Fig. 4.1
Typical eardrum perforation following tympanostomy tube extrusion
Several issues should be investigated before considering surgical closure of a long-standing eardrum perforation [22]. First, age plays a role. Closure at 5–6 years old, before the child may have outgrown Eustachian tube dysfunction, can lead to recollection of middle ear fluid and conductive hearing impairment, or retraction with potential ossicular erosion or cholesteatoma. Additionally, if the individual still has endogenous (not swimming related) ear infections with intermittent otorrhea, the perforation may well serve as an exit portal and be an asset rather than a liability.
The necessity of using a swim plug for eardrum perforation is controversial. Within the past two decades, recommendations have shifted from always using a plug to situational use depending on the type of water (pool, pond, lake, ocean) and depth of swimming [23]. Currently, most otolaryngologists recommend a plug for non-pool swimming and water exposure below 2–3 ft.
Surgical closure of persistent perforation is typically based on surgeon preference. However, a few guidelines are helpful. First, if the individual has a conductive hearing impairment greater than expected due to perforation alone, the ossicles should be examined as part of the procedure. This requires exploration of the middle ear (tympanoplasty) rather than attempt at closure of the perforation alone (myringoplasty). Second, even in the era of minimally invasive surgery, adequate exposure of the entire eardrum perforation and the size of the ear canal are important factors. If the ear canal accommodates only a 4or 4.5 mm speculum, enlargement of the ear canal or a postauricular approach may be necessary for success. Hearing results after tympanoplasty for perforation are not easily predictable [24]. Chronic middle ear disease may lead to acoustical changes that are not surgically correctable.
Adhesive Otitis Media
Consistent negative pressure due to ongoing Eustachian tube dysfunction acts as a vacuum on the undersurface of the eardrum leading to progressive eardrum retraction. When controlled early enough in the process via ventilation, the ear tube arrests the process. Without ventilation, ongoing severe negative pressure may lead to global retraction forming permanent adhesive scar bands from the undersurface of the eardrum to the ossicles and floor of the middle ear, collapse of the middle ear space and adhesive otitis media or “saran wrap” ear. Surprisingly, this may result in very minimal conductive hearing impairment if sound is conducted through the ossicles and oval window. However, in most cases, there is at least mild hearing impairment. The incus-stapes joint is often eroded and occasionally the stapes itself becomes eroded. Adhesive otitis media usually remains as a self-cleaning ear without formation of granulation tissue or cholesteatoma formation (Fig. 4.2).

Fig. 4.2
Severe eardrum atelectasis after many years of Eustachian tube dysfunction
Treatment recommendations for this situation are controversial. Options include monitoring alone with periodic hearing assessment, placement of an ear tube through the eardrum for ventilation, placement of a subannular ear tube for ventilation [25, 26], and cartilage tympanoplasty [27, 28]. The use of transnasal balloon dilation of the Eustachian tube is currently experimental in adults.
Chronic Otorrhea
Whereas some eardrum perforations remain clean and dry, others may intermittently drain mucopurulent infection [29]. If the ear drains only a few times each year and resolves within 1–2 weeks using antibiotic ear drops, then there is little concern. However, if the drainage persists longer than 3 weeks or resumes drainage soon after cessation, then the ear may have chronic infection within the mastoid cavity or chronically infected mastoid cholesteatoma. Some individuals may have small eardrum perforations with occasional otorrhea during upper respiratory infections. If drainage persists longer than 3 weeks, a bacterial and fungal culture should be obtained to help guide therapy.
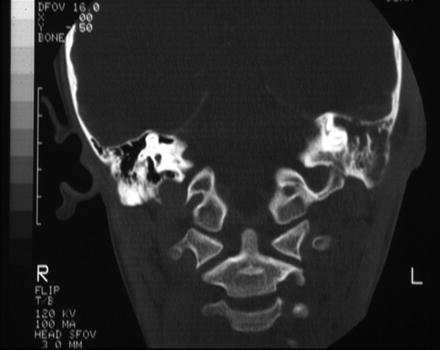
For unremitting drainage, CT scan with contrast of the mastoid may help determine if long-term antibiotics or mastoidectomy may be beneficial. MRI is oversensitive for detection of mastoid disease and does not detect bony defects, as does CT scan.
