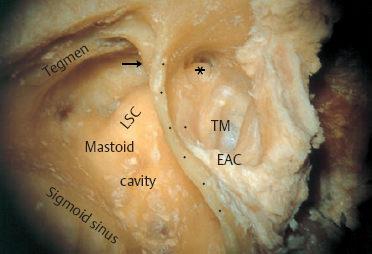
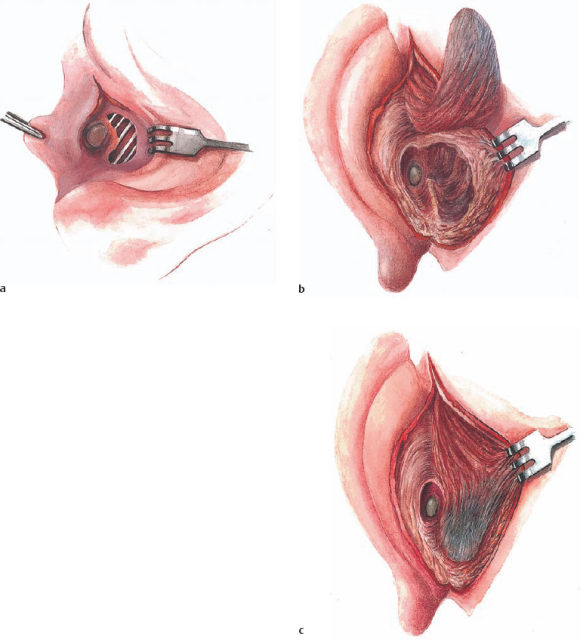
1 Concepts and Principles of Restitutional Ear Surgery Although there are many textbooks and manuals on ear surgery, containing vast amounts of contemporary knowledge and based on statistical evaluations, international controversies in the field continue. There are still different schools teaching their own philosophy and techniques—following tradition rather than the evidence of scientific comparisons between treatment modalities. I am not free of this attitude myself, and to a certain degree I believe it is justified. This is because there are too many variables involved in otosurgical protocols—including specific indications, auxiliary measures, and the skills and aims of the individual surgeon concerned. In addition, statistical results can be misinterpreted, creating prejudice against good alternatives or even discouraging new ideas. Medical history shows that concepts that are fundamentally very sound are often dismissed due to negative initial experience, although after later refinement they become popular and dominant. What this means is that the young otosurgeon should keep an open mind—not relying blindly on state-of-the-art directives, but critically studying the physical and biological significance of published surgical methods. The cardinal question of “why” must never be masked by an impressive report on “how” the author has achieved something. An analysis of one’s own mistakes, from case to case, should be a major source of expertise. This introductory chapter will therefore try to explain the ideas and mechanisms underlying the techniques used, developed, and accepted in my own department. Since reconstructive microsurgery for chronic otitis media provided the basis for all of these, a general discussion of the structural elements of tympanoplasty will be presented, with implications for the management of trauma, malformations, and tumors as well. The use of clear nomenclature is a vital precondition for this type of description; some terms are associated with different meanings in different countries. A brief look at the terminology may therefore help clarify the subsequent text. Everyone who has taken part in an international panel or workshop on ear surgery is familiar with a difficulty frequently encountered in discussions comparing different methods: the audience often misunderstands what is being said because the speaker and listeners are not using the same terminology. The late Professor Jean Marquet organized a special conference solely in order to establish a common nomenclature for the postoperative evaluation of middle ear surgery. Since this goal has still not yet been fully achieved, it may be useful to define certain terms here before going on to explain the procedures. Otitis media refers to an inflammation of the mucosal lining of the middle ear, which in strict terms is in fact a mucoperiosteum. The underlying bone may become affected as a secondary development, giving rise to osteitis, or rarely osteomyelitis. Mucositis may be confined to the tympanic cavity in the form of tympanitis, but it often extends into the retrotympanic spaces in the form of mastoiditis. In clinical practice, however, mastoiditis is used to refer to a complication of otitis media with more or less marked erosion of the pneumatized bone. Both tympanitis and mastoiditis can present as acute otitis media, or can begin and persist as chronic otitis media. In addition to the acute and chronic patterns of bacterial or viral origin, there is a noninfectious form caused by failure of ventilation of the eustachian tube, and this presents with nonbacterial serous or mucous effusion in the middle ear. Otitis media with effusion, and secretory otitis media, are synonymous with this; I prefer the term seromucous otitis media. Incidentally, ventilation defects may also be torpid, resulting in “dry catarrh” in the tympanic cavity, with slightly negative pressure. The term mastoidectomy refers to systematic and complete opening of the mastoid cells, using either an endaural approach or the classic transcortical approach (Fig. 1.1). The goal is to establish free communication among all the complex internal surfaces, not genuinely radical exenteration as is carried out in total resection for malignant disease. For instance, the term mastoidectomy does not cover the handling of the mucosa, preservation of the mucosa, partial removal, or total eradication. The term antrotomy is often used in Europe for the same maneuver—leaving the lining mucosa in its place, but reestablishing reliable drainage via the tympanic cavity. The word ending or suffix -tomy only implies opening, while -ectomy refers to complete removal. Atticotomy is the term for a similar mucosa-preserving opening of the epitympanic recess. Exposure of this recess can be carried out from the external ear canal (anterior atticotomy) or through the mastoid (posterior atticotomy), or can even be performed from above in the course of a middle fossa approach. Anterior atticotomy necessarily removes at least parts of the lateral attic wall, but posterior atticotomy does not. Posterior atticotomy preserves the bone, which was called the “bony bridge” or “scutum” by early middle ear surgeons. S.R. Wullstein (1973) similarly used the term epitympanotomy for exposure of the attic with temporary removal of the scutum. Tympanotomy refers to exposure of the tympanic cavity via the external ear canal (lateral tympanotomy) after posterior circular incision of the drumhead and lifting of a tympanomeatal flap; but this procedure can also be carried out via the mastoid (posterior tympanotomy), or via the middle cranial fossa. Exenteration of the cavity may be termed tympanectomy. A simple incision of the drum membrane for reasons of drainage or endoscopy should not be described as “tympanotomy,” but as myringotomy or paracentesis. Some authors prefer the term “tympanoscopy” for this