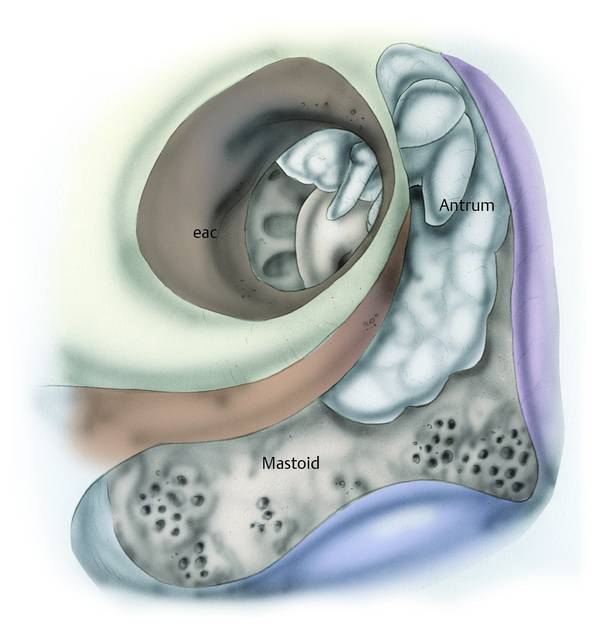
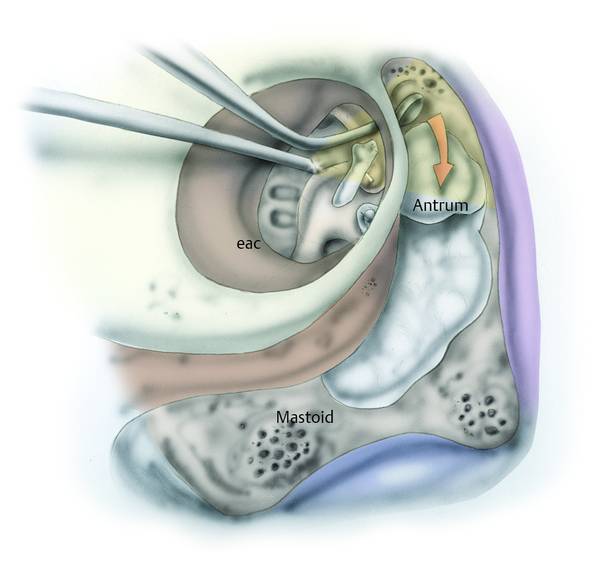
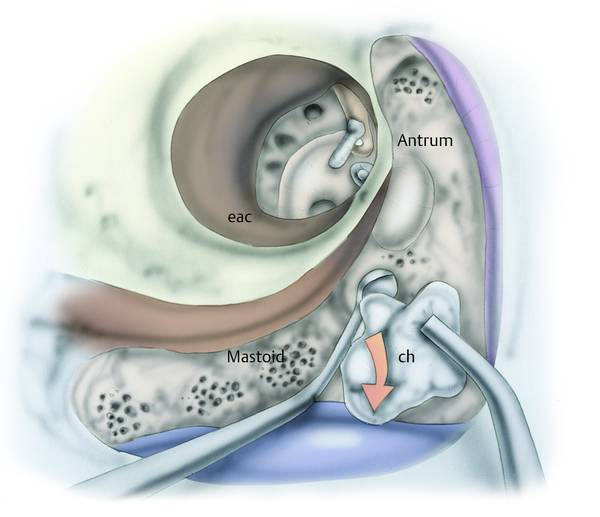
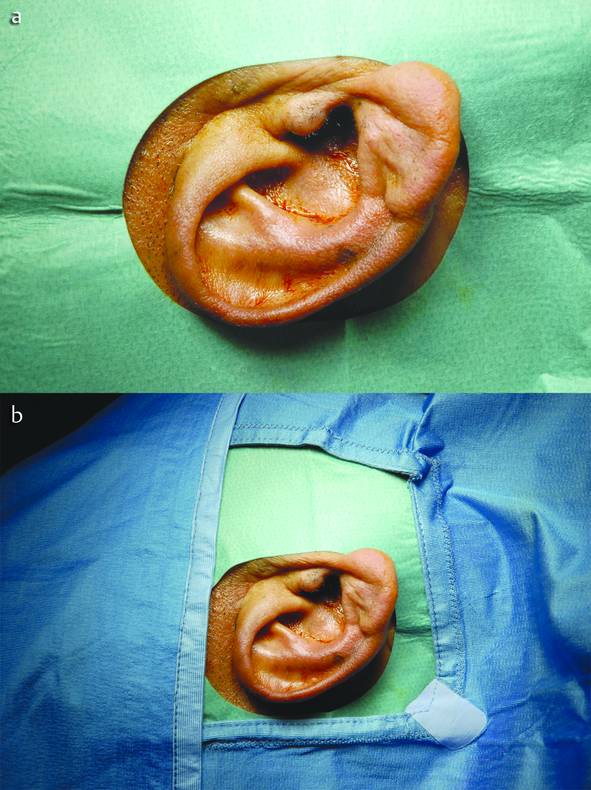
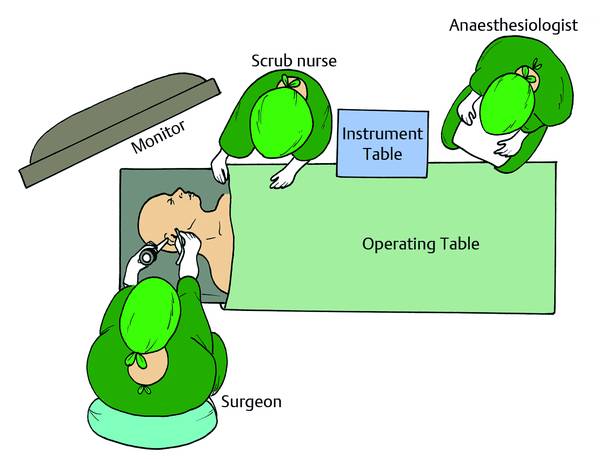
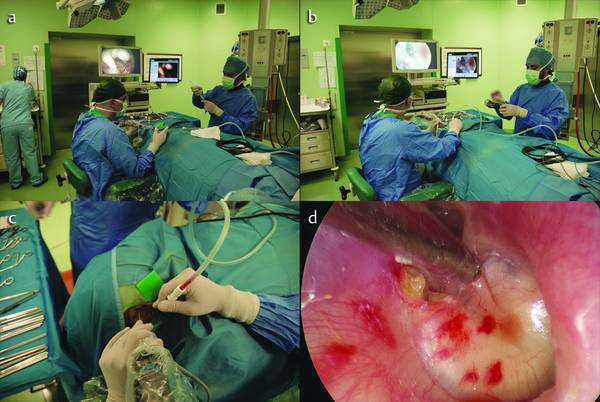
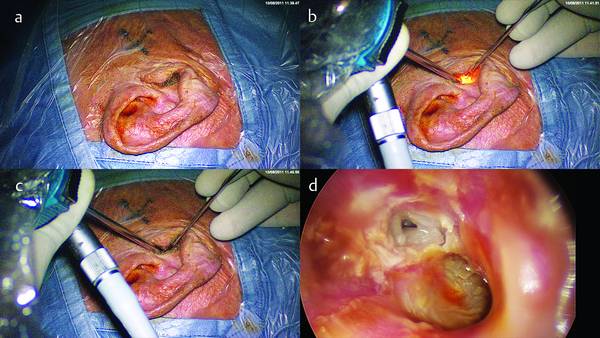
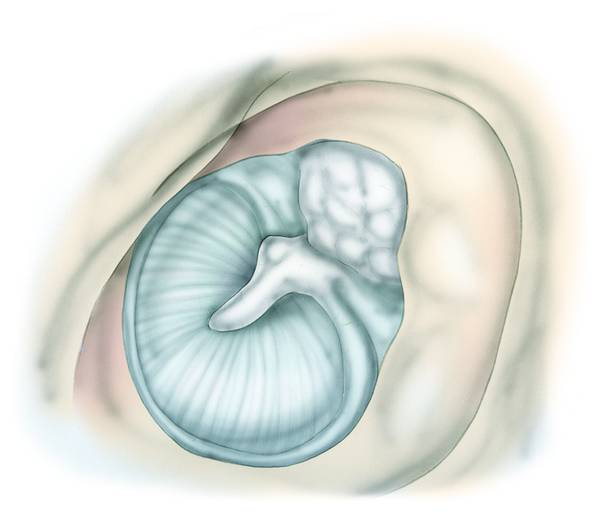
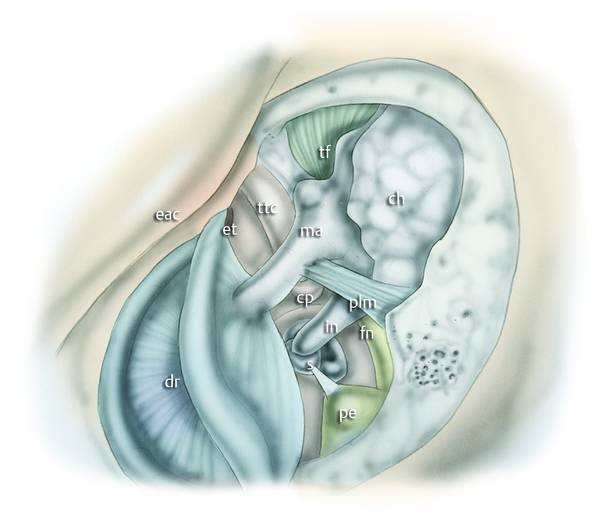
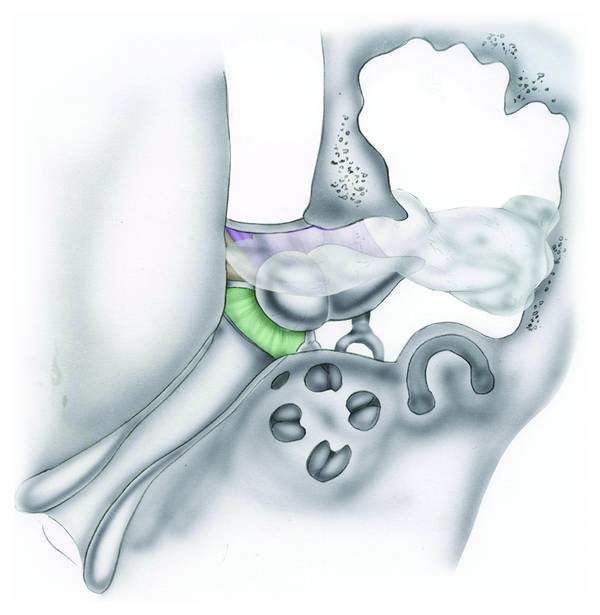
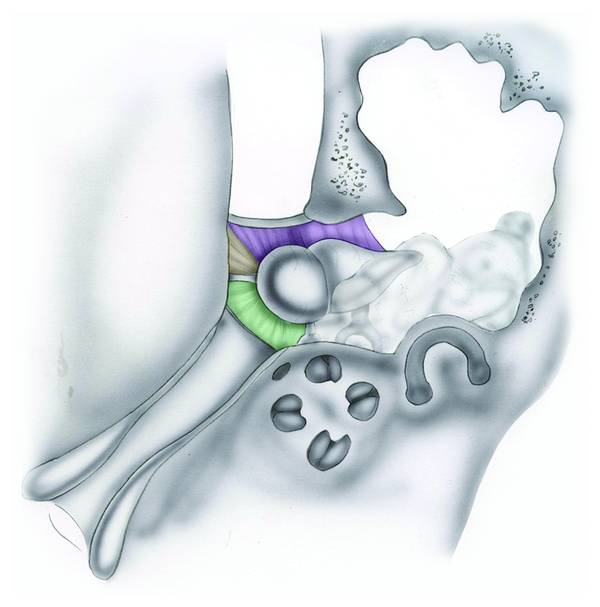
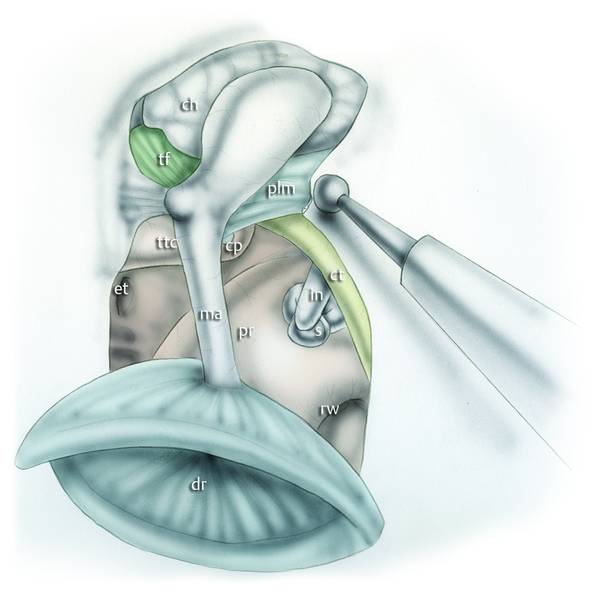
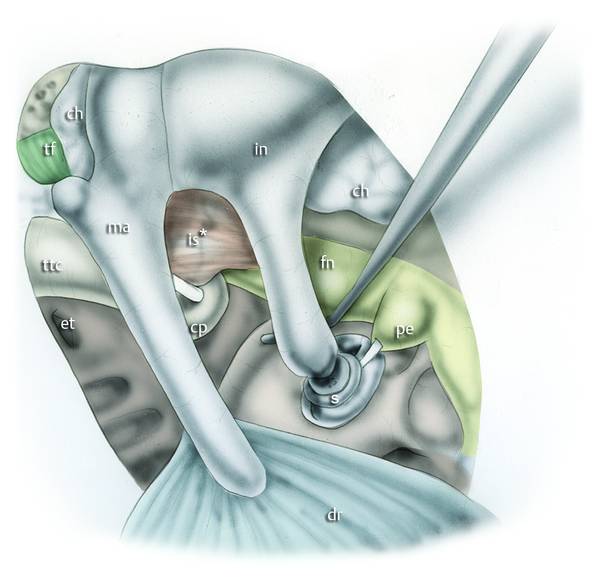
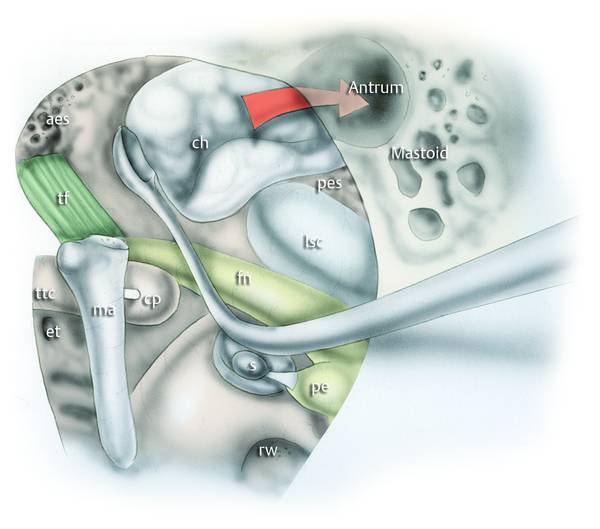
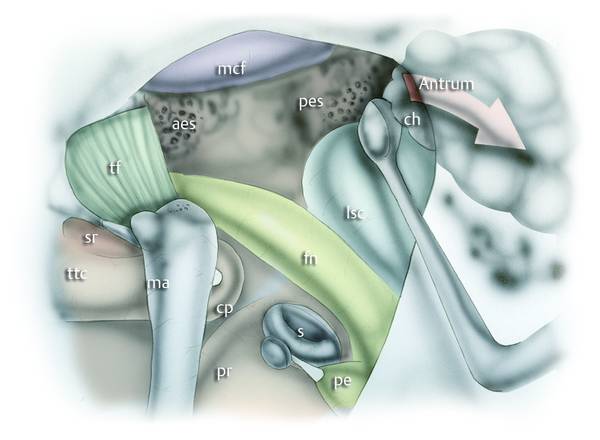
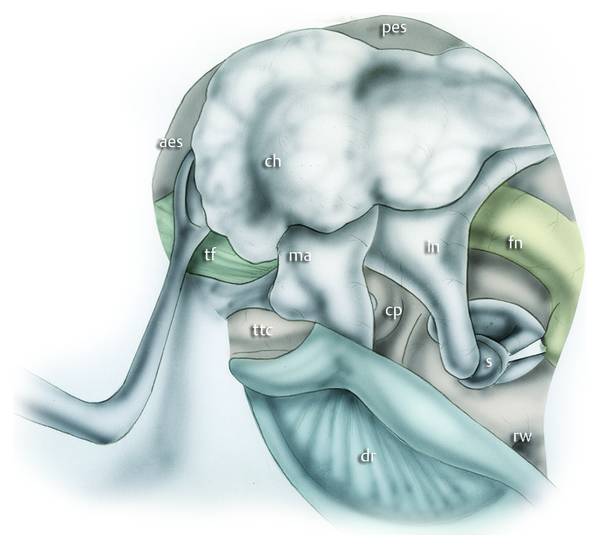
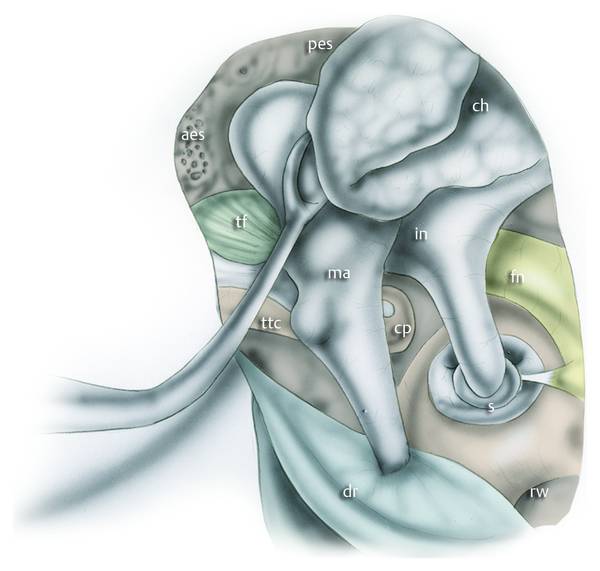
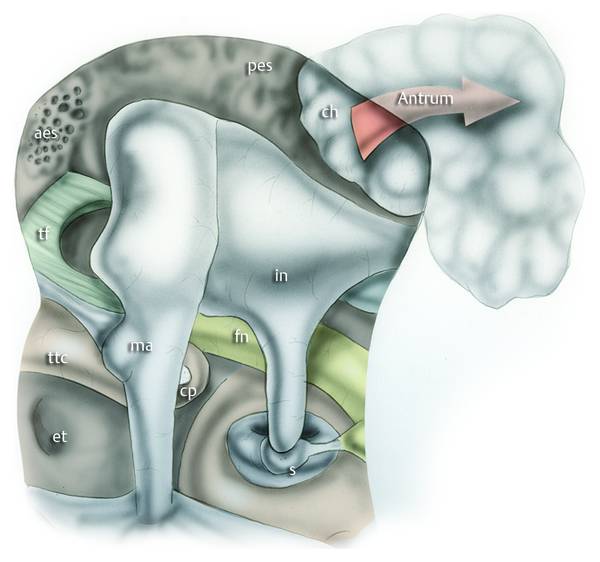
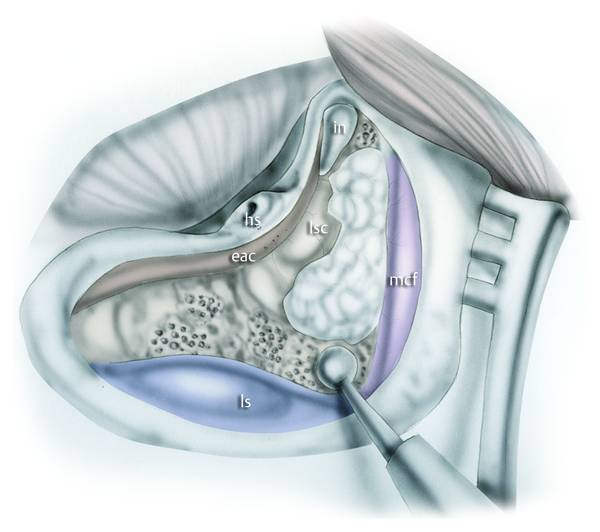
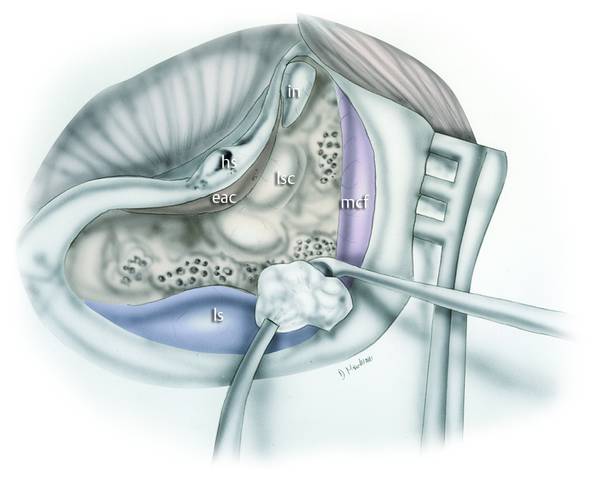
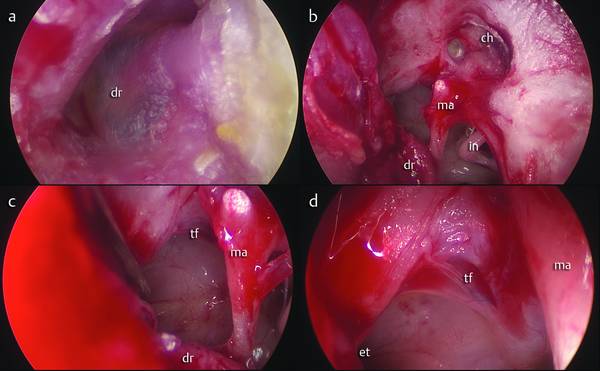
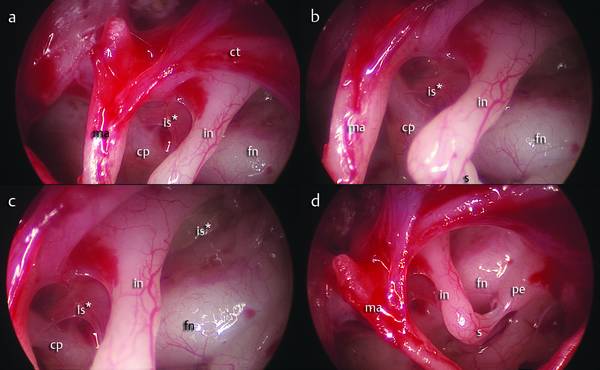
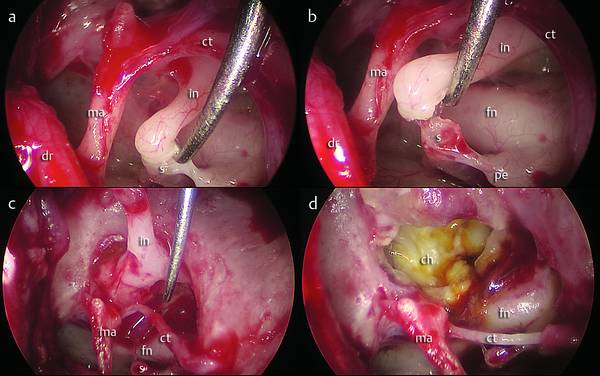
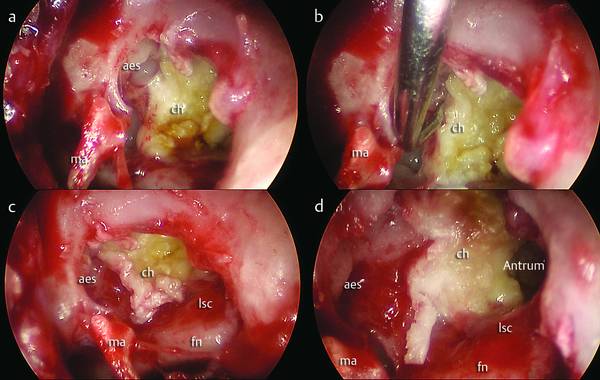
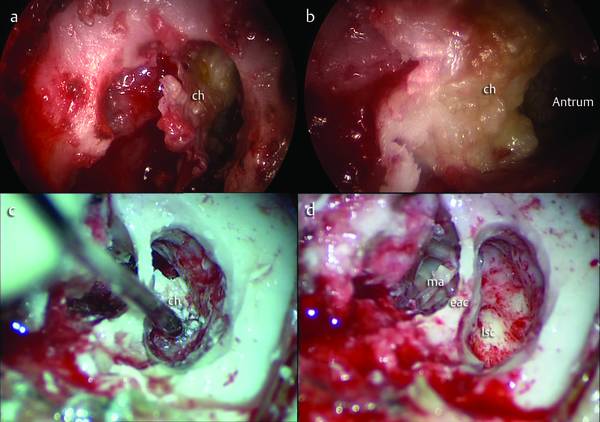
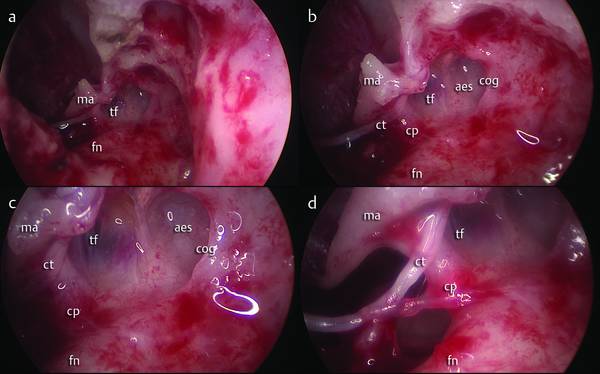
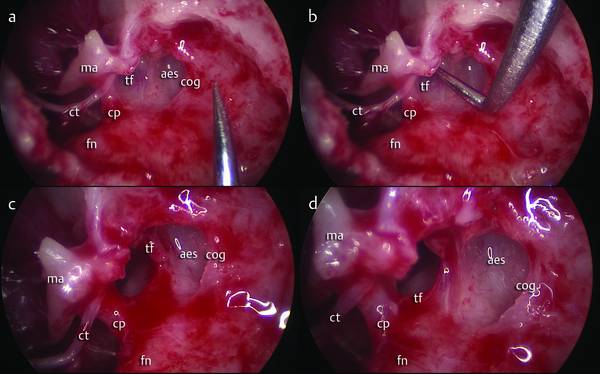
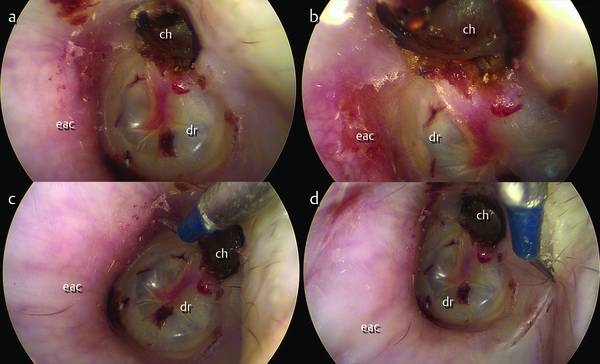
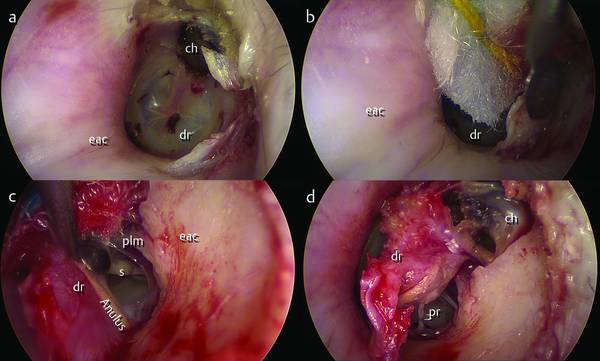
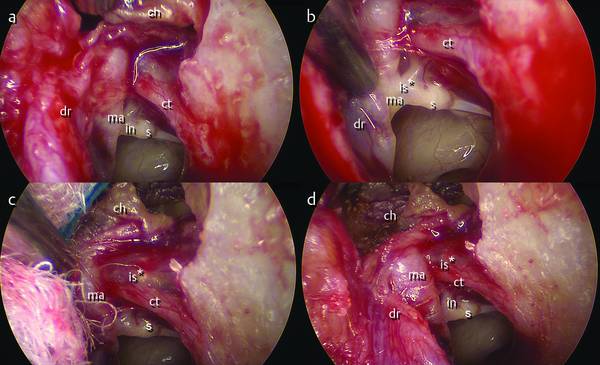
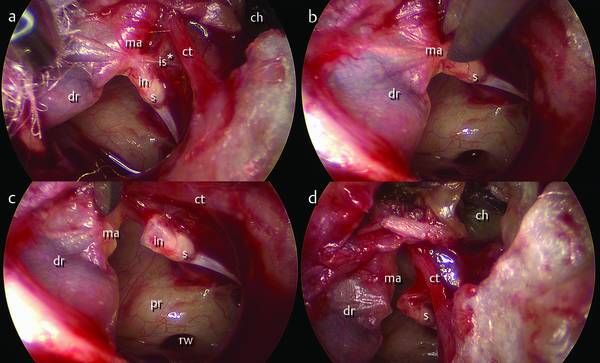
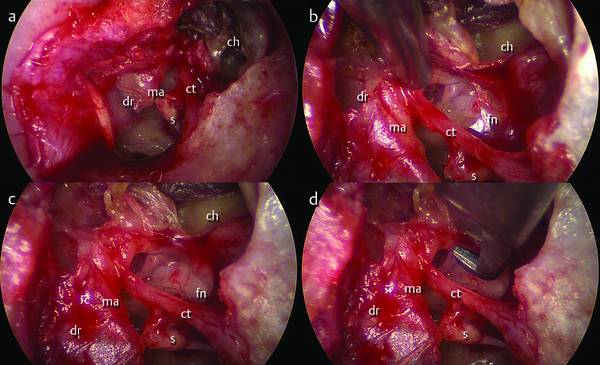
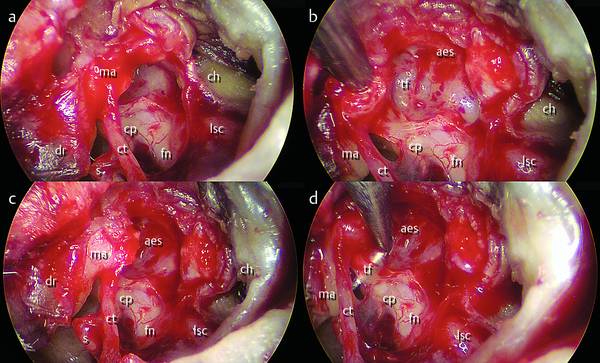
Despite the well-known advantages of endoscopic approaches—e.g., the direct minimally invasive surgical approach to the middle ear preserving the mastoid bone and epitympanic and mastoid mucosa; the direct visualization of the eardrum, ossicular chain, chorda tympani, seventh cranial nerve, and round and oval windows; the wide exposure of the retrotympanic region both medially (sinus tympani, sinus subtympanicus, subpyramidal space) and laterally (facial sinus, lateral sinus)—there are some contraindications to the use of exclusively endoscopic approaches.1–4 For example, if cholesteatoma involves the mastoid cavity, it is not possible to control and remove it by only a transcanal approach; the use of the microscope in combination with the endoscope is recommended. Also, a narrow external ear canal, or external ear malformation, can pose general anatomical difficulties for exclusively endoscopic approaches. The surgical indication for a combined approach should be determined case by case, and in most instances it can even be decided intraoperatively, depending on the true extension of the pathology, in particular the mastoid involvement. Even surgeons with a natural inclination toward the use of the endoscope should never rule out shifting the procedure to a microscopic technique if that is required. The use of combined techniques, compared with the exclusive use of the microscope, will always provide some advantages: mainly that posterior tympanotomy will be required only in exceptional cases, and a possible higher rate of ossicular chain preservation.5–8 This chapter will focus on describing our experiences with the combined use of microscopic and endoscopic techniques. The following two combined approaches should be considered: Endoscopic/microscopic combined approach: Microscopic/endoscopic-assisted approach: With canal wall up technique With canal wall down technique. Attic cholesteatoma (type C2a) with posterior extension to the mastoid, dehiscence of the lateral semicircular canal, dural dehiscence of the mastoid tegmen that needs repair. The combined approach begins with the transcanal endoscopic approach, whose aim is to track and remove the disease from the middle ear, defining the margins anteriorly, superiorly, and