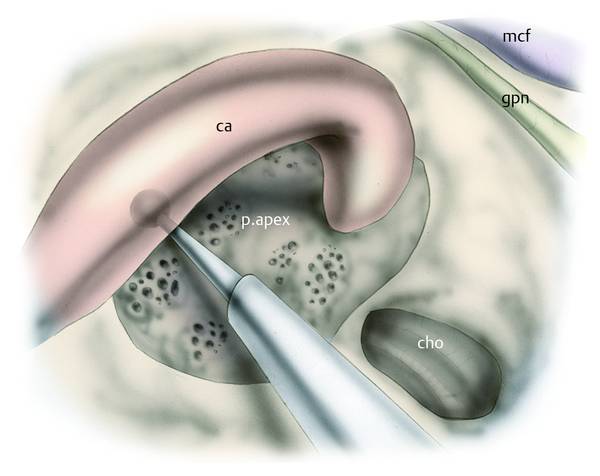
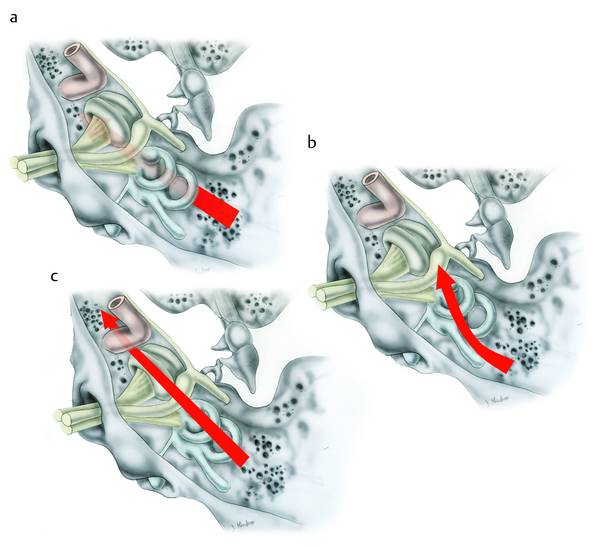
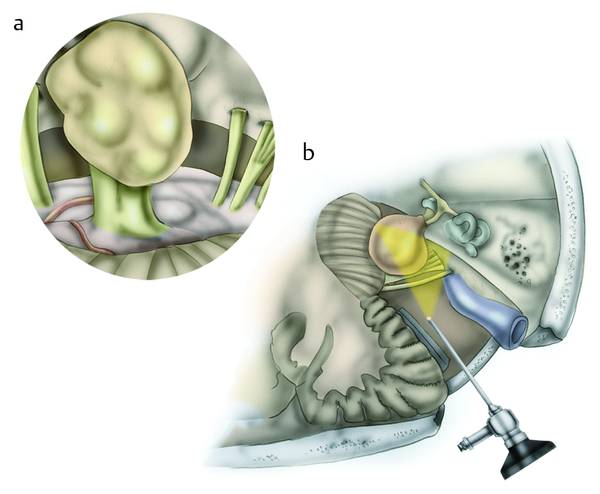
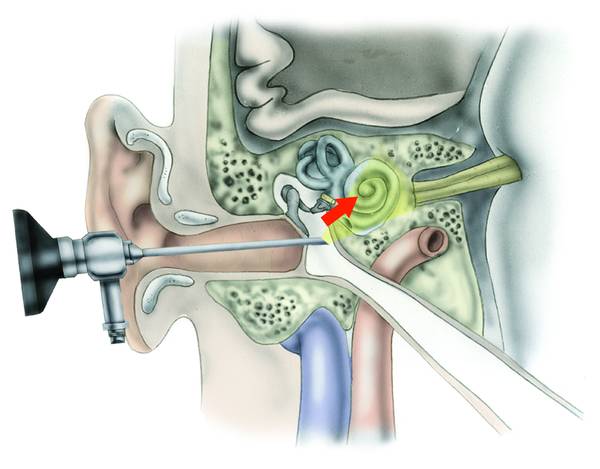
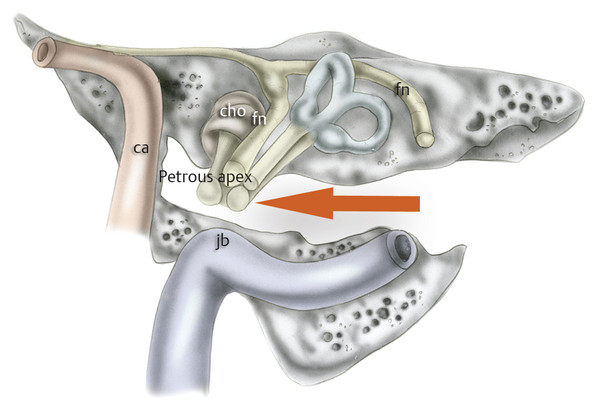
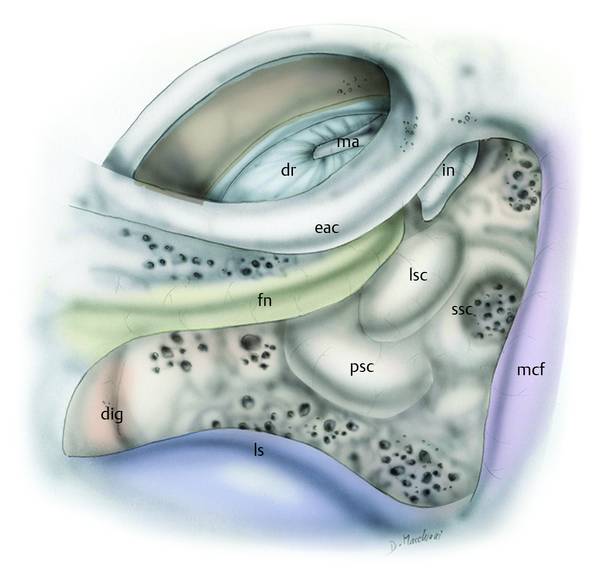
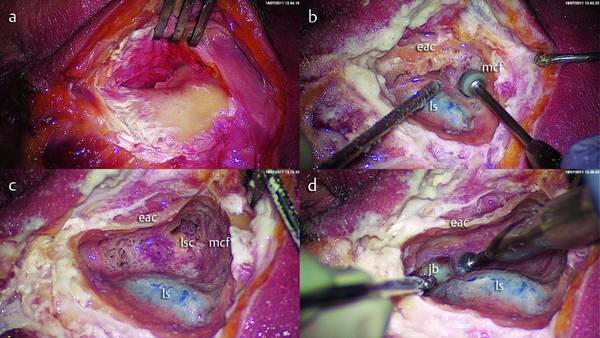
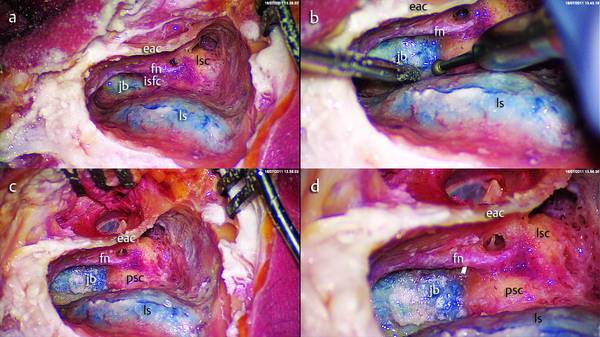
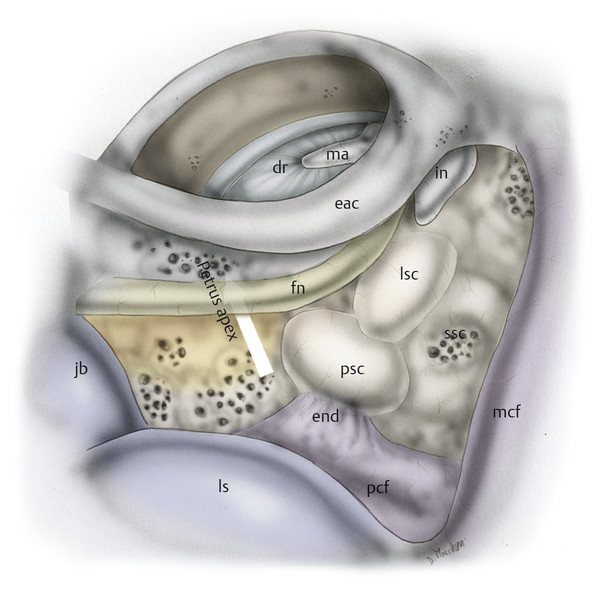
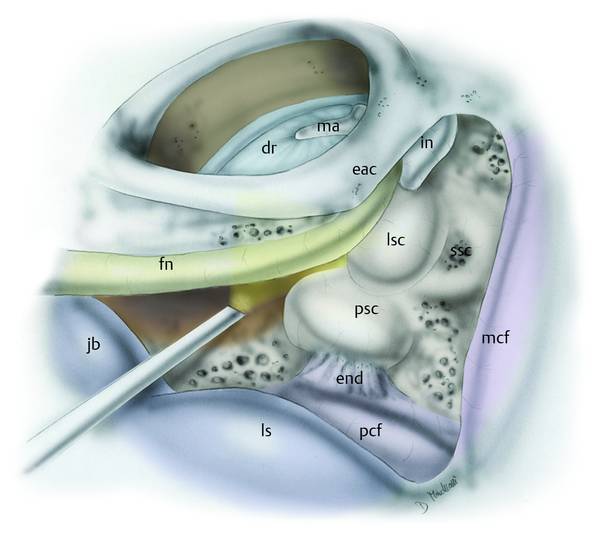
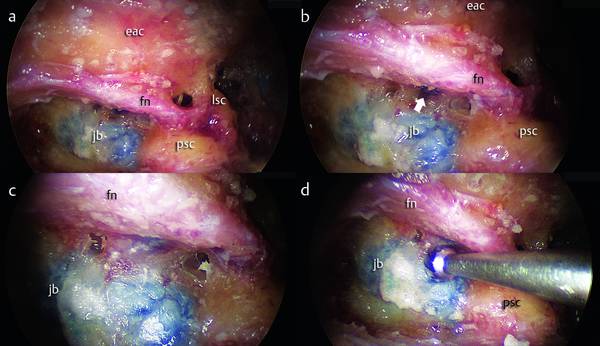
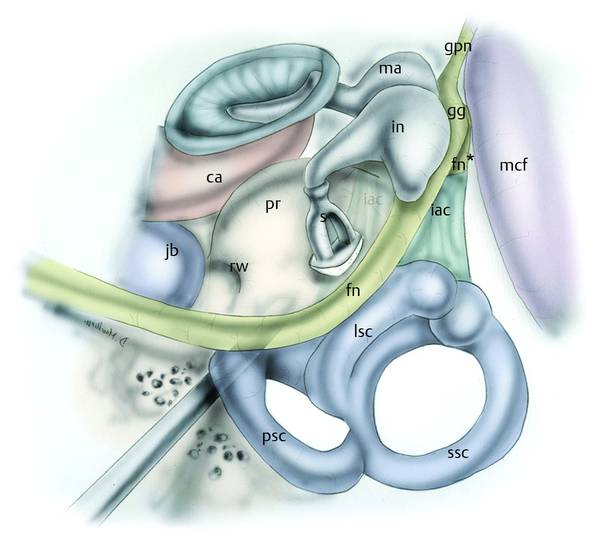
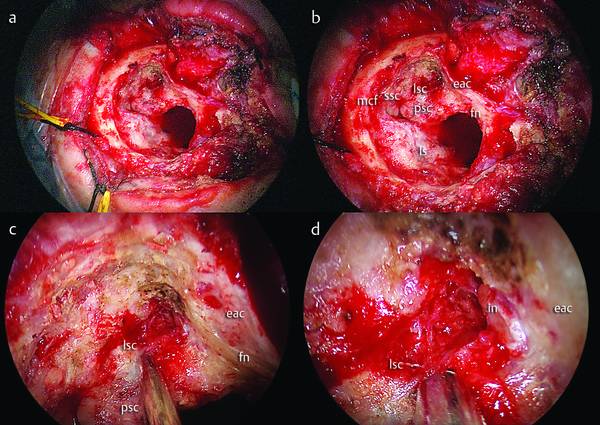
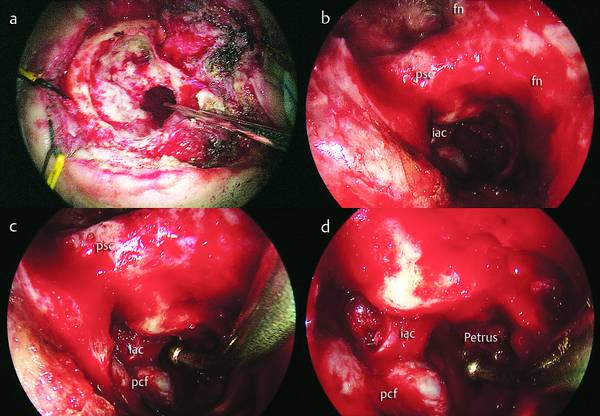
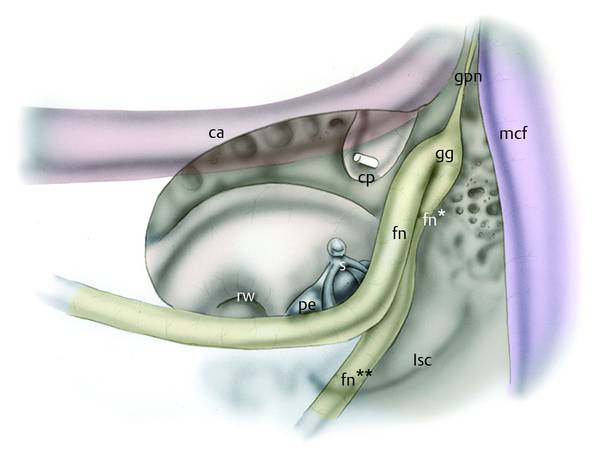
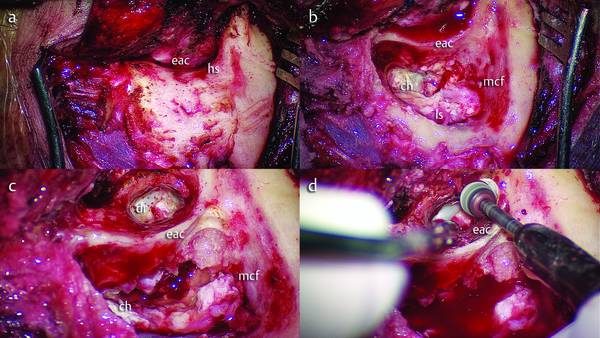
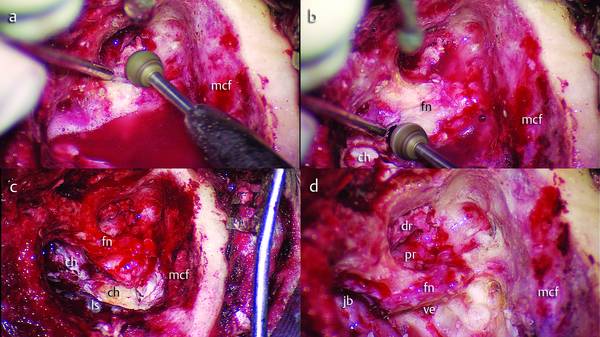
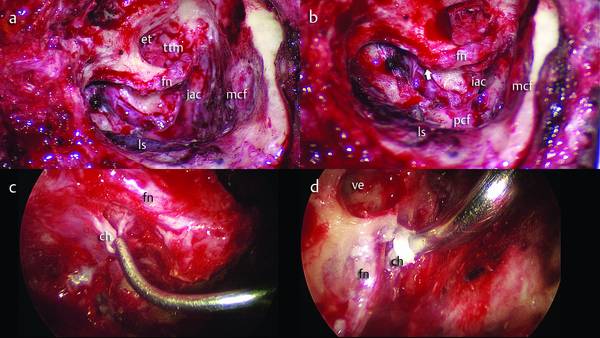
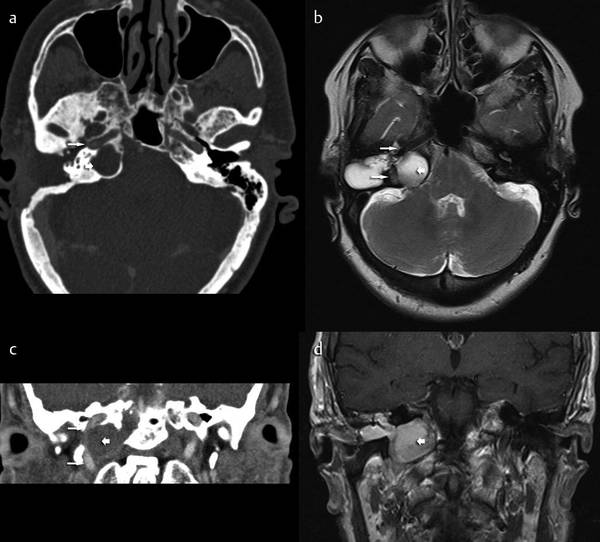
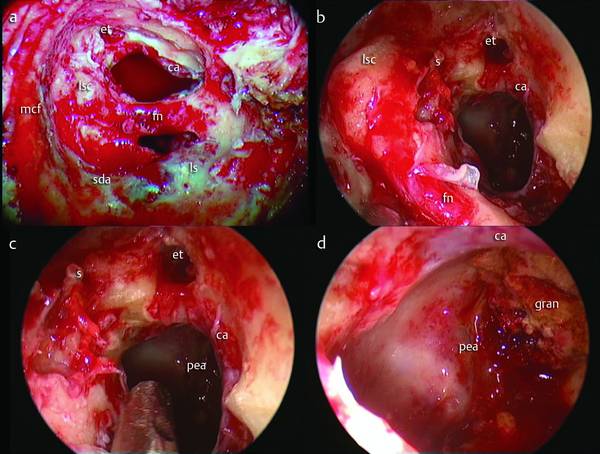
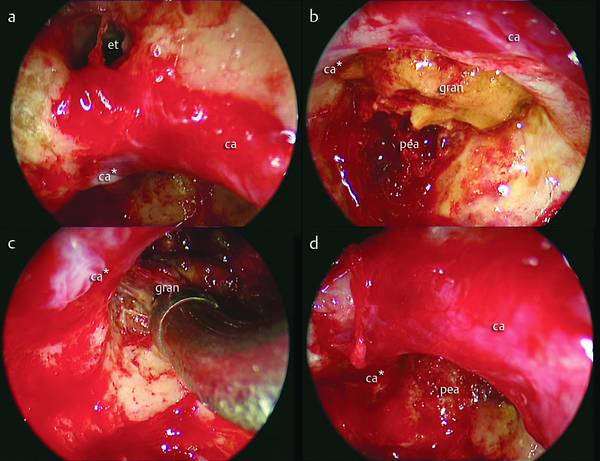
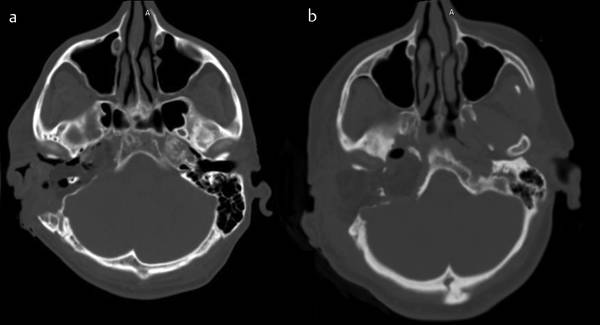
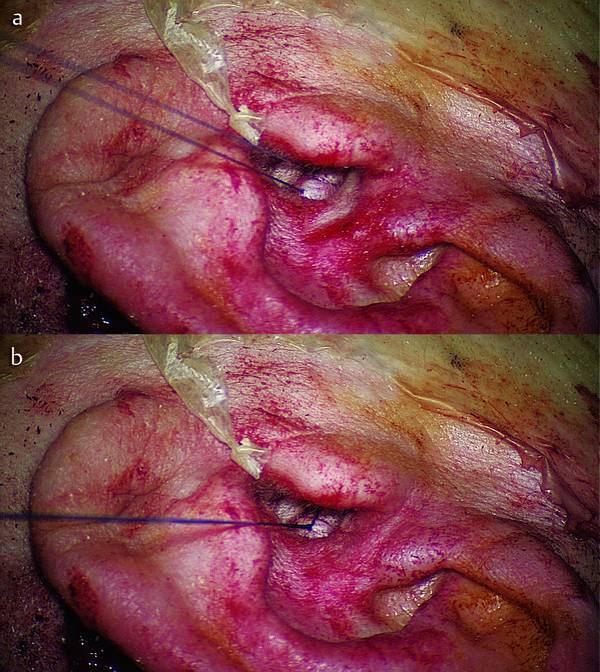
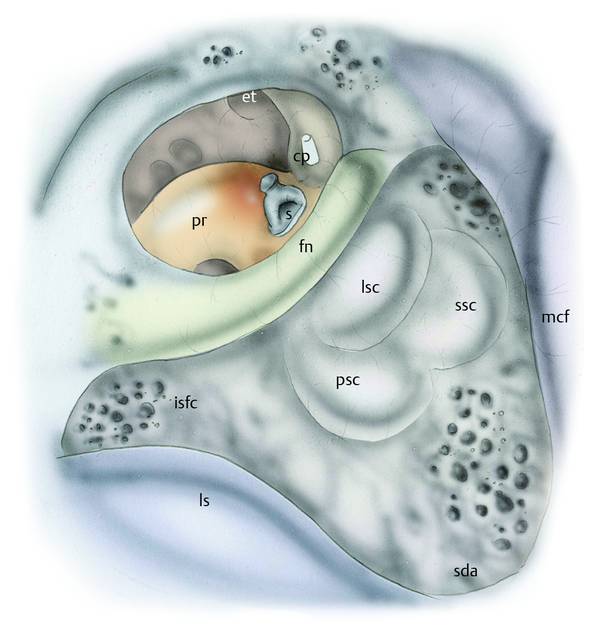
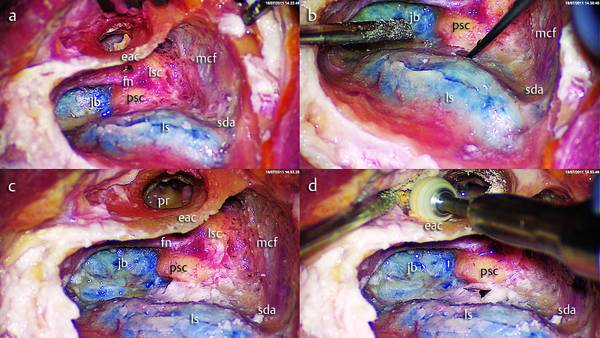
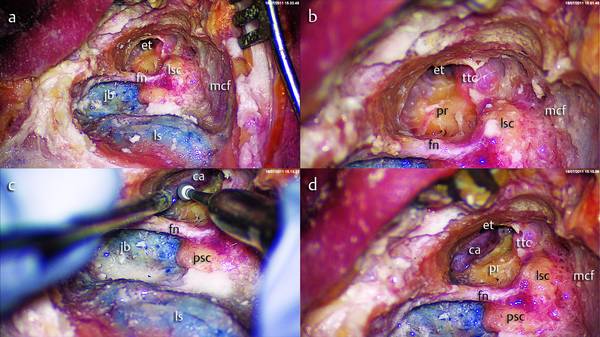
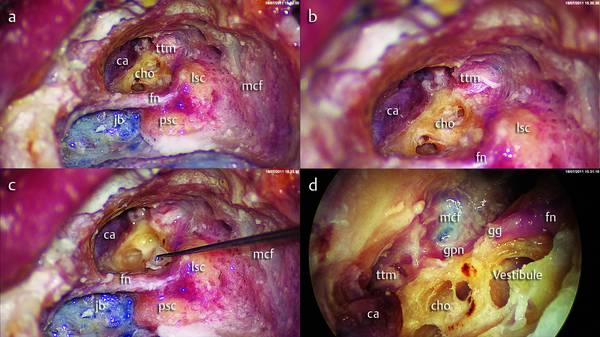
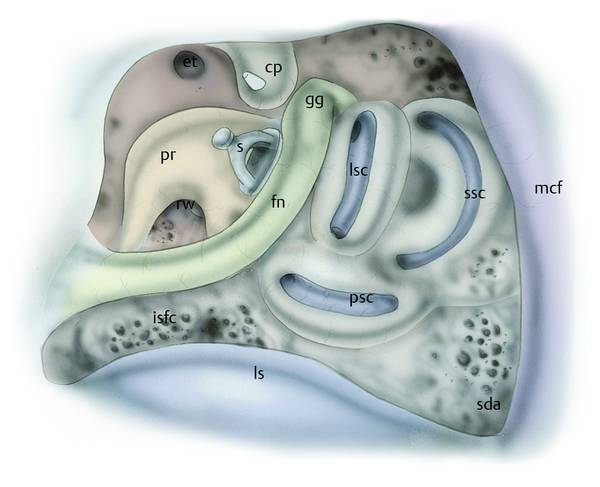
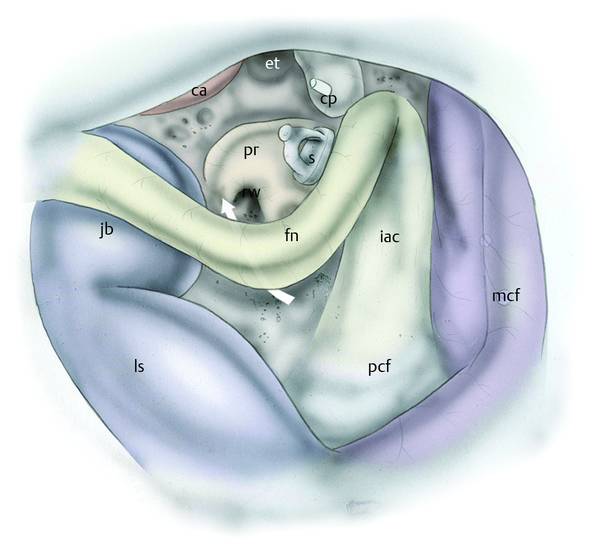
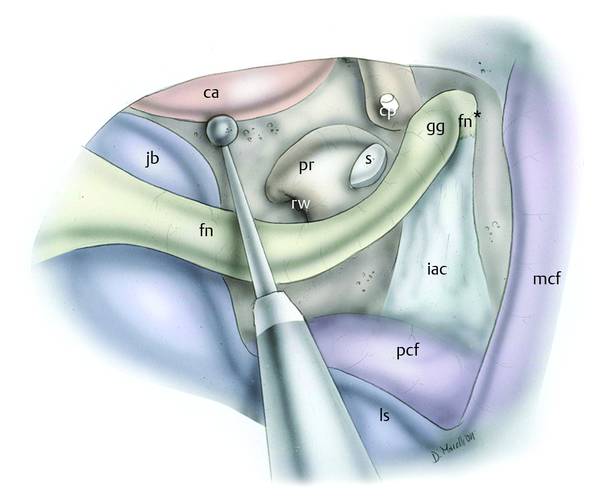
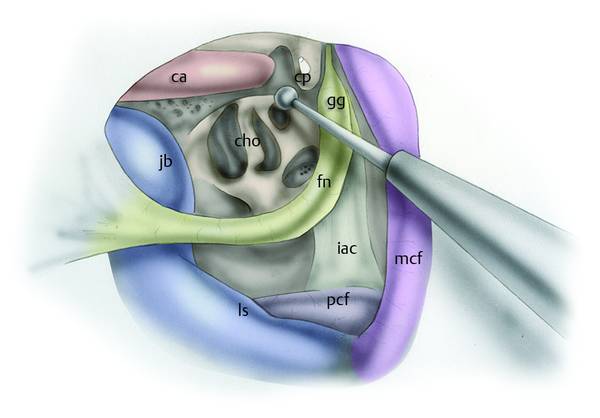
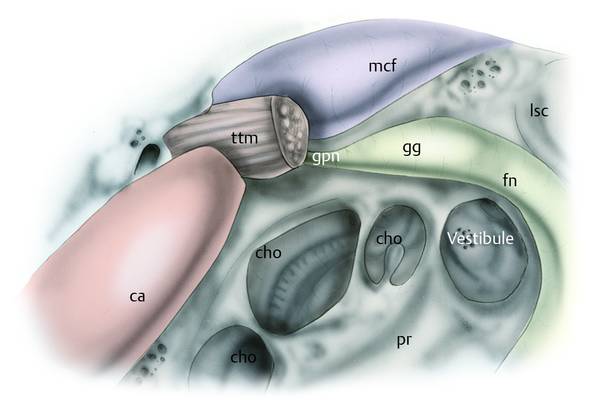
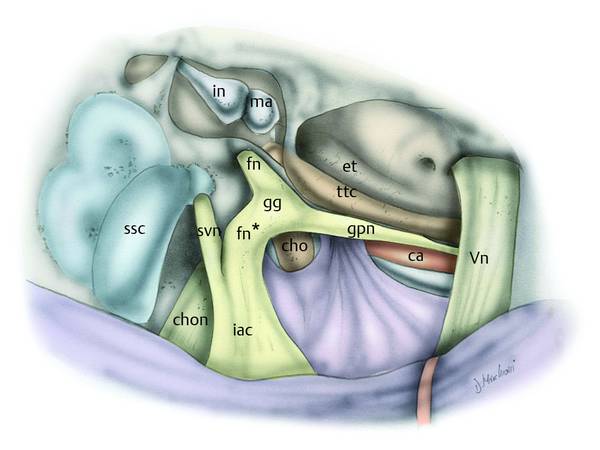
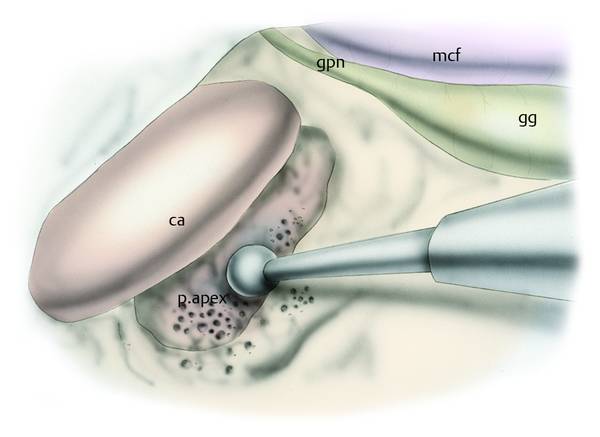
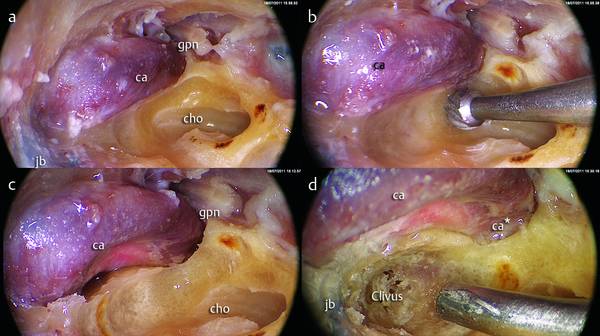
Combined Approaches to Petrous Apex and Inner Ear Diseases The introduction of endoscopes into microsurgical approaches for the inner ear was particularly useful, and in three anatomical regions this tool can be used side by side with the microscope: the petrous apex, the internal auditory canal (IAC), and the posterior cranial fossa (PCF). According to the use of the endoscope during inner ear surgery we can classify two different endoscopic surgical approaches (type A and type B) in treating inner ear disease. Type A Endoscopically assisted approach (combined microscopic/endoscopic), which provides two surgical routes: Transmastoid route Infralabyrinthine endoscopically assisted route (▶ Fig. 19.1a) Suprameatal translabyrinthine endoscopically assisted route (▶ Fig. 19.1b) Transotic endoscopically assisted route (▶ Fig. 19.1c) Retrosigmoid route (▶ Fig. 19.2). Fig. 19.1 Drawing in axial view representing the transmastoid route: infralabyrinthine approach (a); suprameatal translabyrinthine approach (b); transotic approach (c). Fig. 19.2 Right ear. a Drawing of the endoscopic appearance of the cerebellopontine angle: acoustic neuroma is endoscopically detectable. b Drawing representing the retrosigmoid endoscopically assisted route for the posterior fossa. Type B Transcanal, transcochlear/vestibular exclusively endoscopic approach (see Chapter ▶ 18) (▶ Fig. 19.3). Fig. 19.3 Right ear. Drawing representing the transcanal, transcochlear/transvestibular endoscopic approach to the inner ear (red arrow). This chapter will consider the endoscopically assisted approaches. Selection of the surgical route depends on the anatomical region involved by the disease and on the characteristics of the pathological tissue. Before the description of surgical techniques, some brief considerations regarding the two different surgical routes are necessary. The transmastoid route allows an approach to disease lying in the inner ear, petrous apex, and IAC. Exclusively microscopic surgery of the petrous apex did not spare the postoperative complications of many patients who underwent these approaches. We know that in this region there are several anatomical structures that should be preserved: Seventh cranial nerve Middle cranial fossa (MCF) dura Posterior cranial fossa (PCF) dura Internal carotid artery Internal jugular vein bulb Labyrinth Internal auditory canal (IAC). Several surgical approaches previously proposed are based on the anterior rerouting of the seventh cranial nerve (infratemporal approaches) or the posterior rerouting of the facial nerve (transcochlear approaches). Attempts to develop approaches that do not involve displacement of the seventh cranial nerve (such as the transotic approach) have very limited indications due to the narrowness of the surgical field. In many cases endoscopic surgery can be integrated into microscopic surgery for some surgical steps in order to explore and operate “around the corner” without displacing the structures that stand between the surgeon and the pathology; moreover, less bone drilling, along with a magnified view of the anatomy, leads to