for these tumors.1,2 The overall 5-year relative survival rates for laryngeal and oral/pharyngeal cancers were 61%, but were 77% and 82%, respectively, when the diseases were found to be localized. While 57% of laryngeal cancers were localized at the time of diagnosis, only 33% of oral/pharyngeal cancers were.
SCC of the upper aerodigestive tract is strongly linked to the use of alcohol and tobacco products.3,4,5,6,7 and 8 Indeed, using the two products together carries a relative risk of more than 20 for the development of these cancers.6 The risk is dose related, and heavy users are much more likely to develop these malignancies than infrequent or occasional users.8 Furthermore, the cessation of smoking is associated with a decreased risk for the development of these malignancies.
With regard to tobacco products, smoked tobacco is the major culprit.6 Chewed tobacco, however, is also considered to be a risk factor, especially for the development of oral SCCs, although its role remains somewhat unclear, and it carries a significantly lower relative risk for the development of malignancy at all sites when compared with smoking.9 Indeed, some have suggested that individuals should be encouraged to switch from smoked to chewed tobacco to reduce their risk for developing these malignancies.
In recent years, the incidence rate of tobacco product use has declined in the United States. Following this trend, there is now a wellestablished decline in the incidence rate of upper aerodigestive SCCs at sites most commonly related to the use of tobacco products (e.g., the larynx and mouth).
Other risk factors are both familial and environmental.10,11,12,13,14,15,16,17 and 18 Although the data are somewhat unclear, some elucidation has been based on young patients with SCCs who have little or no history of exposure to alcohol or tobacco products. The better understood familial cancer syndromes, including Li-Fraumeni syndrome, Lynch syndrome, and familial atypical mole-melanoma syndrome, with germ line mutations of the genes encoding for the p53 protein, mismatch repair proteins, and the p16 protein all carry increased risk for the development of SCCs of the upper aerodigestive tract.17,18 and 19 Some human leukocyte antigen types are also more prone to develop SCCs, particularly EBV-associated nasopharyngeal carcinomas.10,20,21 and 22
Aside from tobacco and alcohol use, environmental factors include both dietary and infectious factors. Although not commonly chewed in the United States, betel quid (a combination of a stimulant and an alkaloid) has been associated with the development of oral SCC through the development of the precursor lesion, submucosal fibrosis (see Chapter 3).13 Diets deficient in iron can lead to Plummer-Vinson syndrome (dysphagia, iron deficiency, and esophageal webs), which is associated with an increased risk for the development of hypopharyngeal SCC.23 Finally, people whose diets are rich in fruits and vegetables may be at decreased risk for the development of SCC of the upper aerodigestive tract.14
EBV is believed to play a role in the development of some SCCs, namely with undifferentiated SCCs.24 These tumors almost always occur in the nasopharynx; however, they can occur anywhere throughout the upper aerodigestive tract. The exact role that EBV plays in the development of these tumors is unclear. EBV-associated tumors are discussed in more detail in Chapter 5.
High-risk HPV also plays an important role in the development of SCCs of the upper aerodigestive tract, especially in younger patients with no history of alcohol or tobacco abuse.25,26,27 and 28 Our understanding of the role that HPV plays in the development of these tumors has progressed quickly over the past decade. We know that these tumors are almost always located in the oropharynx (the palatine and lingual tonsils), although the tumors rarely can occur throughout the entire tract. HPV-related SCCs are most commonly nonkeratinizing or basaloid (see Chapter 5), although they may sometimes be keratinizing or associated with other variant morphologies. In spite of their often high stage at presentation, the tumors appear to have a better overall prognosis than SCCs secondary to tobacco and alcohol use and are more radiosensitive. While the incidence rate of laryngeal and oral SCCs has declined recently, there has been a surge in the incidence rate of oropharyngeal SCCs, leading some to claim that we now have an epidemic of HPV-related upper aerodigestive tract malignancies.29
CLINICAL
Patients who develop SCCs of the upper aerodigestive tract tend to be older and the disease is much more common in men. As noted earlier, exceptions include EBV-related and HPV-related tumors. Also, tumors with chromosomal rearrangement of the nuclear protein of the testis gene (NUT midline carcinomas) occur in patients of all ages (discussed in Chapter 5).30
Patients’ symptoms depend on the location of their tumor and stage of their disease. Most present with the nonspecific findings of a mass lesion, obstruction, pain, and bleeding. Laryngeal lesions are typically associated with hoarseness. Any tumor, especially those that develop in the nasopharynx and oropharynx, can present with metastases, for example, as a neck mass, without symptoms related to the primary tumor. More advanced tumors can present with symptoms secondary to distant metastases or with systemic complaints such as weight loss.