inferiorly, and then pushing the cholesteatoma inside the antrum (▶ Fig. 11.1, ▶ Fig. 11.2); the next step is a mastoidectomy with microscopic antrostomy, maintaining the integrity of the posterior wall of the external auditory canal, removing the pathology from the mastoid until it joins with the sac of cholesteatoma previously isolated (▶ Fig. 11.3). Afterward an en bloc resection of cholesteatoma is performed with systematic control of the cavity (by checking the retrotympanum, protympanum, and epitympanum using 0° and 45° optics). Fig. 11.1 Typical indication for the endoscopic combined approach. A cholesteatoma mass deriving from the attic, spreading posteriorly to the mastoid. eac, external auditory canal. Fig. 11.2 The endoscopic step of the combined approach. A transcanal endoscopic approach is used to remove the cholesteatoma sac from the tympanic cavity, pushing the pathological tissue into the antrum. eac, external auditory canal. Fig. 11.3 The microscopic step of the combined approach. A cortical mastoidectomy is performed, reaching the cholesteatoma; when possible the sac is removed en bloc from the mastoid cavity, preserving the antral mucosa whenever possible. eac, external auditory canal; ch, cholesteatoma. At the end of the cholesteatoma removal procedure, transmastoid–antral endoscopic exploration allows an excellent view of the anterior attic and of the upper portion of the tensor fold; endoscopic removal of the tensor fold guarantees direct communication between epitympanum and protympanum. Better control of disease in the tympanic cavity by use of the endoscope and the possibility of maintaining the integrity of the posterior wall of the external auditory canal Easier study and better understanding of the pathophysiological mechanisms underlying the cholesteatoma Preservation of antral and periantral mucosa when possible, so as to maintain proper homeostasis of the middle ear in the postoperative period. The patient is prepared by disinfection of the mastoid region and external ear; the patient’s head is turned slightly contralaterally, with the chin slightly hyperextended (▶ Fig. 11.4). The surgeon sits in front of the patient’s ear (▶ Fig. 11.5). The first step is the transcanal endoscopic approach: the surgeon holds the endoscope with the left hand and the surgical instrument with the right hand; the left armrest of the chair must be raised to allow support of the left elbow in order to keep the endoscope stable during the operation. The surgical instrument is introduced into the external auditory canal and is followed by the endoscope (▶ Fig. 11.6, ▶ Fig. 11.7). Fig. 11.4 a, b The position of the patient’s ear during preparation for surgery. a Close view. b The patient’s head is turned slightly contralaterally. Fig. 11.5 Arrangement of the OR during endoscopic ear surgery. The surgeon, sitting in front of the patient’s ear, holds the endoscope with the left hand and the surgical instrument with the right hand. Fig. 11.6 a, b OR setting during the endoscopic approach. c The endoscope is gently introduced into the external ear, and a suction instrument is used with the right hand to clean the surgical field before starting the surgical approach. d On the high-resolution monitor the surgeon is able to observe her or his performance with the endoscope. Fig. 11.7 Right ear. a The position of the patient’s ear before surgery. b, c The position of the endoscope and the surgical instrument during endoscopic ear surgery. d Endoscopic view of the eardrum in the same patient. All the steps described next are performed with an initial optic of 