 tosis has many causes. One convenient classification is infantile ptosis and adult ptosis. Ptosis is an indication for conjunctival-route levator plication, whether the ptosis is mild, moderate, or severe. The Fugo blade’s ability to incise and blunt-dissect bloodlessly encouraged me to look for the levator muscle through fornix incisions and to advance the blade to the anterior surface of the tarsal plate. This new technique is called “sutureless conjunctival-route plication of the levator” or simply “Singh levator plication.” (The conjunctival entry incisions are sutureless; however, levator plication requires buried sutures.)
tosis has many causes. One convenient classification is infantile ptosis and adult ptosis. Ptosis is an indication for conjunctival-route levator plication, whether the ptosis is mild, moderate, or severe. The Fugo blade’s ability to incise and blunt-dissect bloodlessly encouraged me to look for the levator muscle through fornix incisions and to advance the blade to the anterior surface of the tarsal plate. This new technique is called “sutureless conjunctival-route plication of the levator” or simply “Singh levator plication.” (The conjunctival entry incisions are sutureless; however, levator plication requires buried sutures.)
Plication can be performed in both infantile and adult ptosis. Most cases of ptosis are uniocular, but in bilateral ptosis, I prefer to do one eye at a time. Plication may or may not work for paralytic ptosis. It is useful for cases of Marcus Gunn ptosis, because the correction of ptosis reduces the range of jaw-wink lid excursion.
TECHNIQUE
Anesthesia
During surgery, double eversion must be performed on the eyelid must undergo double eversion to create considerable pull on the lid. Pull on the muscle is produced as the levator is located, grasped, and brought forward. Because of this, I prefer to give general anesthesia, even for adults.
Surgical Technique
- Perform double eversion of the lid using a Desmarre lid retractor (Fig. 3.1).
- Pass thick nylon stay sutures through at the upper edge of the tarsal plate, one in the center and one on each side at a distance of about 6 mm. The weight of the artery forceps holding the sutures keeps the lid everted.
- Use lignocaine 2% to balloon the conjunctiva over the double-everted tarsus.
- Make three conjunctival vertical incisions about 10 mm long in line with the stay sutures using a 100-µm Fugo blade tip. When this tip crosses a large subconjunctival vessel, bleeding occurs. To prevent this ablate/close all visible blood vessels in the proposed line of incision using a 300-µm tip at low energy. Alternatively, you may start and complete the incision using the 300-µm tip only. This leaves a minor gap in the conjunctiva, which does not affect the surgical result.
- The fornix ends of the conjunctival incisions are undermined toward the orbit.
- The structure directly beneath the incised conjunctiva is Müller muscle, which originates beneath the levator muscle is better and deep to this is the levator muscle. If you pull this muscle anteriorly, the levator muscle can be caught easily in its aponeurosis. Whereas the Müller muscle is red, the levator muscle appears pearly white. The amount of levator muscle you should pull anteriorly depends on the severity of ptosis: The greater the ptosis, the more anteriorly you should pull the levator muscle.
- Pass an 80-µm vanadium steel suture through the levator muscle caught at the end of each conjunctival incision and secure the sutures with miniclamps.
- Expose the anterior surface of the tarsal plate using a 300-µm blunt Fugo blade probe. Expose the surface at the three proximal ends of the conjunctival incisions. Expose the tarsal plate as ablation of the Müller muscle and the underlying stretched aponeurosis of the levator muscle. Start ablation close to the nylon stay sutures, which provide a clue to the depth at which the Fugo blade is working. The most important point is not to ablate the tarsal plate, but only to expose it. Tarsal plate exposure with the Fugo blade is usually bloodless, but if a large vessel is in the way, it will bleed. You can touch the same Fugo blade tip to the bleeding spot to stop the bleeding. Exposing the tarsal plate using the Fugo blade does not burn the tissues, preventing postoperative reaction and edema (Fig. 3.2).
- Next, pass the steel sutures that are holding the levator muscle through the exposed/prepared anterior surface of the tarsal plate. Insert the needle through a partial thickness of the tarsal plate, about 3 to 3.5 mm from the upper edge of the plate, and exit about 1.5 mm from the edge.
- Attach the levator muscle to the tarsal plate with a reef knot in the steel sutures. Do not use excessive force to pull the sutures, or they may cut through the tissue.
- Remove the stay sutures and return the lid to its normal position. When the lid is in its normal position, the sutures are situated on the anterior surface of the tarsal plate, i.e., they do not face the cornea or the bulbar conjunctiva.
- Temporarily tie the lids together with a thick nylon suture—24 hours for adults and 48 hours for children.
- Use lignocaine 2% to balloon the conjunctiva over the double-everted tarsus.
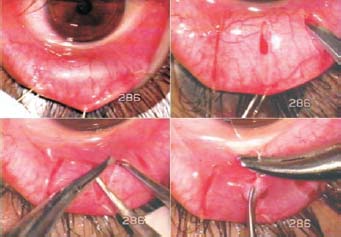
Figure 3.1. The lid has undergone double eversion with a Desmarre lid retractor. Thick nylon stay sutures are passed close to the upper edge of the tarsal plate. The conjunctiva is ballooned with lignocaine, and three vertical conjunctival incisions are made using the Fugo blade. The Müller muscle is pulled anteriorly so that the levator can be grasped. An anchoring suture is passed through the levator muscle.