less-invasive surgery and consequently to a shorter and more comfortable postoperative stay in hospital. The retrosigmoid route is considered the classical neurosurgical approach to the posterior cranial fossa (PCF). Commonly the microscopic retrosigmoid approach allows resection of most of the pathologies in the posterior fossa and particularly when the disease is located in the cerebellopontine angle (CPA). The pathological entity most frequently observed is the acoustic neuroma or schwannoma, but those encountered also include meningiomas, glomus tumors, schwannomas of the mixed nerves, epidermoid cysts, ependymomas, neurovascular conflicts, CSF fistulas, and vascular lesions. The exclusively microscopic approach presents some disadvantages such as poor control of the prepontine cistern and the ventral surface of the brainstem, the impossibility of controlling the Meckel cave, and poor control of the fundus of the internal auditory canal. First, during this approach a cerebellum retractor is used in order to obtain better exposure of the ventral surface of the brainstem: retraction of the cerebellum may lead to edema or to damage of this important organ. Secondly, if a tumor is located in the internal auditory canal and reaches the fundus, extensive drilling of the porus and of the lateral wall of the internal auditory canal is required to remove the disease. Even with this, microscopic control of the fundus is limited and the removal of tumor from this anatomical area has to be performed by blind maneuvering. In these circumstances, the surgeon might inadvertently leave residual tumor, with eventual recurrence. The introduction of endoscopically assisted surgery into the retrosigmoid approach resolves these important limitations of the technique, permitting good exposure of the ventral surface of the brainstem and of the fundus of the IAC without extensive drilling of the porus. As previously indicated, selection of the surgical route will depend on the position and characteristics of the pathology; there can be distinguished an endoscopically assisted transmastoid route—indicated for removal of lesions of the petrous apex and fundus of the IAC—and an endoscopically assisted retrosigmoid approach for the removal of lesions of the posterior cranial fossa and CPA. Three endoscopically assisted transmastoid surgical routes can be distinguished; the route will be selected according to the characteristics of the pathological tissue to be remove and the site involved: Infralabyrinthine endoscopically assisted route Transotic endoscopically assisted route Suprameatal translabyrinthine endoscopically assisted route. This approach is indicated for lesions involving the temporal bone with inferior extension (beneath the labyrinth), in patients with normal hearing function. This approach allows tumor resection without sacrifice of auditory function (▶ Fig. 19.4). Fig. 19.4 Infralabyrinthine route (orange arrow), right ear from behind. The labyrinth and the cochlea are preserved. The mastoid air cells located inferiorly to the bony labyrinth are removed in order to reach the petrous apex, preserving hearing function. ca, carotid artery; jb, jugular bulb; cho, cochlea; fn, facial nerve. A high jugular bulb extending cranially to the labyrinthine block contraindicates this procedure, since it makes subfacial tympanotomy extremely dangerous and the space is inadequate for endoscopic surgery. Furthermore, removal of lesions that infiltrate the dura layer and require dural resection is not feasible with this technique. Two different steps can be distinguished: the first is the microscopic step, preparing the transmastoid route and reaching the disease; then follows the endoscopic step to remove the lesion. The surgeon performs a classical microscopic mastoidectomy, highlighting the common anatomical landmarks (▶ Fig. 19.5, ▶ Fig. 19.6): the dura of the middle cranial fossa superiorly, and the posterior sigmoid sinus inferiorly, which is exposed up to identification of the jugular bulb. If required, a mastoid antrostomy is performed to identify the labyrinth and the incus, preserving the integrity of the ossicular chain. The sigmoid sinus is decompressed and bone removal is continued posterior to the sigmoid sinus to allow further decompression of this vessel. Inferiorly and anteriorly to the sigmoid sinus, the jugular bulb is identified and exposed (▶ Fig. 19.6). Fig. 19.5 Infralabyrinthine approach. Left ear. A traditional microscopic mastoidectomy is performed; the common anatomical landmarks are