type of exposure, but this expression only implies endoscopic visualization of the tympanic cavity. According to H.L. Wullstein and his school, the term tympanoplasty (originally proposed by Weschke) covers three types of surgical treatment for chronic otitis media (Wullstein 1968): From this point of view, the aim of tympanoplasty is to achieve biological healing of all the middle ear spaces, with simultaneous improvement in hearing. However, in the contemporary literature, the use of the word “tympanoplasty” has been confined to plastic reconstruction of the tympanic cavity (in Glasscock and Shambaugh 1990, for example). Nowadays, tympanoplastic procedures in the sense intended by Wullstein are therefore described using two or three additional terms—e.g., tympanoplasty with mastoidectomy and meatoplasty. This specification must be accepted as an international trend, and in the present book the term tympanomeatoplasty will be used if plastic remodeling of the external auditory meatus is a basic element of the procedure, together with curative exposure and reconstruction of the middle ear spaces. Meatoplasty or canal plasty refers to plastic reconstruction of the walls of the external auditory meatus. A wall is the solid partition from an adjacent different compartment. This maybe the case anteriorly, against the glenoid fossa; superiorly, against the middle cerebral fossa; or posteriorly, against the mastoid cavity in cases of injury, atresia, etc. The most frequent form of meatoplasty is reconstruction of a defective posterior canal wall over a hollow mastoid in cases of chronic otitis media (Fig. 1.2). However, the term is still often used for the procedure of shaping a posterior canal wall by obliterating a radical mastoid cavity with soft or hard tissues, thereby establishing a massive block of tissue instead of a ventilated mastoid cavity (Estrem and Highfill 1999). It has also been used to refer to simple lining of a radical cavity with grafts (Glasscock and Shambaugh 1990). The endaural approach means entering the external auditory meatus via the auricle, through its natural orifice behind the tragus. This narrow passage may be widened either with an auxiliary skin incision in the tragohelical incisure (Botey 1898), or with an extended skin incision (Heermann and Heermann 1964). The common element in these two procedures is that the fixation of the concha to the mastoid cortex remains untouched. The endaural meatal route can proceed into the tympanic cavity, into the mastoid, or into other compartments of the temporal bone. In the postauricular approach, exposure of the mastoid bone from behind the auricle involves transecting the skin and periosteum in a more or less semicircular curve. This incision can be continued transmeatally to the tympanum, after exposure of the bony orifice of the external ear canal with the spine of Henle and after incision of the posterior canal skin, or it can be followed by transcortical opening of the mastoid. In all cases, the fixation of the concha to the mastoid cortex is transected, and the auricle has to be resutured into its normal position later. Management of the mastoid and other retrotympanic spaces, recently termed mastoidectomy, can be achieved using different approaches. For example, most authors (like Glasscock and Shambaugh 1990) remove a mastoid cholesteatoma using a postauricular transcortical approach on principle. They then only have a choice between the open technique (canal wall down technique) and the closed technique (canal wall up technique) in relation to preservation of the posterior bony canal wall. One of the main aims of the following chapters is to show that the endaural transmeatal approach to the mastoid is a third possible option. As will be seen, this endaural approach is usually carried out as part of a closed technique, with preservation of the lateral attic wall and of the bony bridge, which are parts of the posterior meatal wall. Fig. 1.2 Restitution of the posterior wall of the external auditory canal through preservation or reconstruction of the posterior meatal wall (a), or obliteration of the underlying cavity (b and c) with a muscle-periosteum flap (Palva’s technique). The term lateral approach can be used to cover all routes penetrating into the middle and inner ear or the lower parts of the petrous bone, as well as to the nasopharynx, from a lateral direction—thus passing the external ear canal, the temporomandibular joint, and the greater wing of the sphenoid bone. This type of premeatal access is often included in larger approaches—e.g., infratemporal ones—aiming at the clivus or the sphenoid bone. The transotic approach through the cochlea and labyrinth into the internal auditory canal described by Fisch is also strictly speaking a lateral approach. Definitions of the approaches also need to include the transcervical approach to the lateral skull base. This follows a direction from caudolateral to craniomedial, starting from a superior neck dissection along the great vessels and nerves. It is aimed at the jugular foramen and at the channel of the internal carotid artery, coming from below and proceeding cranially. The term is not very popular, since it overlaps with the terms for other lateral approaches mentioned above. The present book follows Glasscock’s recommendation to combine a transmastoid approach to the jugular bulb with transcervical exposure of the jugular foramen and the internal carotid artery, using a transcervical–transmastoid approach. The term petrosectomy is also often used with different meanings. I prefer to speak of partial petrosectomy and total petrosectomy, reserving the latter expression for complete exenteration of the petrous bone up to the petrous apex, including the middle and inner ear structures.
 Terminology
Terminology
 Goals and Principles of Restitutional Ear Surgery
Goals and Principles of Restitutional Ear Surgery
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