DIAGNOSIS
Although the diagnosis of some variants of SCC can be particularly challenging (see Chapter 5), the recognition of most conventional SCCs is routine. These are infiltrative tumors composed of irregular, often anastomosing nests of obviously squamous cells that show varying degrees of intracellular and extracellular keratin formation (Fig. 4.1, e-Fig. 4.1). Increased differentiation is usually present toward the center of the nests, with the most peripheral cells having a basaloid phenotype with scant basophilic cytoplasm (Fig. 4.2, e-Fig. 4.2). As the cells progress centrally within the nests, their cytoplasm tends to become more abundant and eosinophilic. Extracellular keratin, commonly intermixed with necrotic debris, is often identified at the centers of the nests (e-Fig. 4.3). This is not a firm rule and some degree of atypical maturation is usually seen, with more peripheral cells having increased intracellular or extracellular keratinization and some central cells having a more basaloid phenotype. Furthermore, extracellular keratin formation may be seen anywhere throughout the nests and may even not be present. The squamous nests can vary considerably in size, with some appearing large and cystic, resembling nonneoplastic keratinous cysts (e-Fig. 4.4). Single-cell infiltration may be present and can be very helpful for distinguishing nonneoplastic or noninvasive disease from invasive malignancy (e-Fig. 4.5). The surrounding stroma usually has some degree of chronic inflammation, often with stromal desmoplasia.
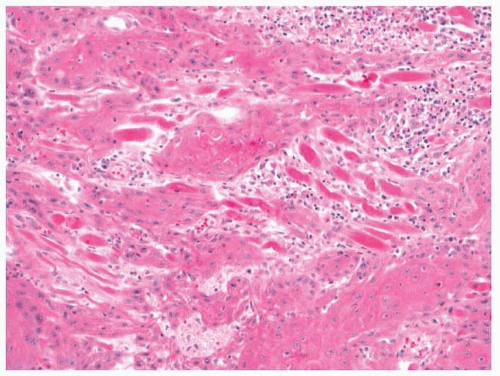 FIGURE 4.1 A squamous cell carcinoma with a typical pattern of infiltration. |
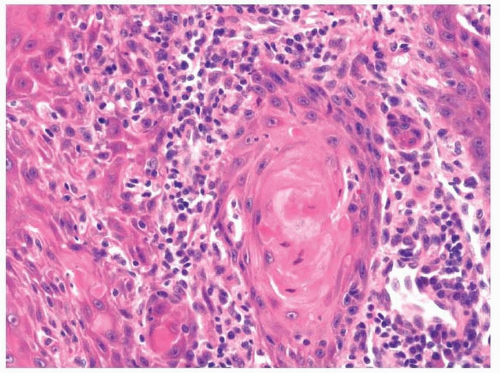 FIGURE 4.2 Maturing, keratinized squamous cells are present toward the center of the infiltrating nests. |
Cytologically, conventional SCCs have cells with varying degrees of differentiation and varying degrees of cytologic atypia. The smaller, basaloid cells have a more undifferentiated phenotype and can appear round with little cytoplasm. Larger cells will have more abundant eosinophilic to clear cytoplasm and typically have a more rigid, polygonal shape. These cells often show artifactual separation from one another, and intercellular desmosomes can typically be identified. Within the cytoplasm of the larger, differentiated cells, intracellular keratin formation and granules can sometimes be seen. The nuclei of the neoplastic cells show moderate to marked differences in shape and size, with irregular contours and vesicular to granular, malignant-appearing chromatin. Prominent nucleoli are usually seen and mitotic figures, including atypical mitotic figures, can usually be found. Necrosis of both individual tumor cells and large portions of tumor is frequently seen with SCCs.
Immunohistochemistry is not commonly used for the diagnosis of conventional SCC. Neoplastic cells will be reactive with antibodies to pankeratins and, specifically, with antibodies to CK5/6, 8, 13, and 19. Immunoreactivity with antibodies to CK7 may be seen in some cases; however, immunoreactivity with antibodies to CK20 is almost never seen. Most cases are immunoreactive with antibodies to p63 and variable immunoreactivity can be seen with markers of molecular abnormalities such as p53, cyclin Dl, and retinoblastoma protein. The use of these molecular markers has been proposed by some to help distinguish neoplastic from nonneoplastic disease.