0° view, 15 cm long, and 3 mm in diameter. The external auditory canal is infiltrated with an epinephrine solution. The injection is administered into the posterior wall of the canal, and then some cottonoids with epinephrine are placed in the external auditory canal and kept in place for about 5 minutes. Using appropriate scalpels and/or with the Vesalius molecular resonance hook, a skin incision is made in the external auditory canal from the 3 o’clock to the 9 o’clock positions up to about 2.5 cm lateral to the anulus (▶ Fig. 11.8). The tympanomeatal flap is lifted gently with the help of epinephrine-soaked cottonoids that are placed between the incision and the bone. The flap is pulled from lateral to medial and from superior to inferior with a specific dissector. The anulus is identified and the dissection of the tympanomeatal flap is performed underlay by lifting the anulus with appropriate hooks. The dissection continues with the dissection superiorly of the pars flaccida, which is carefully detached from the short process of the malleus and pulled inferiorly. The tympanomeatal flap is left adherent to the umbus and is pulled inferiorly to obtain a good exposure of the protympanum (▶ Fig. 11.9). Fig. 11.8 Left ear. Combined approach. The first step is incision of the external auditory canal from the 3 o’clock to the 9 o’clock position up to about 2.5 cm from the anulus; the incision is made with a triangular shape having the apex on the attic. Fig. 11.9 Left ear. Combined approach. The tympanomeatal flap is gently lifted and pulled inferiorly. At the end of the dissection the flap is left adherent to the umbus, giving a good exposure of the tympanic cavity. dr, eardrum; ma, malleus; in, incus; fn, facial nerve; pe, pyramidal eminence; s, stapes; plm, posterior ligament of the malleus; cp, cochleariform process; ttc, tensor; tympani canal; ch, cholesteatoma; et, eustachian tube; tf, tensor fold; eac, external auditory canal. After the creation of the flap, there follows an exploratory phase to investigate the possible presence of an isthmic block and to explore the region of the tensor fold (see Clinical case 1 [▶ Fig. 11.22, ▶ Fig. 11.23] and Clinical case 2 [▶ Fig. 11.30, ▶ Fig. 11.31]). The exploration uses a 45° optic, 15 cm long and 3 mm in diameter, to identify the morphology of the tensor fold and tympanic isthmus. It is also possible to obtain a real-time assessment of the extent of the disease, evaluating the retrotympanic, protympanic, epitympanic, and hypotympanic regions. A further evaluation is made of the ossicular chain (for example, distinguishing the presence of an interruption or disjuncture of the chain) and of the anatomical relationships between the chain and the cholesteatoma. It will be possible to preserve a normally articulated chain if the cholesteatoma extends to the anterior epitympanum and lateral attic without affecting the medial attic and the medial aspect of the incudomalleolar joint (▶ Fig. 11.10); otherwise it will be necessary to remove the chain before the dissection of the cholesteatoma (▶ Fig. 11.11). Drilling of the scutum is carried out to regularize the area usually eroded by the disease and the posterior malleolar ligament is detached (▶ Fig. 11.12); these steps allow further exploration of the chain and medial attic with 45° optics. Fig. 11.10 Attic cholesteatoma with epitympanic lateral extension with respect to the ossicular chain, involving the mastoid antrum. Fig. 11.11 Attic cholesteatoma with epitympanic medial extension with respect to the ossicular chain, involving the mastoid antrum. Fig. 11.12 Left