Ossicular Erosion
Long-term Eustachian tube dysfunction with negative pressure or chronic drainage may lead to erosion of the incus-stapes joint and further erosion of both the incus and stapes bones leading to conductive hearing impairment [30, 31]. Yet, there are no prospective studies addressing how long this process takes to occur and when is the proper time of intervention to arrest this process. Moreover, cholesteatoma formation may erode the ossicles leading to conductive hearing impairment.
Ossicular erosion may occur by direct pressure exerted by the retracted eardrum, ongoing infection with inflammation or enzymatic bony destruction due to cholesteatoma. Commonly, the lenticular process of the incus is involved with incus-stapes disarticulation. Continuation of the process leads to stapes erosion. Usually, the malleus is spared.
Facial Nerve Paralysis
At any time, acute otitis media may cause acute facial nerve paresis or paralysis [35–37]. This is a direct toxic effect of the bacteria rather than an erosive process of the bone surrounding the nerve sheath. Facial nerve weakness is more likely if there is a natural bone dehiscence within the middle ear with a direct toxic effect on the nerve sheath. Treatment is urgent myringotomy with ventilation tube placement and culture-directed antibiotic therapy. Prompt therapy leads to over 95 % return of facial nerve function. However, delayed therapy may impair resolution of facial nerve weakness with residual permanent injury.
Cholesteatoma (Keratoma)
The term cholesteatoma is a misnomer and has no meaning. The term was coined in the 1850s when the thought was that this represented a growth or “oma” of cholesterin. Even though the proper term is “keratoma”: meaning “skin growth,” The literature continues to perpetuate the word cholesteatoma and it seems difficult to purge this from our lexicon (Figs. 4.3 and 4.4).
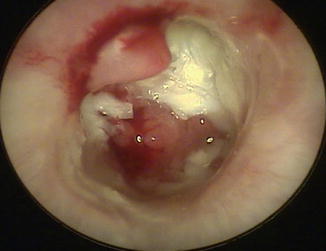

Fig. 4.3
Photo of middle ear cholesteatoma with granulation tissue
Fig. 4.4
Photo of attic retraction cholesteatoma and eardrum perforation
Acquired cholesteatoma may occur in several ways. Classically taught, focal eardrum retraction of the posterior half of the eardrum may extend to and beyond the incus and stapes bones with erosion of the ossicles [38] along with trapping of skin debris and formation of granulation tissue. If instead, or in addition, the posterior, superior portion of the eardrum called the pars flaccida retracts from the attic region behind to the antrum of the mastoid, this is termed an attic retraction cholesteatoma. An attic retraction cholesteatoma does not usually lead to ossicular damage unless there is a concurrent middle ear component tracking towards to incus and stapes. Other mechanisms of cholesteatoma formation include implantation of skin behind the eardrum after repeated eardrum rupture due to acute infection or occasionally due to a surgically created perforation as with ear ventilation tubes. Acquired cholesteatomas may remain clean and dry or may become chronically infected with mixed aerobic and anaerobic bacteria.
The cholesteatoma dissolves bone both by direct extension and by halisteresis (bone resorption through enzymatic destruction). This process may become very destructive with erosion of the bone separating the mastoid from the middle cranial fossa called the tegmen. The bone covering the floor of the mastoid may also erode with extension to the posterior fossa. Infection may then lead to intratemporal, intracranial complications. Treatment is surgical and may require several, staged surgeries for successful keratoma removal and ossicular reconstruction [39–42]. Pediatric ossicular reconstruction is less successful than in the adult population.
