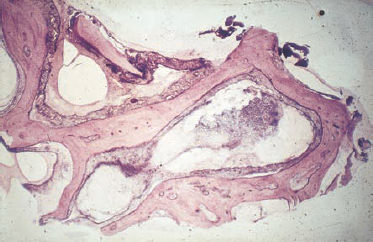
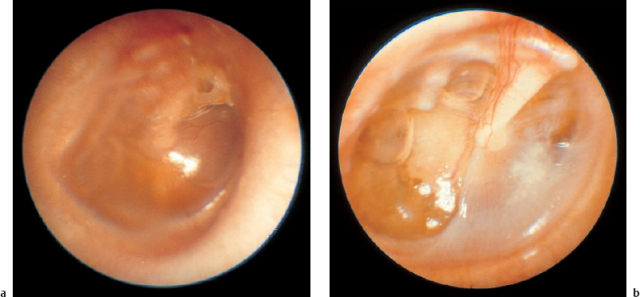
9 Acute Otitis Media and Mastoiditis Acute otitis media is an otosurgical disease that has high complication rates, as well as a wide range of surgical indications. The prognosis is not always easy to predict in individual cases. Physicians in other disciplines such as general medicine and pediatrics—who are often concerned with the treatment of this condition, rather than with thorough diagnosis of it—should be aware of the dangers of masking it and delaying the diagnosis. Four principal types of acute otitis media can be distinguished: Valuable regular updates on the state of contemporary knowledge and research in acute otitis media have been provided by a series of international research conferences on “Recent Advances in Otitis Media,” the proceedings of which are published in Annals of Otology, Rhinology and Laryngology (Anon. 1998). A reading of this update shows clearly that there are marked differences between various authors with regard to the terminology used and the treatment approaches taken. The published proceedings of the Third Extraordinary Symposium on Recent Advances in Otitis Media, held in 1997, also reflect substantial controversies (Tos et al. 1999). In the present Chapter, there is insufficient space to review the countless publications discussing the details of pathophysiology and conservative treatment (a summary is given by Bluestone and Klein 1995). Instead, we have basically outlined the surgical experience and practices in our own department, using a mostly successful regimen. Noninfectious acute otitis media (otitis media with effusion, secretory otitis media) is basically caused by tubal insufficiency of various causes that induces low tympanic pressure, stimulating the mucosa to produce serous or mucous exudates. Apart from conductive hearing loss, the main dangers associated with this condition are transition to an adhesive process, with subsequent development of cholesteatoma, and inner ear depression with a progressive course or with sudden hearing loss. While acute otitis media predominantly occurs during infancy—originating from hyperplasia of the adenoids and tonsils, and more rarely due to rhinosinusitis, cleft pathology, or allergy—its incidence in adults must raise a suspicion of nasopharyngeal lesions such as carcinoma or lymphoma. Nonspecific bacterial acute otitis media is also mediated through the eustachian tube, but in this case, rhinogenic bacterial invasion, originating from rhinosinusitis or adenoiditis, is facilitated by the short and patent tube in the infant. The first phase of this condition is characterized by massive inflammation of the tympanic cavity and drum membrane, followed by spontaneous rupture of the membrane. In the second phase, the process extends into the normally well-developed pneumatic cell system of the temporal bone, leading to mastoiditis. However, involvement of the facial nerve, inner ear, and even of the adjacent dura must be expected if appropriate treatment is neglected. The bacteria involved vary; common microbes are Streptococcus pneumoniae and Haemophilus influenzae, which are isolated in 25–40% of middle ear fluids in acute otitis media. In addition, Moraxella catarrhalis is frequently found (Anon. 1998: 29). Scarlatina is known to cause early total destruction of the tympanic membrane. Specific infections of the middle ear by tuberculosis or syphilis have become very rare. These tend to induce chronic otitis media, rather than the acute syndrome. With the increasingly mixed population in Europe, however, one needs to be attentive to note “rare cases”—including Wegener’s granuloma, which can also mimic acute otitis media. Acute otitis media of viral origin is characterized by nonputrid inflammation of the mucosa and all layers of the drum membrane. A preceding viral infection predisposes the middle ear mucosa to mixed bacterial infection. The most common pathogens are rhinovirus, respiratory syncytial virus, adenovirus, influenza A and B, parainfluenza, enterovirus, cytomegalovirus, and herpes simplex virus (Anon. 1998: 29). The complication rate is higher than with bacterial acute otitis