exposed during drilling. ls, sigmoid sinus (lateral sinus); eac, external auditory canal; psc, posterior semicircular canal; lsc, lateral semicircular canal; ssc, superior semicircular canal; mcf, middle cranial fossa; fn, facial nerve; dr, eardrum; ma, malleus; in, incus; dig, digastric ridge. Fig. 19.6 Infralabyrinthine approach. Microscopic dissection. Left ear. a After incision of the skin, the mastoid bone is exposed and the spine of Henle and the posterior bony wall of the external auditory canal are identified. b, c A traditional mastoidectomy is performed, preserving the posterior bony wall of the external auditory canal, and reaching the antrum and the bony labyrinth. d The sigmoid sinus is widely exposed and following this vascular structure the jugular bulb is also identified. eac, external auditory canal; lsc, lateral semicircular canal; ls, sigmoid sinus (lateral sinus); mcf, middle cranial fossa; jb, jugular bulb. The air cells between the sigmoid sinus and the facial nerve mastoid segment (third segment) are removed, exposing and preserving the posterior semicircular canal, which will be the upper limit of the dissection (▶ Fig. 19.7). After this step a diamond bur is used to remove the residual air cells and to detect the dura of the posterior cranial fossa. The endolymphatic sac is visualized and preserved between the posterior cranial fossa and the posterior semicircular canal. The mastoid segment of the facial nerve is identified in correspondence with the digastric notch up to the stylomastoid foramen to locate where the nerve runs, so as to avoid injury to this nerve during the tumor dissection (▶ Fig. 19.7).1–5 The mastoid air cells medial to the mastoid segment of the facial nerve are gently removed, preparing a subfacial route. The dissection is carried out preserving the bony labyrinth superiorly and facial nerve anteriorly and laterally in order to reach the disease in the inferior aspect of the temporal bone.3,5 Fig. 19.7 Infralabyrinthine approach. Microscopic dissection. Left ear. a, b The mastoid cells between the sigmoid sinus, labyrinthine block, and facial nerve (inter-sinus-facial cells) are progressively removed, exposing the mastoid facial nerve and posterior semicircular canal. A diamond bur is used to better expose the jugular bulb medially with respect to the facial nerve. c A bony triangle between the posterior semicircular canal superiorly, the mastoid facial nerve anteriorly and laterally, and the jugular bulb inferiorly is delimited in this way. d A diamond bur is used, removing the air cells of the bony triangle under the bony labyrinth in order to reach the petrous apex (white arrow). ls, sigmoid sinus; eac, external auditory canal; psc, posterior semicircular canal; lsc, lateral semicircular canal; fn, facial nerve; jb, jugular bulb; isfc, inter-sinus-facial cells. This microscopic surgical step allows the surgeon to prepare the surgical field until the pathological tissue is reached, before the employment of the endoscope. The limits of the field (see ▶ Fig. 19.8) are: Fig. 19.8 Infralabyrinthine approach. Left ear. The infralabyrinthine route is prepared (white arrow), exposing the posterior semicircular canal superiorly, the mastoid facial nerve anterolaterally, and the posterior fossa dura and the endolymphatic sac posteriorly. ls, sigmoid sinus; eac, external auditory canal; psc, posterior semicircular canal; lsc, lateral semicircular canal; ssc, superior semicircular canal; mcf, middle cranial fossa; pcf, posterior cranial fossa; fn, facial nerve; dr, eardrum; ma, malleus; in, incus; end, endolymphatic sac. jb, jugular bulb. Superiorly, the labyrinth Anterolaterally, the third tract of the facial nerve Posterolaterally, the PCF dura, the sigmoid sinus, and the jugular bulb. The endoscopic access is achieved by inserting the endoscope into the subfacial recess in the access route previously created by the microscope (▶ Fig. 19.9), accessing the petrous apex medially and anteriorly to the third portion of the facial nerve and the labyrinthine block, with preservation of these structures (▶ Fig. 19.10). The use of curved vacuum instruments (dissectors) and curved vacuum suction allows the removal of the pathology from the cavity created under direct endoscopic visualization. Fig. 19.9 Infralabyrinthine approach. Left ear. Endoscopic step. After the creation of the infralabyrinthine route, a 45° endoscope is inserted into the subfacial recess. ls, sigmoid sinus; eac, external auditory canal; psc, posterior semicircular canal; lsc, lateral