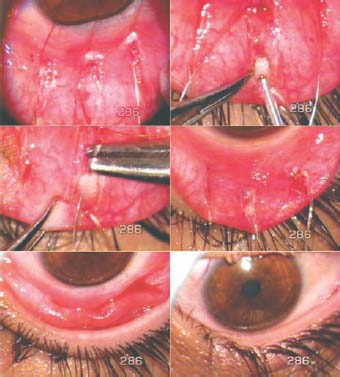
Figure 3.2. The levator muscle is anchored at three points with sutures. The anterior surface of the tarsal is carefully exposed at three places with a 300-µm Fugo blade tip. The levator anchoring sutures are passed through the half thickness of the tarsal plate, at about 3.5 mm from the upper edge of the tarsal plate, then the sutures are tied, and the lid is returned to the normal position. No conjunctival sutures are required.
Postoperative Management
Direct the patient to apply steroid-antibiotic eye ointment three times a day for 15 days and instill artificial tear drops seven to eight times a day for 15 days. Make sure that the patient is able to close the lid. Advise the patient that a pad and bandage should be used overnight or while sleeping for the first few days.
Little or no inflammatory reaction occurs after this surgery, partly because the Fugo blade ablates the tissue without charring it and partly because of the simplicity and atraumatic nature of the surgical technique.
It is important to watch the lid margin for any turning in. This can happen if the levator muscle is attached too far anteriorly from the superior edge of the tarsal plate. Turning in can also occur in very severe ptosis, for which an excess of levator muscle must be pulled out. In this case, the tarsal plate moves up, while the other tissues of the lid tend to hang over the lid margin. Temporary sutures that lift the skin prevent the cilia from striking the cornea. A bandage lens may be worn for a few days if needed.
Summary
My colleagues and I have performed more than 180 of these levator plication operations during the past 5 years. We have had a satisfactory outcome in more than 90% of the cases. When the correction does not meet expectations, we perform additional surgery using plication of the orbicularis oculi muscle. A waiting period of about 3 to 4 months is needed before a second surgery can be done. Examples of some of our results are shown in Figures 3.3, 3.4, and 3.5.

Figure 3.3. A pediatric patient with ptosis in both eyes, and more severe in the left eye. The photos show the patient’s preoperative (Left) and 1 month postoperative (Right) appearance while looking up, looking straight, looking down, and closing her eyes. Lid lag, but no lagophthalmos, is present while looking down.
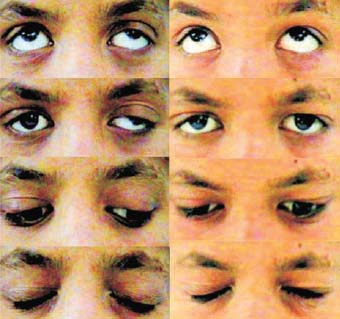
Figure 3.4. Unilateral severe ptosis with good levator function in a 13-year-old patient. The postoperative appearances (Right) are 1 year after the operation. Lid lag, but no lagophthalmos, is present in the operated eye.

Figure 3.5. Residual ptosis after a Fasanella–Servat operation on the left eye. Poor elevation of the left eye was a pre-existing condition. The preoperative and 1 week postoperative results, after levator plication, are shown. The operated eye can be closed easily.
In 1981, Beard stated “All told… well over a hundred operations and variations of operations for ptosis have been reported. This is good evidence that the ‘ideal’ operation has not as yet been devised and probably never shall be. Our present concepts may seem archaic in the not too distant future.”1 About Müller muscle, Beard writes in his preface, “Here is a structure of obvious importance that has been largely disregarded by many of us. This muscle has been ruthlessly excised in many levator resections. It could be that ptosis surgery in the future will be largely aimed at the preservation of this structure.…”
Our goal has been to develop a ptosis surgery technique that:
- involves minimal handling of tissues,
- preserves the Müller muscle,
- may be redone to reduce or enhance the correction,
- does not compromise the ocular tissues for additional surgery by any other currently used surgical technique,
- is applicable to all grades of ptosis, and
- is easy to learn.
Our experience shows that all the points mentioned above are more or less achieved by our technique. Hence, we believe that this new concept of “sutureless plication of levator muscle” is a step toward the realization of an ideal ptosis procedure. The Fugo blade is a major ally in performing the most crucial steps of the procedure in a bloodless manner.
Suggested Reading
Agatson SA. Resection of levator palpebrae muscle by the conjunctival route for ptosis. Arch Ophthalmol. 1942;27:994.
Beard C. Ptosis. St. Louis, Mo: Mosby, 1981.
Berke RN. A simplified Blaskovics operation for blepharoptosis. Arch Ophthalmol. 1954;48:460.
Blaskovics L. A new operation for ptosis with shortening of the levator and tarsus. Arch Ophthalmol. 1923;52:563.
Cohen AJ. Ptosis, adult. Accessed January 3, 2010, at http://www.emedicine.com/oph/topic201.htm.
Iliff CE. A simplified ptosis operation. Am J Ophthalmol. 1954;37:529.
Roy FH. Ptosis: complete classification. Ann Ophthalmol. 2005;37:5–32.
Singh D, Fugo RJ. Orbicularis plication for ptosis, a third alternative. Ann Ophthalmol. 2006;38:185–193.
Singh D, Kaur A, Singh K, et al. Sutureless levator plication by conjunctival route: a new technique. Ann Ophthalmol. 2006;38:285–292.
Suh DW. Ptosis, congenital. Accessed January 3, 2010, at http://www.emedicine.com/oph/topic345.htm.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