media, and involves sensorineural hearing loss with tinnitus, vestibular insufficiency, and facial paralysis. Concomitant neuritis of the cochleovestibular nerve can be expected in some cases. There are similarities with herpes zoster infection, but the virological classification is unclear in most cases. All forms of viral acute otitis media can cause inflammation of the external and middle ear, as well the sensorineural compartments of the cochleovestibular system. Fig. 9.1 Acute mastoiditis: the histology of the removed cells reveals mucoperiostitis without myelitis. Acute mastoiditis. Although acute otitis media does, of course, also involve the mucosa of the mastoid process to a minor extent, wider invasion of the retrotympanic cell system, leading to blockage of the internal drainage due to inflammatory hyperplasia of the mucoperiosteum with subsequent osteitis, is known as mastoiditis. Bone destruction is propagated via the mucosa-lined cells (Fig. 9.1), in contrast to osteomyelitis, which proliferates via the Haversian channels due to phlebitis. Treatment of the causative infection therefore consists of reestablishing internal drainage and ventilation by reopening the occluded cell system, using the mastoidectomy procedure. If the osteitis extends into the zygomatic arch or into the soft tissues of the neck via the mastoid tip (Bezold’s mastoiditis), the adjacent areas also need to be included in the mastoidectomy. Otitis media with effusion is marked by a sudden or delayed onset of painless hearing loss, autophony, and a sensation of mild aural pressure. Otoscopy demonstrates retraction of the tympanic membrane, or a yellowish shadow behind it (Fig. 9.2). The Politzer maneuver can produce visible air bubbles. The drum membrane may develop marked atrophy, facilitating retraction and adhesion via an initial atelectasis; or can thicken, with fibrous infiltration and calcification (Fig. 9.3). Even hemorrhage may result from the hypobaric irritation of the mucosa, giving the drumhead a dark appearance. Audiometry reveals an air conduction deficit, and tympanometry can measure the barometric distortion of middle ear pressure. Nonspecific acute otitis media produces burning aural pain as the presenting symptom, followed by conductive hearing loss and tinnitus. Giddiness and vertigo are rare. Concomitant upper respiratory disease is frequent. In bacterial acute otitis media, otoscopy shows vascularization of the central areas in the initial stages (Fig. 9.4), and a reddened and thickened drumhead, without light reflexes, after two to four days. Pus may become translucent (Fig. 9.4b) before spontaneous rupture occurs. Rupture provides relief, but it is followed by an ear discharge. In viral acute otitis media, the pale or reddish drumhead is less thickened, but it is characterized by hemorrhagic blisters that often extend into the external auditory canal (Fig. 9.5). Typical of Hunt’s syndrome (herpes zoster oticus) are grouped blisters on a reddened background, combined with palsies of the facial or vestibulocochlear nerve, or both (Fig. 9.6). By the time the patient presents a week later, the classic efflorescence has often changed to crusted erosions, or may already have disappeared. A Schüller radiograph helps confirm mastoid involvement, with either opacification or lucency caused by bone destruction—both of which indicate manifest coalescent mastoiditis (Fig. 9.7). Narrowing of the external auditory canal due to sagging of the posterior canal wall indicates an osteitic perforation, often combined with abtrusion of the auricle (Fig. 9.8). Swelling at the sleeve is due to inflammation of the zygomatic bone. Acute otitis media, and particularly mastoiditis in children, is usually accompanied by an accelerated erythrocyte sedimentation rate and leukocytosis. Fig. 9.2 Acute otitis media with effusion. a The light reflex is distorted by the translucent yellowish effusion. b Persistent otitis media with effusion has led to posterosuperior atelectasis of the tympanum, with bone erosion on the long incudal process.
 Clinical Entities
Clinical Entities
 Symptoms, Signs and Diagnosis
Symptoms, Signs and Diagnosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