semicircular canal; ssc, superior semicircular canal; mcf, middle cranial fossa; pcf, posterior cranial fossa; fn, facial nerve; dr, eardrum; ma, malleus; in, incus; end, endolymphatic sac, jb, jugular bulb. Fig. 19.10 Infralabyrinthine approach. Left ear. Endoscopic dissection. a Endoscopic exploration identifies the landmarks and the anatomical structures located in the surgical field. b, c In this case a high jugular bulb is found and the space between the mastoid segment of the facial nerve and the jugular bulb is narrow (white arrow). This anatomical conformation is a relative contraindication for this surgical approach. d A 45° endoscope is used to remove the bony tissue in the subfacial recess, avoiding vessel and nerve damage. eac, external auditory canal; fn, facial nerve; jb, jugular bulb; lsc, lateral semicircular canal; psc, posterior semicircular canal. The first procedure to be performed is an endoscopic exploration searching for anatomical landmarks in the cavity that is created by the tumor. Special attention should be paid to the identification of the internal auditory canal (IAC) and to the dura layer that covers it, usually found in the upper part of the endoscopic field. Identification of the internal carotid artery is necessary when it is surrounded by the disease (▶ Fig. 19.11). The endoscopic dissection is performed in a lateromedial direction without damaging the labyrinth. Fig. 19.11 Infralabyrinthine approach. Left ear. Drawing representing the anatomical relationship between the major structures in the petrous apex during the infralabyrinthine approach. psc, posterior semicircular canal; lsc, lateral semicircular canal; ssc, superior semicircular canal; mcf, middle cranial fossa; fn, facial nerve; ma, malleus; in, incus; s, stapes; jb, jugular bulb; rw, round window; pr, promontory; ca, carotid artery; gg, geniculate ganglion; gpn, greater petrosal nerve; fn*, labyrinthine facial nerve; iac, internal auditory canal. We recommend the use of a 0° optic for anatomical orientation, changing to a 45° optic (15 cm long and 4 mm in diameter, if the surgical access allows) because the 4 mm diameter gives optimal brightness of the surgical field, minimizing the effects of the presence of blood in the surgical field. It is advisable to wash the cavity frequently to clean the blood from the operative field and to attain the best endoscopic view. Angled optics allow exploration of the entire cavity. After removal of the diseased tissue, there follows another exploratory phase (with a 45° optic) to search for and remove any residue of disease (see Clinical case 1 [▶ Fig. 19.12, ▶ Fig. 19.13]). Fig. 19.12 Clinical case 1. Right ear. a, b A mastoidectomy has been performed, creating an intralabyrinthine route. The labyrinth was isolated and preserved, and the third portion of the facial nerve and the sigmoid sinus were carefully isolated. c, d The mastoid antrum was opened and the incus preserved. psc, posterior semicircular canal; lsc, lateral semicircular canal; ssc, superior semicircular canal; mcf, middle cranial fossa; fn, facial nerve; in, incus; eac, external auditory canal; ls, sigmoid sinus. Fig. 19.13 Clinical case 1. Right ear. a–d The introduction of a 45° endoscope, through the intralabyrinthine route created, allows control of the petrous apex with removal of the pathological tissue under endoscopic control, preserving crucial structures such as the internal auditory canal, carotid artery, and posterior fossa dura. psc, posterior semicircular canal; pcf, posterior cranial fossa; fn, facial nerve; iac, internal auditory canal. At the end of the procedure the petrous apex cavity is filled with abdominal fat. Only in rare cases (when there has been a large injury of the dura) is obliteration of the eustachian tube with muscle fragments required, with obliteration of the cavity with abdominal fat and closure of the external ear canal. Obviously, in these cases there is a conductive hearing loss. This approach traditionally represents an anterior extension of the translabyrinthine approach at the expense of the cochlea without mobilization of the facial nerve. The introduction of the endoscope during this approach allows the removal of large lesions involving the entire petrous bone apex with impaired auditory function (e.g., cholesterinic granulomas, cholesteatoma) and exposure of the entire vertical portion of the internal carotid artery The traditional microscopic transotic technique avoids facial nerve mobilization and the facial nerve is left like a bridge