Acute Mastoiditis
An acute middle ear infection by definition leads to infection in the mastoid cavity via direct extension through the attic region of the middle ear, which is the portion of the middle ear cavity superior to the eardrum. Therefore, radiographically, the mastoid cavity will be expected to have infection just as the middle ear. However, an acute otitis media with radiographic fluid in the mastoid does not equate clinically with a diagnosis of acute mastoiditis. Rather, the diagnosis of acute mastoiditis depends on clinical findings. Early findings are fever, pain and erythema and edema behind the ear over the mastoid bone equating with the largest air cell of the mastoid called the antrum (Fig. 4.5). Next, as the mastoid diploic veins become engorged and develops venous congestion, the swelling increases pushing the conchal bowl of the ear outward and then downward (proptosis). Internally, the infection dissolves the trabecular network of bony partitions within the honey-combed mastoid cavity leading to coalescent mastoiditis. The cortex may then erode externally leading to a subperiosteal abscess and/or internally leading to an epidural abscess or brain abscess. A Bezold abscess develops when the infection erodes through the mastoid tip into the neck. Gradenigo syndrome is the triad of deep unremitting ear pain, ear drainage and Cranial Nerve VI (abducens) paralysis.

Fig. 4.5
Clinical photo of early mastoiditis
The incidence of acute mastoiditis has declined since introduction of the heptavalent pneumococcal conjugate vaccine (PCV7) in 2000 [43, 44]. However, the clinician must guard against a false sense of security regarding the efficacy of intravenous antibiotic therapy alone, without prompt surgical intervention to arrest the infectious process, especially in the presence of intracranial complications [45, 46].
Intratemporal, Intracranial Complications
The overall incidence of intracranial complications has declined dramatically. However, masked symptoms and signs may lead to a false sense of security with delayed therapy or undertreatment. The clinician needs to be keenly aware of circumstances that warrant concern including deep unremitting ear pain, vertigo and only partial response to antibiotic therapy.
Advances in imaging technology have greatly enhanced the ability to make critical, life-saving decisions quickly. Magnetic resonance imaging with vascular flow studies help pinpoint the site and extent of disease.
Meningitis
The incidence of bacterial meningitis has greatly decreased in well-vaccinated populations. Vaccination with PCV 7 and PCV 13 has been instrumental in reduction of pneumococcal meningitis, with reductions in the order of 80–90 %, almost exclusively in vaccine serotypes [47].
Meningitis is a medical emergency, requiring immediate initiation of intravenous, broad-spectrum antibiotics (typically a third generation cephalosporin in combination with vancomycin to cover for resistant pneumococcus). It is a rare complication of otitis media and more typically occurs through hematogenous spread, subsequent to initial invasion of the retropharyngeal tissues by the pathogenic bacteria that are common oral flora. Meningitis can occur secondary to infection in adjacent structures, such as the frontal or mastoid air sinuses, and in that setting the onset may be sudden and catastrophic.
Although the diagnosis can be made clinically it usually requires a lumbar puncture be performed to obtain cerebrospinal fluid (CSF) for analysis, gram stain, and culture. Bacterial meningitis typically has high white cell counts in the CSF (1000’s per microliter) with a neutrophil predominance, low glucose and high protein. Bacteria may or may not be visible on gram stain, but usually grow readily from fluid cultures. Antibiotic therapy should not be delayed for results, and in fact should ideally not be delayed by the attempts to perform the lumbar puncture. If the lumbar puncture cannot be performed quickly, empiric therapy followed by subsequent attempts to obtain CSF for analysis is the standard of care.
The duration of treatment varies by pathogen—from as short as a week for Neisseria meningitides to 3 weeks or more for enteric organisms. Consultation with an infectious disease specialist is recommended.
There is a risk of sensorineural hearing loss secondary to bacterial meningitis, and all patients who have meningitis should have a hearing test performed at the end of therapy.
Epidural Abscess
Acute mastoiditis may lead to an epidural abscess via direct extension of infection through natural dehiscences of bone to either the middle or posterior fossa. The most common site is extension through the tegmen bone separating the mastoid cavity from the middle cranial fossa (Figs. 4.6, 4.7 and 4.8). The presenting symptom is deep seated, throbbing pain from dural traction. Neurosurgical consultation should be obtained. When small, the abscess will usually resolve with mastoidectomy and culture directed intravenous antibiotics. When extensive, the intracranial abscess may require neurosurgical drainage [48].