ear. Combined approach. The scutum is partially removed endoscopically with a diamond bur to provide good access to the cholesteatoma sac. dr, eardrum; ma, malleus; in, incus; s, stapes; ct, chorda tympani; plm, posterior ligament of the malleus; cp, cochleariform process; ttc, tensor tympani canal; ch, cholesteatoma; et, eustachian tube; tf, tensor fold; pr, promontory; rw, round window. For the approach to attic cholesteatoma with medial extension to the ossicular chain (▶ Fig. 11.11) an optic with 0° view, 15 cm long, and 3 mm in diameter, is used. When the cholesteatoma extends to the medial aspect of the body of the incus and the head of the malleus, and occupies the entire medial attic, it is necessary to remove the incus and the head of malleus. During the removal, the endoscope must show the lenticular apophysis of the incus and, using a hook, the space between it and the incudostapedial joint must be identified; this maneuver must be particularly gentle. Once the joint is identified, the incus is gently lateralized with a hook, detaching the incudostapedial joint (▶ Fig. 11.13; see also Clinical case 1 [▶ Fig. 11.24, ▶ Fig. 11.25]). After this step it is particularly easy to separate the incudomalleolar joint using a hook and remove the bone with forceps. The removal of the incus allows a wide access to the facial region, exposing the second tract of the facial nerve, which is visualized with the endoscope posteriorly as far as its second genu and anteriorly as far as the geniculate ganglion. The lateral semicircular canal is also visualized, running just above and behind the second genu of the facial nerve and representing an important landmark during surgical dissection of the cholesteatoma from attic to antrum. The neck of the malleus is identified and the head is dissected and removed using forceps (▶ Fig. 11.14); this maneuver allows wide endoscopic access to the entire epitympanum both anteriorly and posteriorly. In this way the cholesteatoma can be controlled endoscopically and, using an angled dissector, it will be possible to dissect the anterior margin of the cholesteatoma from the anterior wall of the anterior epitympanum, pushing the cholesteatoma posteriorly toward the posterior epitympanum and the mastoid antrum (▶ Fig. 11.15; see Clinical case 1 [▶ Fig. 11.26] and Clinical case 2 [▶ Fig. 11.35, ▶ Fig. 11.36]). The anatomical landmarks to consider in the anterior attic are: anteroinferiorly the upper surface of the tensor fold and the tensor tympani canal; anteriorly the anterior wall of the anterior epitympanum; superiorly the dural plane of the middle skull base and the transverse crest (cog), which can present anatomical variations but in most cases originates from the tegmen and drops caudally to the cochleariform process, dividing the anterior and posterior attic. The dissection of the cholesteatoma proceeds from anterior to posterior and from inferior to superior until the cholesteatoma is pushed from the anterior to the posterior attic (▶ Fig. 11.16). Fig. 11.13 Left ear. Combined approach. When the cholesteatoma involves the medial aspect of the ossicular chain it is necessary to remove the incus with a gentle maneuver of the incudostapedial joint endoscopically. dr, eardrum; ma, malleus; in, incus; s, stapes; fn, facial nerve; cp, cochleariform process; ttc, tensor tympani canal; ch, cholesteatoma; et, eustachian tube; tf, tensor fold; is*, isthmus blockage; pe, pyramidal eminence. Fig. 11.14 Left ear. Combined approach. The removal of the head of the malleus allows direct access to the medial epitympanic compartments for