in the middle of the surgical field; this limits the control of the internal carotid artery and the petrous apex.6–8 For this reason, the introduction of the endoscope is especially suitable for the paraclival carotid region and to control the internal carotid artery in the petrous bone apex (allowing good access to the petrous bone medially, to the vertical tract of the carotid artery anteriorly, and the inferior-medial tract of the horizontal carotid). And this is possible while avoiding any rerouting of the facial nerve and preserving the function (▶ Fig. 19.14). Fig. 19.14 Left ear. Drawing representing the main structures of the tympanic cavity and inner ear, which may be isolated during the transotic approach. lsc, lateral semicircular canal; mcf, middle cranial fossa; fn, facial nerve; fn*, labyrinthine facial nerve; fn**, intracanal facial nerve; s, stapes; rw, round window; ca, carotid artery; cp, cochleariform process; gg, geniculate ganglion; gpn, greater petrosal nerve; pe, pyramidal eminence. Petrous apex cholesteatoma involving the internal carotid artery with normal function of facial nerve Inner ear cholesteatoma with anterior extension with or without cochlear involvement (see Clinical case 2 [▶ Fig. 19.15, ▶ Fig. 19.16, ▶ Fig. 19.17]) Fig. 19.15 Clinical case 2. Left ear. Patient affected by extensive cholesteatoma involving the inner ear. a The mastoid bone was widely exposed. b, c An extended mastoidectomy was performed exposing widely the dura of the middle cranial fossa and the sigmoid sinus, d The posterior bony wall of the external auditory canal was drilled and removed. mcf, middle cranial fossa; hs, spine of Henle; eac, external auditory canal; ch, cholesteatoma; ls, sigmoid sinus. Fig. 19.16 Clinical case 2. Left ear. Patient affected by extensive cholesteatoma involving the inner ear. a, b The posterior bony wall of the external auditory canal was removed, exposing and preserving the third portion of the facial nerve. c, d The tympanic facial nerve was exposed up to the ganglion, and the retrofacial air cells were drilled. A labyrinthectomy was performed, removing the cholesteatoma from the inner ear. mcf, middle cranial fossa; ch, cholesteatoma; fn, facial nerve; ls, sigmoid sinus; ve, vestibule; jb, jugular bulb; pr, promontory; dr, eardrum. Fig. 19.17 Clinical case 2. Left ear. Patient affected by extensive cholesteatoma involving the inner ear. a, b In order to remove the cholesteatoma the labyrinthine bloc and cochlea were removed, and the internal auditory canal identified. The retrofacial cells were removed. b The facial nerve is like a bridge in the middle of the surgical field, covering the retrofacial area (white arrow). c, d A 45° endoscope is used to detect the residual cholesteatoma under the third portion of the facial nerve and close to the vestibule; the residual disease was removed using a curved suction instrument. mcf, middle cranial fossa; ch, cholesteatoma; ls, sigmoid sinus, fn, facial nerve; ve, vestibule; et, eustachian tube; iac, internal auditory canal; pcf, posterior cranial fossa. ttm, tensor tympani muscle. Middle ear tumor involving the petrous apex with normal function of the facial nerve Cholesterinic granuloma with petrous apex involvement (see Clinical case 3 [▶ Fig. 19.18, ▶ Fig. 19.19, ▶ Fig. 19.20, ▶ Fig. 19.21]) Fig. 19.18 Clinical case 3. Right ear. Preoperative CT (a, c) and MRI (b, d) images of a patient affected by recurrence of cholesterinic granuloma of the petrous apex (short arrows) of the right ear with internal carotid artery involvement (long arrows). Fig. 19.19 Clinical case 3. Right ear. a A transotic microscopic approach was adopted, exposing the entire facial nerve and the internal carotid artery. b–d A 45° endoscope was used to reach the petrous apex and the pathological tissue lying medially and anteriorly to the internal carotid artery. mcf, middle cranial fossa; ls, sigmoid sinus, fn, facial nerve; et, eustachian tube; lsc, lateral semicircular canal; sda, sinodural angle; ca, carotid artery; pea, petrous apex; gran, cholesterinic granuloma. Fig. 19.20 Clinical case 3. Right ear. a Endoscopic magnification of the relationship between the internal carotid artery and the eustachian tube. b Cholesterinic granuloma laying medially and anteriorly with respect to the vertical carotid artery. c, d A 45° endoscope was used to remove the disease from the petrous apex without carotid manipulation. et, eustachian tube; ca, carotid artery (vertical); ca*, carotid artery (horizontal); pea, petrous