Chapter 119 Contact lenses for children
Types of lenses
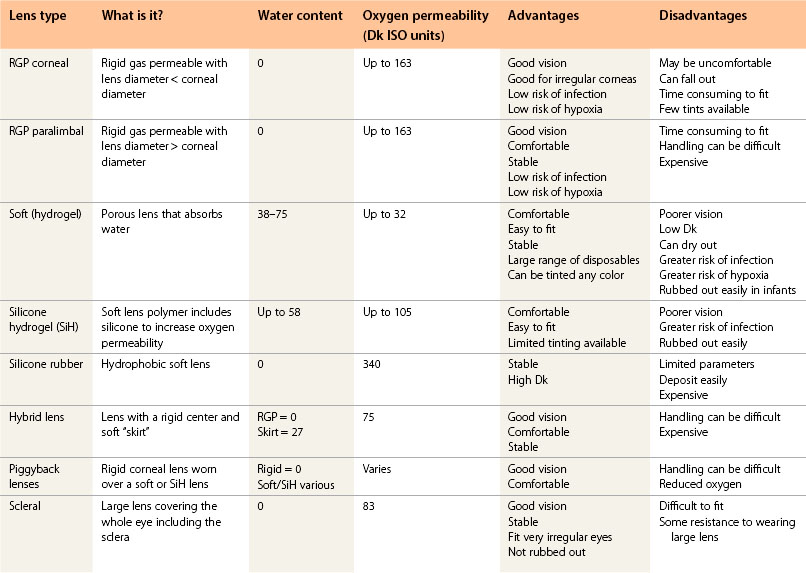
Any type of lens can be fitted. The choice of lens depends on the condition being fitted, when the lenses are going to be worn, and the limitations of each material, design, and parameter range (Table 119.1). Rigid lenses have a name for being uncomfortable, but two drops of a local anesthetic can overcome any problems. By the time the anesthetic has worn off, the lens has usually settled.
Hygiene
Stress the need for strict hygiene with a simple, effective, regimen. Solutions that could cause an allergic response should be avoided. Preservative-free solutions may be preferable. The rub and rinse step prior to lens soaking greatly decreases the risk of infection and is recommended by the FDA.1
High prescriptions and aphakia
Contact lenses provide a clearer field of vision than spectacles.2 High myopes have better visual acuity with contact lenses than with spectacles, which reduce the image size. However, high hypermetropes and aphakes have better acuity in spectacles because the image size is larger.2 This can lead to disappointment when aphakes with poor acuity are fitted with contact lenses.
Unilateral ametropia
Contact lenses reduce aniseikonia for both unilateral axial and refractive myopia,3 but amblyopia is usually present and highly myopic eyes (over –9.00 D) do not usually respond well to patching;4 only 32% of unilateral aphakes achieve vision greater than 0.6 logMAR5 and, because binocularity is rare, children do not notice much difference when wearing a lens, making compliance poor. However, wearing a contact lens often reduces the angle of any strabismus.
Aphakia
Congenital cataracts
Procedure for lens fitting
Determine keratometry (K) and corneal diameter using a printed corneal gauge. Alternatively, fit the lenses empirically using the average radius of a neonate – 7.1 mm.6
What lens to fit?
• Soft or silicone hydrogel (SiH) lens with the back optic zone radius (BOZR) approximately 0.3 mm flatter than average K and total diameter ≥2 mm larger than corneal diameter. With microcornea, larger lenses will help center the lenticular portion over the pupil. These lenses are not available from most multinational companies so order tailor-made lenses from a smaller manufacturer. Infants may rub their lenses out and lenses are prone to dry out and mislocate or fall out.7
• Silicone rubber lenses do not dry out and are not easily rubbed out. They are fitted on flattest K and assessed using fluorescein. The high Dk (oxygen permeability) means that they can be worn overnight in emergencies. The steepest lens is 7.50 mm BOZR, too flat for many aphakes.
• Rigid lenses are rubbed out less often. They can be made of hyper Dk materials. Paralimbal lenses with a decreased edge lift will lessen the risk of the lens becoming dislodged.7 The edge lift may need to be increased when the child is older.
Traumatic aphakia
Intraocular lenses usually give better acuity than contact lenses.8 After trauma, lens insertion can be difficult; spectacles may be preferable.
What lens to fit?
• Rigid corneal lenses where there is corneal scarring to give the best acuity and least risk of neovascularization.
• Paralimbal or large diameter rigid corneal lenses (Fig. 119.1).
• Soft prosthetic lenses if there is aniridia, poor cosmesis and photophobia, but the low Dk increases the risk of hypoxia. Wearing time should be limited to a few hours a day.
Ectopia lentis or dislocated lens
What lens to fit?
• Soft disposable spherical lenses together with spectacles correcting any astigmatism in either eye and a bifocal or multifocal lens for the aphakic eye.
• RGP corneal lenses may give better acuity but aphakic lenses are liable to sit low because the center of gravity of the lens is in front of the cornea. This problem is exacerbated on a flat cornea (Fig. 119.2).

Visual development