removal of the cholesteatoma endoscopically from the attic to the mastoid antrum. dr, eardrum; ma, malleus; s, stapes; fn, facial nerve; cp, cochleariform process; ttc, tensor tympani canal; et, eustachian tube; tf, tensor fold; pe, pyramidal eminence; pr, promontory, rw, round window; lsc, lateral semicircular canal; aes, anterior epitympanic space. Fig. 11.15 Left ear. Combined approach. The cholesteatoma is pushed from the anterior epitympanic space to the posterior epitympanic space (red arrow) with a curved dissector under endoscopic control. The mastoid antrum is located just superiorly and posteriorly with respect to the semicircular lateral canal. ma, malleus; s, stapes; fn, facial nerve; cp, cochleariform process; ttc, tensor tympani canal; et, eustachian tube; tf, tensor fold; pe, pyramidal eminence, rw, round window; lsc, lateral semicircular canal; aes, anterior epitympanic space; pes, posterior epitympanic space; ch, cholesteatoma. Fig. 11.16 Left ear. Combined approach. Under 45° endoscopic view the cholesteatoma is pushed into the mastoid antrum (red arrow) from the posterior epitympanic space. ma, malleus; s, stapes; fn, facial nerve; cp, cochleariform process; ttc, tensor tympani canal; sr, supratubal recess; tf, tensor fold; pe, pyramidal eminence; lsc, lateral semicircular canal; aes, anterior epitympanic space; pes, posterior epitympanic space; ch, cholesteatoma; pr, promontory; mcf, middle cranial fossa. In this phase the anatomical landmarks are the second portion of the facial nerve, which represents the lower limit of posterior epitympanum, and the lateral semicircular canal which runs just above and posterior to the second portion of the facial nerve. Superior and posterior to the lateral semicircular canal there is the mastoid antrum (▶ Fig. 11.16). The cholesteatoma is pushed into the mastoid antrum and then the microscopic steps are carried out. For cholesteatoma with extension to the lateral attic (▶ Fig. 11.10), with or without involvement of the anterior epitympanum, dissection of the cholesteatoma can be considered with the aim of conserving the ossicular chain if the chain is normally articulated. This procedure requires the presence of a large anterior epitympanum, with a wide space between the head of the malleus and the anterior wall of the anterior epitympanum. Preservation of the chain will be particularly difficult in patients with a narrow anterior epitympanum that does not allow surgical maneuvers. The chain preservation maneuver is carried out using angled dissection instruments. The first step is dissection of the cholesteatoma from the anterior wall of the anterior epitympanum; then with gentle manipulation the disease is dissected from the lateral surface of the ossicular chain (the head of the malleus and the body of the incus). The maneuvers are made from anterior to posterior (▶ Fig. 11.17, ▶ Fig. 11.18). Fig. 11.17 Left ear. Combined approach. In cases where the cholesteatoma is lying laterally with respect to the ossicular chain, the dissection of the cholesteatoma is started from the anterior epitympanic space to the posterior epitympanic space. A gentle dissection should be applied to the ossicular chain with a curved dissector to remove the cholesteatoma matrix from the lateral attic, avoiding any damage to the ossicular structures. ma, malleus; s, stapes; in, incus; fn, facial nerve; cp, cochleariform process; ttc, tensor tympani canal; tf, tensor fold; aes, anterior epitympanic space; pes, posterior epitympanic space; ch, cholesteatoma; rw, round window; dr, eardrum. Fig. 11.18 Left ear. Combined approach. The