apex; gran, cholesterinic granuloma. Fig. 19.21 Clinical case 3. Right ear. a, b Postoperative CT scans showing the transotic endoscopic-assisted approach. In this case also we can distinguish a microscopic stage, preparing the surgical field in order to reach and remove part of the disease, and a following endoscopic stage in order to reach the pathological tissue in the depth of the petrous apex, controlling the internal carotid artery. A wide postauricular incision is made, about 3 cm posteriorly to the postauricular sulcus. The subcutaneous tissues are elevated and the external auditory canal opening is detected and transected at the bony cartilaginous junction. The lateral portion of the skin of the external auditory canal is everted in order to close the ear canal at the end of the surgical procedure (▶ Fig. 19.22). Fig. 19.22 Left ear. a, b The external auditory canal is transected and closed as a cul-de-sac. A muscoloperiosteal flap is elevated in order to uncover the occipital and mastoid bone. A traditional canal wall down extended mastoidectomy is performed; during this phase it is particularly important to identify the common anatomical landmarks—the dura of the middle cranial fossa superiorly and the sigmoid sinus posteriorly. The middle cranial fossa dura mater is more widely exposed and skeletonized inferiorly and posteriorly until the sinodural angle is exposed (▶ Fig. 19.23, ▶ Fig. 19.24). Fig. 19.23 Left ear. An extended mastoidectomy is performed with a canal wall down technique; the facial nerve is skeletonized from the stylomastoid foramen to the geniculate ganglion, and the middle cranial fossa dura and the sigmoid sinus are widely exposed. The inter-sinus-facial cells are drilled. mcf, middle cranial fossa; ls, sigmoid sinus, fn, facial nerve; et, eustachian tube; sda, sinodural angle; lsc, lateral semicircular canal; psc, posterior semicircular canal; ssc, superior semicircular canal; pr, promontory; s, stapes; cp, cochleariform process; isfc, inter-sinus-facial cells. Fig. 19.24 Left ear (microscopic steps). a A mastoidectomy is performed, exposing the middle cranial fossa superiorly and the sigmoid sinus with the jugular bulb posteroinferiorly. The third portion of the facial nerve and the labyrinthine block are exposed. b The endolymphatic duct is exposed between the posterior semicircular canal and the posterior cranial fossa dura. c The retrofacial air cells are drilled, exposing the jugular bulb. d The external auditory canal is removed. mcf, middle cranial fossa; ls, sigmoid sinus; fn, facial nerve; sda, sinodural angle; lsc, lateral semicircular canal; psc, posterior semicircular canal; pr, promontory; jb, jugular bulb; eac, external auditory canal. The sigmoid sinus is more widely exposed using a diamond bur; following it in an inferior to medial direction we are able to identify and expose the dura of the PCF near the labyrinth. The exposure of the PCF dura is continued until the endolymphatic sac is exposed between the posterior semicircular canal and the posterior dura (▶ Fig. 19.24). The dissection of the sigmoid sinus is carried further inferiorly until the jugular bulb is well exposed (▶ Fig. 19.24). The tympanic membrane, the residual skin of the external auditory canal, and the ossicles are removed. The microscopic stage is continued to expose the mastoid segment of the facial nerve, which can be done by removing the posterior wall of the external auditory canal, identifying and exposing the third segment of the facial nerve. During this step the surgeon must be careful to leave a thin bony layer around the facial nerve to protect it (▶ Fig. 19.25). Inter-sinus-facial cellular bone drilling is performed between the jugular bulb inferiorly, the dura of the PCF, and the sigmoid sinus posteromedially. This step allows access to the retrofacial recess, establishing a communication below the facial region with the cochlea and the tympanic cavity. Fig. 19.25 Left ear (microscopic steps). a, b The external auditory canal is removed, widely exposing the third portion of the facial nerve. The eardrum and the ossicles are removed. c, d Using a diamond bur, the protympanum is drilled until the vertical portion of the carotid artery is gently exposed. mcf, middle cranial fossa; ls, sigmoid sinus, fn, facial nerve; lsc, lateral semicircular canal; psc, posterior semicircular canal; pr, promontory; jb, jugular bulb; et, eustachian tube; ttc, tensor tympani canal; ca, carotid artery. Once the mastoid segment of the facial nerve is completely exposed (from the stylomastoid