cholesteatoma sac is gently dissected from the malleus and from the body of the incus, pushing it posteriorly. ma, malleus; s, stapes; in, incus; fn, facial nerve; cp, cochleariform process; ttc, tensor tympani canal; tf, tensor fold; aes, anterior epitympanic space; pes, posterior epitympanic space; ch, cholesteatoma; rw, round window; dr, eardrum. Key point: During these steps, and especially for inexperienced surgeons, disjointing the incudostapedial articulation is recommended to avoid luxation of the stapes and fracture of the crura. In some cases it is advisable to drill the posterior wall of the external auditory canal to obtain a good exposure of the short process of the incus. The cholesteatoma is pushed toward the antral region so as to allow the further surgical steps under the microscope (▶ Fig. 11.19). Fig. 11.19 Left ear. Combined approach. The cholesteatoma is pushed into the mastoid antrum from the lateral attic. The short process of the incus is located just inferiorly and anteriorly to the mastoid antrum. ma, malleus; s, stapes; in, incus; fn, facial nerve; cp, cochleariform process; ttc, tensor tympani canal; tf, tensor fold; aes, anterior epitympanic space; pes, posterior epitympanic space; ch, cholesteatoma. Similarly to the traditional mastoidectomy (see Clinical case 2 [▶ Fig. 11.37, ▶ Fig. 11.38]), the surgery begins with a retroauricular skin incision; a temporalis muscle flap is prepared and a temporal fascia is identified, then the mastoid bone is uncovered. The external ear is held with retractors. A cortical mastoidectomy is performed using a bur and the classic landmarks are identified; the middle fossa dura and the sigmoid sinus are skeletonized and the sinodural angle is exposed. The posterior wall of the external auditory canal is skeletonized and preserved. The dissection proceeds until the periantral air cells, the lateral semicircular canal, and the fossa incudis are identified in order to expose the mastoid antrum in which is the cholesteatoma (▶ Fig. 11.20). The cholesteatoma previously dissected is carefully removed, avoiding drilling the antral region and attempting to maintain mucosal integrity (▶ Fig. 11.21). Fig. 11.20 Left ear. Combined approach. Microscopic stage. A cortical mastoidectomy is made to reach the cholesteatoma sac lying in the mastoid antrum. in, incus; hs, spine of Henle; eac, external auditory canal; ls, lateral tympanic sinus; mcf, middle cranial fossa; lsc, lateral semicircular canal. Fig. 11.21 Left ear. Combined approach. The cholesteatoma is removed from the mastoid cavity, maintaining the integrity of the antral mucosa. in, incus; hs, spine of Henle; eac, external auditory canal; ls, lateral tympanic sinus; mcf, middle cranial fossa; lsc, lateral semicircular canal. Once the cholesteatoma has been removed, the mastoid cavity and the entire tympanic cavity are explored using a 45° optic, looking for residual disease, which will be removed if found. Additionally, using a 45° optic with transmastoid access, the superior surface of the tensor fold can be visualized and can be removed with a hook to create good communication between the protympanum and the anterior attic (see Clinical case 1). When necessary, the scutum is reinforced with a cartilage graft from the auricular concha (see Clinical case 2 [▶ Fig. 11.39, ▶ Fig. 11.40]) and a resorbable suture is placed in the retroauricular incision. The reconstructive stage is performed endoscopically through the external canal (see Clinical case 2 [▶ Fig. 11.40]). After these steps the need for ossiculoplasty is evaluated and ossiculoplasty will be performed at the same time or will be programmed for 12 months later, in a second-look procedure (see Clinical case 1 and Clinical case 2). Fig. 11.22 Clinical case 1. Left ear. a Endoscopic view of the eardrum before surgery. b The tympanomeatal flap is elevated and transposed inferiorly; the cholesteatoma sac extending into the epitympanum is visible endoscopically. Despite the presence of pathological attical tissues, the mesotympanic mucosa is well aerated. c With a 0° endoscope we are able to see the inferior edge of the tensor fold located anteriorly with respect to the malleus handle. d Endoscopic magnification of the tensor fold; in this case the tensor fold is complete, separating the protympanum from the anterior epitympanic space. ma, malleus; in, incus; tf, tensor fold; ch, cholesteatoma; et, eustachian tube; dr, eardrum. Fig. 11.23 Clinical case 1. Left ear. a, b A 45° endoscopic exploration of the isthmus is undertaken; an isthmus blockage is endoscopically evident due to a mucosal fold attaching between the cochleariform process and the incus. c, d Another fold is blocking the posterior isthmus. A selective dysventilation syndrome is postulated in this patient. ma, malleus; in, incus; cp, cochleariform process; is*, isthmus blockage; ct, chorda tympani; fn, facial nerve; pe, pyramidal eminence. Fig. 11.24 Clinical case 1. Left ear. a, b In this case the medial extension of the cholesteatoma requires removal of the incus in order to enable the dissection of the cholesteatoma from the medial attic. The articulation between the stapes and the incus is gently detached endoscopically. c The incus and the head of the malleus are removed. d The cholesteatoma sac is endoscopically exposed in the medial attic. ma, malleus; in, incus; s, stapes; ct, chorda tympani; fn, facial nerve; pe, pyramidal eminence; ch, cholesteatoma; dr, eardrum. Fig. 11.25 Clinical case 1. Left ear. a, b The endoscopic dissection of the sac is begun from the anterior epitympanic space to the posterior epitympanic space with a curved dissector. c During the dissection, wherever possible the surgeon should pay attention to maintaining the integrity of the cholesteatoma sac, observing the anterior limit of the cholesteatoma. d A 45° endoscope is used to identify where the mastoid antrum is located. ma, malleus; fn, facial nerve; ch, cholesteatoma; aes, anterior epitympanic space; lsc, lateral semicircular canal. Fig. 11.26 Clinical case 1. Left ear. a, b The cholesteatoma is gently pushed into the antrum endoscopically. c, d A cortical mastoidectomy is performed in order to remove the cholesteatoma from the mastoid cavity. ma, malleus; ch, cholesteatoma; lsc, lateral semicircular canal; eac, external auditory canal. Fig. 11.27 Clinical case 1. Left ear. a–d A 45° endoscope is used through the mastoid to expose the anterior epitympanic space; the relationships between the superior edge of the tensor fold, the cochleariform process, and the cog are visible endoscopically. c In this case a horizontal orientation of the complete tensor fold is evident; the cog is like a bony crest separating the anterior epitympanic space from the posterior epitympanic space. d The chorda tympani runs laterally with respect to the tensor fold, maintaining a close relationship with this fold. ma, malleus; aes, anterior epitympanic space; fn, facial nerve; tf, tensor fold; ct, chorda tympani; cp, cochleariform process. Fig. 11.28 Clinical case 1. Left ear. Before the reconstruction stage, using a curved instrument through the mastoid the surgeon is able to remove the tensor fold endoscopically, creating