foramen to the second genu) the dissection of the tympanic cavity continues, exposing the second portion of the facial nerve until identification is made of the geniculate ganglion above the cochleariform process. During this procedure attention should be paid to avoiding damage to the nerve, leaving a layer of bone on the nerve sheath. The tensor tympani muscle and canal can be removed (▶ Fig. 19.26). Fig. 19.26 Left ear. a–c The stapes is removed to expose the vestibule; the canal of the tensor tendon is also removed, exposing the homonymous muscle; the cochlea is opened. d After this microscopic step, the introduction of an endoscope allows recognition of the surrounding anatomical structures. mcf, middle cranial fossa, fn, facial nerve; lsc, lateral semicircular canal; psc, posterior semicircular canal; jb, jugular bulb; ttm, tensor tympani muscle; ca, carotid artery; cho, cochlea; gg, geniculate ganglion; gpn, greater petrosal nerve. The stapes is then removed and the vestibule is identified; the promontory bone is drilled, exposing the cochlear turns (▶ Fig. 19.26). If necessary, extensive drilling of the cochlea can be performed up to identification of the bottom of the internal auditory canal. The vertical portion of the internal carotid artery is identified and exposed. The carotid artery is identified below the ostium of the eustachian tube in the protympanum (▶ Fig. 19.25). The internal carotid artery lies immediately medial to the floor of the eustachian tube; the drilling must be performed from top to bottom. If the disease lies in the petrous apex close to the carotid artery, a wide skeletonization of the vertical tract of this vessel is carried out (alternatively, if the lesion is widely extended anteriorly, it is appropriate to drill anterior to the carotid itself, to the eustachian tube region to completely isolate the artery). Depending on the extent of the disease, a labyrinthectomy may be included; this procedure allows the internal auditory canal dura to be reached (▶ Fig. 19.27, ▶ Fig. 19.28). Fig. 19.27 Left ear. If required, the labyrinthine block is removed and the semicircular canals are opened in order to reach the internal auditory canal. mcf, middle cranial fossa; ls, sigmoid sinus, fn, facial nerve; sda, sinodural angle; lsc, lateral semicircular canal; psc, posterior semicircular canal; ssc, superior semicircular canal; pr, promontory, rw, round window; cp, cochleariform process; et, eustachian tube; isfc, inter-sinus-facial cells; s, stapes. Fig. 19.28 Left ear. The labyrinthine block has been removed, exposing the dura of the internal auditory canal and the dura of the posterior cranial fossa. The retrofacial air cells are removed, connecting the mastoid with the tympanic cavity (white arrow). mcf, middle cranial fossa; ls, sigmoid sinus; fn, facial nerve; pr, promontory; rw, round window; cp, cochleariform process; et, eustachian tube; s, stapes; ca, carotid artery, jb, jugular bulb; pcf, posterior cranial fossa; iac, internal auditory canal. The surgical field is prepared for the endoscopic phase to remove any residual disease close to the medial and anterior aspect to the carotid artery. The vertical carotid artery is skeletonized microscopically (▶ Fig. 19.29) and the cochlea is opened in order to prepare the route for the endoscopic maneuvers (▶ Fig. 19.30). Fig. 19.29 Left ear. The carotid artery is gently exposed microscopically, drilling anteriorly with respect to the cochlea and medially to the eustachian tube opening. mcf, middle cranial fossa; ls, sigmoid sinus, fn, facial nerve; gg, geniculate ganglion; fn*, labyrinthine facial nerve; pr, promontory, rw, round window; cp, cochleariform process; s, stapes; ca, carotid artery; jb, jugular bulb; pcf, posterior cranial fossa; iac, internal auditory canal. Fig. 19.30 Left ear. The promontory is drilled and the cochlea is opened. The stapes is removed, exposing the vestibule. mcf, middle cranial fossa; ls, sigmoid sinus, fn, facial nerve; cp, cochleariform process; ca, carotid artery, jb, jugular bulb; pcf, posterior cranial fossa; iac, internal auditory canal; gg, geniculate ganglion; cho, cochlea. The advantage of the use of the endoscope in the open approach (transotic approach) is to allow drilling in the subcarotid space, pushing anteriorly and medially to the carotid vertical tract and caudally to the horizontal carotid tract without the need for manipulation of the arterial vessel. This procedure is indicated if the disease involves the petrous apex, extending medially and anteriorly to the carotid artery. Prior to proceeding with the dissection under endoscopic guidance, the operative field is evaluated endoscopically to obtain a good anatomical orientation. The anatomical landmarks are the cochlea, the internal carotid artery vertical tract, the tensor tympani muscle, the geniculate ganglion, and the jugular bulb (if protruding into the tympanic cavity) (▶ Fig. 19.26, ▶ Fig. 19.31). Fig. 19.31 Endoscopic steps. Left ear. Before starting the surgical approach, endoscopic orientation is necessary to identify all the anatomical landmarks. mcf, middle cranial fossa, fn, facial nerve; ca, carotid artery, gg, geniculate ganglion; cho, cochlea; pr, promontory; gpn, greater petrosal nerve; ttm, tensor tympani muscle; lsc, lateral semicircular canal. The cochleariform process and tensor tympani muscle are removed to allow a wide access to the supratubal region; the surgeon proceeds by identifying the greater petrosal nerve and following the geniculate ganglion anteriorly. This neural structure is firmly adherent to the MCF dura, which in this region is lower, and this nerve represents the cranial limit of the dissection and an important landmark for finding the internal carotid artery (horizontal tract). In fact, the greater petrosal nerve flags up the horizontal tract of the internal carotid artery and runs in a parallel and cranial course with respect to the carotid artery, going anteriorly as far as the fifth cranial nerve and anterior lacerum foramen (▶ Fig. 19.32). Fig. 19.32 Right ear. Anatomical view from above of the facial nerve, geniculate ganglion, and greater petrosal nerve. Note that the greater petrosal nerve runs parallel to the horizontal carotid artery, up to the trigeminal nerve anteriorly. fn, facial nerve; ca, carotid artery, gg, geniculate ganglion; cho, cochlea; gpn, greater petrosal nerve; ttc, tensor tympani canal; ssc, superior semicircular canal; in, incus; ma, malleus; et, eustachian tube; fn*, labyrinthine facial nerve; iac, internal auditory canal; svn, superior vestibular nerve; chon; cochlear nerve; Vn, trigeminal nerve. The greater petrosal nerve is followed endoscopically over the vertical tract of the carotid (during these maneuvers it is possible to injure to the nerve due to its fragility), and subsequently under endoscopic viewing the area between the vertical tract of the carotid artery (anteriorly), the cochlea (posteriorly), the greater petrosal nerve (superiorly), and the jugular bulb (inferiorly) is drilled (▶ Fig. 19.33, ▶ Fig. 19.34). Fig. 19.33 Endoscopic steps. Left ear. The bone between the vertical tract of the carotid artery anteriorly and the cochlea posteriorly is drilled to reach the petrous apex; the geniculate ganglion and the greater petrosal nerve have been dissected. The greater petrosal nerve represents the superior limit of the dissection, indicating where the horizontal carotid artery runs. gpn, greater petrosal nerve; gg, geniculate ganglion; mcf, middle cranial fossa; ca, carotid artery; p.apex, petrous apex. Fig. 19.34 Endoscopic steps. Left ear. a The positions of and the relationship between the carotid artery, greater petrosal nerve, and the cochlea are investigated endoscopically. b, c A bur is used to drill the bony wall between the cochlea posteriorly and the carotid artery. d The bony wall medially to the vertical carotid artery is progressively removed, exposing the petrous apex and the paraclival cells. gpn, greater petrosal nerve; ca, carotid artery (vertical); ca*, carotid artery (horizontal); cho, cochlea; jb, jugular bulb. Using a 45° endoscope, the bone medial to the vertical portion of the internal carotid artery is further broken down with a diamond drill. This procedure allows the opening of paraclival air cells near the clivus; the drilling is done from caudal to superior direction for identification of the horizontal tract of the carotid, which can be followed medially and anteriorly near the anterior lacerum foramen (▶ Fig. 19.35, ▶ Fig. 19.36).
19.1 Introduction and Classification of Endoscopic Approaches to the Inner Ear
19.1.1 Transmastoid Route
19.1.2 Retrosigmoid Route
19.2 Transmastoid Route: Micro-Endoscopic Combined Surgical Approaches (Endoscopically Assisted) to the Petrous Apex and/or IAC Fundus
19.2.1 Infralabyrinthine Endoscopically Assisted Route
Indication
Contraindications
Surgical Steps
Microscopic Step
Endoscopic Step
19.2.2 Transotic Endoscopically Assisted Route
Indications
Microscopic Step
Endoscopic Step
Ento Key
Fastest Otolaryngology & Ophthalmology Insight Engine