a direct connection between the protympanum and the anterior epitympanic space (a–d). ma, malleus; aes, anterior epitympanic space; fn, facial nerve; tf, tensor fold; ct, chorda tympani; cp, cochleariform process. Fig. 11.29 Clinical case 2. Left ear. a, b Endoscopic magnification before surgery in a patient with attic cholesteatoma. c, d An incision of the external ear canal is made with a Vesalius dissector. dr, eardrum; eac, external auditory canal; ch, cholesteatoma. Fig. 11.30 Clinical case 2. Left ear. a, b The tympanomeatal flap is elevated with an appropriate dissector, until the anulus is endoscopically visible. c The anulus is elevated with the flap, entering into the tympanic cavity. d During the dissection of the pars flaccida, the cholesteatoma sac is gently separated from the eardrum; the flap is transposed inferiorly. dr, eardrum; eac, external auditory canal; ch, cholesteatoma; plm, posterior ligamental fold of the malleus; pr, promontory; s, stapes. Fig. 11.31 Clinical case 2. Left ear. a–c The dissection of the flap is continued, pulling the eardrum anteriorly and inferiorly. b The handle of the malleus and the incudostapedial joint are evaluated endoscopically. In this case the isthmus is also evaluated endoscopically: the isthmus is blocked by a mucosal fold involving the chorda tympani, the incudostapedial joint, and the malleus. d The handle of the malleus is medialized on the stapes. dr, eardrum; ch, cholesteatoma; ct, chorda tympani; ma, malleus; s, stapes; in, incus; is*, isthmus blockage. Fig. 11.32 Clinical case 2. Left ear. a The handle of the malleus is adherent to the stapes, the anterior isthmus is blocked, and the long process of the incus is eroded. b, c The mucosal fold between the stapes and the malleus is removed with microscissors. d The mucosal fold has a horizontal orientation separating the attic, where the cholesteatoma is located, from the mesotympanic spaces (where a well-ventilated mucosa is noted). dr, eardrum; ch, cholesteatoma; ct, chorda tympani; ma, malleus; s, stapes; in, incus; pr, promontory; rw, round window; is*, isthmus blockage. Fig. 11.33 Clinical case 2. Left ear. a, b The mucosal fold is gently removed with a suction instrument in order to reveal the tympanic facial nerve; the body of the incus is absent. c, d The dissection continues with the removal of the head of the malleus. dr, eardrum; ch, cholesteatoma; ct, chorda tympani; ma, malleus; s, stapes; fn, facial nerve. Fig. 11.34 Clinical case 2. Left ear. a, b Removal of the head of the malleus allows direct access to the anterior epitympanic space, exposing the superior edge of the tensor fold. The dissection of the cholesteatoma continues, removing the sac from the anterior epitympanum. c, d
When surgery is begun as a transcanal endoscopic approach to the tympanic cavity to remove the pathology from the tympanic cavity to the mastoid antrum, and continues with a microscopic mastoidectomy in order to reach and remove the pathology in the antrum and mastoid cells.
When classical microscopic surgery is performed (with canal wall up or canal wall down technique) and after the microscopic surgery, the endoscope is introduced into the cavity in order to find and remove residual disease.
11.2 Endoscopic/Microscopic Combined Approach
11.2.1 Indications
11.2.2 Advantages
11.2.3 Endoscopic Surgical Steps
Approach to Attic Cholesteatoma with Medial Extension to the Ossicular Chain

Approach to Attic Cholesteatoma with Lateral Extension to the Ossicular Chain
11.2.4 Microscopic Surgical Steps
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine
